



The coronavirus disease 2019 (COVID-19) pandemic strained supply chains, disrupted healthcare operations, and tremendously affected the well-being of healthcare workers (HCWs). Reference Gilleen, Santaolalla, Valdearenas, Salice and Fusté1,Reference Ibar, Fortuna and Gonzalez2 The pandemic necessitated unexpected and urgent adaptations to established workflows to reduce infection risk and slow the spread of severe acute respiratory coronavirus virus 2 (SARS-CoV-2), the virus causing COVID-19. Rapidly implemented policy and practice changes led to increased utilization of protective measures and equipment, such as N95 respirators, depleting or exhausting supplies of items that are typically readily available. Lack of evidence-based information regarding the severity, susceptibility, and transmission of COVID-19 led to uncertainty and confusion. HCW stress, anxiety, and depressive symptoms increased substantially. Reference Shreffler, Petrey and Huecker3 Emotional distress among HCWs Reference Mehta, Machado and Kwizera4 was associated with fear of self-infection, fear of carrying the virus home to family and friends, Reference Cox, Miller and Jamison5 decreases in patient care quality, and stigmatization. Reference Cawcutt, Starlin and Rupp6 Fear was fueled by uncertainty regarding contagion risk and best practices for controlling an emerging virus.
Early in the pandemic, infection transmission routes were less well understood than at present; insufficient evidence existed to understand whether and to what extent SARS-CoV-2 could be transmitted from person to person by very small particles, often referred to as aerosols or droplet nuclei. In July 2020, the World Health Organization (WHO) issued a scientific brief that underscored aerosol-generating procedures (AGPs) as a source of transmission. 7 Yet the amount of virus required for transmission, sometimes called the inoculum size, and many other factors that can influence human transmission were not sufficiently studied to draw conclusions. 8 HCWs remained uncertain about the magnitude of risks associated with common patient care practices, including AGPs.
The Centers for Disease Control and Prevention has described AGPs as “… procedures performed on patients [that] are more likely to generate higher concentrations of infectious respiratory aerosols than coughing, sneezing, talking, or breathing.” 9 However, AGP definitions and criteria are evolving. More recently, AGPs have been defined as “medical procedures that can result in the release of aerosols from the respiratory tract” that are “high risk of aerosol generation and increased risk of transmission.” 10 Participation in AGPs has been documented to be a significant risk factor for transmission of highly contagious pathogens to HCWs. Reference Tran, Cimon, Severn, Pessoa-Silva and Conly11,Reference Wilson, Marks and Eckhardt12 Yet, a large gap remains in our understanding of which and to what extent AGPs confer an increased risk of respiratory pathogen transmission via small-particle aerosols from patient to HCWs performing AGPs or that are present in spaces where they are performed. Reference Klompas, Milton, Rhee, Baker and Leekha13 Insufficient evidence exists regarding which procedures or activities actually create small-particle aerosols of patient-derived material as opposed to simply being associated with increased risk for transmission via other mechanisms, such as via body fluid sprays or proximity to an infected patient. Emerging evidence suggests that proximity, duration, viral load, and room ventilation are primary risk factors for infection transmission, which may explain why procedures requiring close contact with patients increase transmission risk. Reference Harding, Broom and Broom14
Classical representations of behavior under uncertainty hold that beliefs—including perceptions—are key determinants of decisions related to money, health, life duration, and approval. Reference Savage15 Uncertainty especially affects decision making regarding health and welfare when most outcome probabilities are ambiguous and not objectively known. Reference Attema, Bleichrodt and L’Haridon16 Without clear understanding of respiratory pathogen transmission risks associated with specific AGPs, HCWs face uncertainty about how to protect themselves and others. In many instances, they resort to presuming transmission risk based on personal experience, anecdotal evidence, and historical perceptions that AGPs pose higher exposure and infection risk to HCWs.
Although risk preferences and tolerance vary across individuals, Reference Dohmen, Falk, Huffman, Sunde, Schupp and Wagner17 attitudes mediate the relationship between perceptions and behavior. Reference Reibstein, Lovelock and Dobson18 HCW risk perceptions will influence their cognitive (ie, beliefs) and affective (ie, feelings) attitudes regarding the appropriateness of conducting AGPs under various conditions. In turn, these attitudes shape their behaviors, influencing their willingness to conduct AGPs. Reference Reibstein, Lovelock and Dobson18 Furthermore, because behavior reciprocally influences attitudes, HCW decisions to conduct AGPs or not can influence their emotional state. HCWs may experience moral distress when weighing personal safety against conducting potentially life-saving AGPs, such as emergent endotracheal intubation or cardiopulmonary resuscitation. Risk uncertainty may compound distress by leaving HCWs questioning whether prioritizing personal safety (and thereby protecting their ability to provide care to others) is ethical or justified. If risk perceptions are incorrect, HCWs may either compromise their own health unwittingly or unnecessarily modify care to levels that do not meet current standards or even delay or deny care to patients in need. The resulting conundrum may further distress HCWs and exacerbate symptoms of stress, anxiety, and depression.
Given the interplay of these phenomena, we sought to elucidate what is known about HCW perceptions of AGP risk and their affective response to those perceptions. To do so, we conducted a systematic review of the published literature about HCW reactions to conducting AGPs. Here, we present the results of our review.
Methods
Between March 2 and April 10, 2021, we conducted systematic searches in PubMed, CINHAL Plus, and Scopus using combinations of the following key words and synonyms in conjunction with the controlled vocabulary of the database: “risk,” “risk perception,” “anxiety,” “stress,” “concern,” “fear,” “health personnel,” “aerosol generation,” “aerosol procedure,” and “aerosol generating procedure.” In total, 504 unique records were retrieved. We examined references in the included papers for additional studies. After those selections were added and duplicates were removed, 596 distinct records remained for screening.
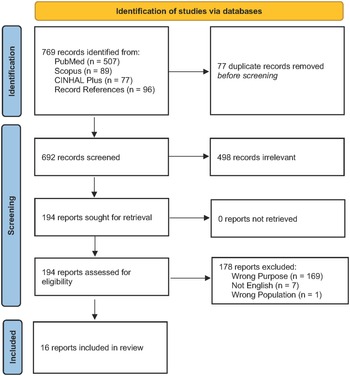
To reduce the risk of bias, titles and abstracts were screened for eligibility by 2 independent reviewers (L.E.B. and D.W.). For the purposes of this paper, we defined HCW as any type of worker whose occupation is engaged directly or indirectly in providing healthcare services to patients. Papers describing perceived risk of adverse outcomes posed to HCWs while conducting an AGP or affective (eg, cognitions, attitudes, and emotions) responses of HCWs to perceived risk were included. Articles were excluded if they did not meet these inclusion criteria (eg, articles focused on non-HCWs, such as bystanders administering CPR, were not included) or were not written in English (Fig. 1). Articles were not excluded on the basis of publication type, presence of original data, or study design. All coauthors participated in data extraction as independent reviewers. Two independent reviewers extracted data from each record. Discrepancies were discussed by all coauthors until consensus was reached.

Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flowchart
Results
Report characteristics
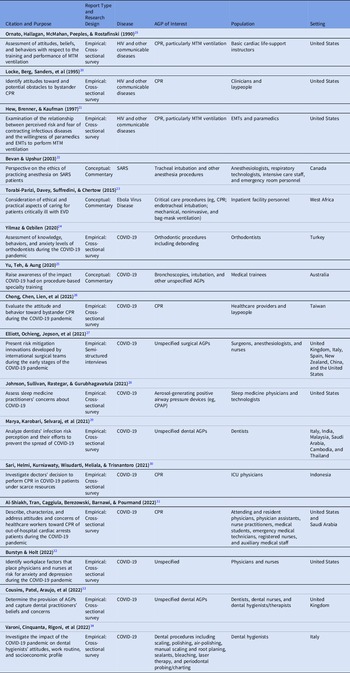
We included 16 reports in this review (Table 1). Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Varoni, Cinquanta and Rigoni34 Publication date of the reports ranged from 1990–2022. Report settings included the United States (n = 7), Italy (n = 3), the United Kingdom (n = 2), Saudi Arabia (n = 2), Australia (n = 1), Cambodia (n = 1), Canada (n = 1), China (n = 1), India (n = 1), Indonesia (n = 1), Malaysia (n = 1), New Zealand (n = 1), Spain (n = 1), Taiwan (n = 1), Thailand (n = 1), Turkey (n = 1), and West Africa (n = 1). Included reports were either conceptual (n = 3) or empirical (n = 13). Conceptual reports were published as commentaries. Also, 12 empirical reports leveraged a cross-sectional survey research design; 1 study reported results from a semistructured interview study.
Table 1. Descriptions of Selected Peer-Reviewed Publications

Note. AGPs, aerosol-generating procedures; CPAP, continuous positive airway pressure; CPR, cardiopulmonary resuscitation; EMT, emergency medical technician; EVD, Ebola virus disease; HIV, human immunodeficiency virus; ICU, intensive care unit; MTM, mouth-to-mouth; SARS, severe acute respiratory syndrome.
Disease of interest
Across the 16 reports included in this review, 4 specific diseases were highlighted: (1) human immunodeficiency virus (HIV; n = 3), (2) severe acute respiratory syndrome (SARS; n = 1), (3) Ebola virus disease (EVD; n = 1), and (4) SARS-CoV-2 (COVID-19; n = 11). Though all reports tended to refer to a single illness as the primary disease of interest, several expected their discussion to apply to communicable respiratory diseases more generally.
The diseases highlighted in the reports mirrored the contemporary epidemics or public health crises at the times of publication. For example, studies conducted in the 1990s Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Hew, Brenner and Kaufman21 focused on HIV, whereas contemporary reports generally centered on COVID-19. Reference Yilmaz and Ozbilen24–Reference Varoni, Cinquanta and Rigoni34 Similarly, Bevan and Upshur Reference Bevan and Anesthesia22 published their SARS report in 2003 and the 2015 paper by Torabi-Parizi et al Reference Torabi-Parizi, Davey, Suffredini and Chertow23 focused on EVD.
Population of interest: Types of HCWs
Reports addressed different types of HCWs in various outpatient and inpatient settings. In total, 6 reports addressed clinicians and healthcare providers (including attending and resident physicians, nurse practitioners, registered nurses), medical technicians, auxiliary medical staff, basic cardiac life-support instructors, and emergency medical technicians and paramedics providing bystander cardiopulmonary resuscitation (CPR) in community settings or inpatient settings under conditions of scarce resources. Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Hew, Brenner and Kaufman21,Reference Chong, Chen and Lien26,Reference Sari, Helmi, Kurniawaty, Wisudarti, Meliala and Trisnantoro30,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31 Also, 3 reports focused on inpatient facility personnel such as anesthesiologists, surgeons, intensive care personnel, emergency room personnel, respiratory care personnel and nurses engaged in performing procedures such as endotracheal intubation, mechanical ventilation, general anesthesia, and renal replacement therapy. Reference Bevan and Anesthesia22,Reference Torabi-Parizi, Davey, Suffredini and Chertow23,Reference Elliott, Ochieng and Jepson27 One additional report addressed medical trainees learning to perform these types of critical-care inpatient procedures such as endotracheal intubation and bronchoscopy. Reference Yu, Teh and Aung25 Furthermore, 4 reports addressed dentistry professionals including orthodontists, dentists, dental nurses, and dental hygienists and hygiene therapists. Reference Yilmaz and Ozbilen24,Reference Marya, Karobari and Selvaraj29,Reference Cousins, Patel and Araujo33,Reference Varoni, Cinquanta and Rigoni34 One report studied sleep medicine physicians and technologists, Reference Johnson, Sullivan, Rastegar and Gurubhagavatula28 and another focused generally on physicians and nurses in inpatient settings. Reference Burstyn and Holt32
AGPs of interest
The cumulative list of AGPs addressed across all 16 reports included CPR; anesthesia procedures including intubation (endotracheal, mechanical, noninvasive, and bag mask); bronchoscopies; orthodontic and dental procedures including bonding, scaling, polishing, root planning, bleaching, laser therapy, and periodontal probing and/or charting; and positive airway pressure.
Cardiopulmonary resuscitation (CPR, including mouth-to-mouth ventilation, which was recommended for use during CPR until 2008) 35 was the single most commonly explored AGP in our review. All 6 of these reports were empirical cross-sectional survey investigations of HCWs attitudes and behaviors surrounding CPR during outbreaks of infectious disease. Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Hew, Brenner and Kaufman21,Reference Chong, Chen and Lien26,Reference Sari, Helmi, Kurniawaty, Wisudarti, Meliala and Trisnantoro30,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31
The remaining reports referred to 2 or more AGPs categorized by purpose or discipline. Of these, dental and orthodontic procedures were most commonly considered (n = 4). Reference Yilmaz and Ozbilen24,Reference Marya, Karobari and Selvaraj29,Reference Burstyn and Holt32,Reference Varoni, Cinquanta and Rigoni34 One study reported attitudes regarding the use of aerosol-generating positive airway pressure devices (eg, continuous positive airway pressure [CPAP]). Reference Johnson, Sullivan, Rastegar and Gurubhagavatula28 Another report did not specify any particular AGP. Reference Burstyn and Holt32 The remaining 4 reports explored unspecified critical care, anesthesia, and surgical procedures. Reference Bevan and Anesthesia22,Reference Torabi-Parizi, Davey, Suffredini and Chertow23,Reference Yu, Teh and Aung25,Reference Elliott, Ochieng and Jepson27
Infection risk perceptions
Collectively, the included studies suggest that AGPs are perceived to place HCWs at high risk of becoming infected with respiratory pathogens (Table 2). Conceptual evidence suggests that anesthesiologists, Reference Bevan and Anesthesia22 critical care providers, Reference Torabi-Parizi, Davey, Suffredini and Chertow23 and medical trainees Reference Yu, Teh and Aung25 are at increased risk for infection with respiratory illnesses when conducting AGPs. Empirical work suggests that most sleep medicine practitioners were extremely or very concerned about transmission of an infectious disease during sleep studies. Reference Johnson, Sullivan, Rastegar and Gurubhagavatula28 Furthermore, paramedics and emergency medical technicians (EMTs), Reference Hew, Brenner and Kaufman21 basic life-support instructors, Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19 HCWs, Reference Locke, Berg and Sanders20,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31 and laypeople Reference Locke, Berg and Sanders20,Reference Chong, Chen and Lien26 all perceive an elevated infection risk when conducting CPR. Evidence from these studies also suggests that risk perception influences HCW attitudes toward and emotional response to conducting CPR during an outbreak. Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Hew, Brenner and Kaufman21,Reference Chong, Chen and Lien26,Reference Sari, Helmi, Kurniawaty, Wisudarti, Meliala and Trisnantoro30
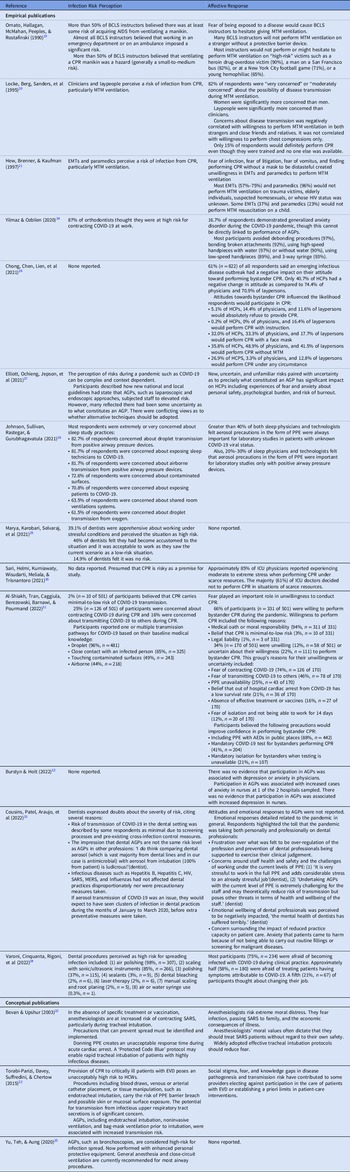
Table 2. Findings from Selected Peer-Reviewed Publications

Note. AGPs, aerosol-generating procedures; AIDS, acquired immunodeficiency syndrome; BCLS, basic cardiac life support; CPR, cardiopulmonary resuscitation; EMT, emergency medical technician; EVD, Ebola virus disease; HCP, healthcare provider; HCW, healthcare worker; MTM, mouth-to-mouth; SARS, severe acute respiratory syndrome.
Dentistry practitioners appear to have mixed views regarding the risk of transmitting an infectious disease during their practice. One study showed that 87% of orthodontists believe that they are at high-risk for contracting COVID-19 while conducting AGPs such as bonding and debonding procedures. Reference Yilmaz and Ozbilen24 Similarly, in another study, most dentists perceived air polishing and scaling with sonic and ultrasonic instruments to be high-risk AGPs related to their practice. Reference Varoni, Cinquanta and Rigoni34 Despite this finding, another study showed that 39% of dentists perceived their jobs to be high risk, 46% viewed them as low risk, and 15% felt there was no risk. Reference Marya, Karobari and Selvaraj29 Dentists cited several reasons for doubting risk severity, including the perception that dental AGPs are not the same risk level as AGPs in other professions and that the screening processes and pre-existing cross-infection control measures sufficiently protected against transmission. Reference Cousins, Patel and Araujo33
Affective response to perceptions of infection risk
Common affective responses to infection risk perceptions include fear of infection, Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Bevan and Anesthesia22,Reference Elliott, Ochieng and Jepson27,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31,Reference Varoni, Cinquanta and Rigoni34 fear of economic consequences of illness, Reference Bevan and Anesthesia22 fear of litigation, Reference Hew, Brenner and Kaufman21,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31 fear of spreading the disease to others, Reference Hew, Brenner and Kaufman21,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31 and unwillingness to perform AGPs. Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19–Reference Hew, Brenner and Kaufman21,Reference Torabi-Parizi, Davey, Suffredini and Chertow23,Reference Yilmaz and Ozbilen24,Reference Sari, Helmi, Kurniawaty, Wisudarti, Meliala and Trisnantoro30,Reference Al-Shiakh, Tran, Caggiula, Berezowski, Barnawi and Pourmand31 Performance of AGPs during an infectious outbreak can create emotional stress responses that impact the psychological well-being of HCWs Reference Elliott, Ochieng and Jepson27 and influence the decision to perform potentially lifesaving AGPs. Reference Ornato, Hallagan, McMahan, Peeples and Rostafinski19,Reference Hew, Brenner and Kaufman21,Reference Yilmaz and Ozbilen24,Reference Chong, Chen and Lien26,Reference Sari, Helmi, Kurniawaty, Wisudarti, Meliala and Trisnantoro30
Discussion
To our knowledge, this is the first review of HCW perceptions of AGP risk and affective response to conducting AGPs, including during outbreaks of high-consequence pathogens. Key takeaways of the included reports indicate that HCWs perceive increased risk to contracting a high-consequence infectious disease from participating in an AGP and that this perception stimulates a negative affective response and hesitancy to participate in the procedures. As Bevan and Upshur wrote, “Communicable diseases underscore human vulnerability and a fearful response to contagion is understandable, particularly in a context where the infectious agent is poorly understood, and the science is evolving.” Reference Bevan and Anesthesia22
However, our findings indicate a paucity of data-driven research on AGP risk perceptions and affective response. Our review demonstrates that HCWs perceive AGPs as an occupational hazard that may pose substantial personal and vocational consequences. Still, very little research has been conducted to quantify the degree of perceived risk (ie, how risky various AGPs are perceived to be). Furthermore, precision of the science is weak: numerous AGPs have been implicated as risky (eg, intubation or extubation, CPR, orthodontic bonding); however, few studies have characterized exposure and transmission risk during AGPs. The lack of sufficient empiric data to adequately characterize exposure or transmission risk of high-consequence pathogens during AGPs, or even which procedures should be considered AGPs because they generate potentially infective small particle aerosols from patients, leads to uncertainty among HCWs. This uncertainty causes anxiety, fear, and worry, potentially decreasing workforce wellness and workplace satisfaction Reference Elliott, Ochieng and Jepson27 which, in turn, may contribute to workforce attrition. Reference Mehta, Machado and Kwizera4,Reference Majeed, Irshad and Bartels36,Reference Yong37 Faced with uncertainty, many HCWs may assume an elevated risk of infection (including secondary transmission to family, friends, and coworkers), which creates a conflict between duty to care versus self-protection.
When clinical evidence informing self-protection is lacking, HCWs will likely search for ways to limit infection risk. Protection motivation theory proposes that people will protect themselves based on appraisals of threat (ie, situation severity) and coping (ie, response option). Reference Rogers38,Reference Rogers39 Threat appraisal involves an assessment of both the likelihood a situation will emerge and the severity of the situation if it occurs. Coping appraisal involves assessments that a particular behavior will reduce the threat (‘response efficacy’) and the belief that one can carry out an effective response (‘self-efficacy’). Our review underscores the concept that AGPs are generally believed to incur high infection risk. How HCWs choose to cope with this appraisal depends on what they perceive to be effective and acceptable response options and whether they believe they can and are willing to commit to those actions.
For example, HCWs rely on personal protective equipment (PPE) to prevent the spread of infection. Reference Yu, Teh and Aung25,Reference Johnson, Sullivan, Rastegar and Gurubhagavatula28 However, PPE alone is an insufficient solution. First, PPE use is rife with potential failure modes such as improperly fitted or functioning PPE and human error. Reference Gurses, Dietz and Nowakowski40 Thus, the effectiveness of PPE is highly dependent on the institutional framework for supporting proper PPE use through user training, fit testing, and provision of ample supplies. For these reasons, it is the lowest-ranked intervention to reduce hazardous exposures in the hierarchy of controls. 41 Second, donning and doffing procedures can be time intensive, creating unacceptable response lags to emergencies. Reference Bevan and Anesthesia22 Better infection controls, such as engineering controls to capture and remove infectious aerosols at the source and validated knowledge of infection risk, will facilitate the use of PPE only when necessary, reducing resource waste and time lags. Other response options, such as social distancing and reducing or eliminating certain AGPs, may not be seen as acceptable from the standpoint of patient welfare or safety, even if they are deemed effective for slowing the spread of infections. Practicing clinicians place a premium on meeting accepted standards of care. Distress may result, particularly when HCWs perceive a lack of agency and control.
Self-determination theory suggests that autonomy is 1 of 3 essential human needs underlying intrinsic motivation. Reference Ryan and Deci42 Developing a sense of autonomy and control over situations is fundamental for individuals to be able to self-regulate or maintain and internalize recommended behaviors such as respecting rules, complying with legal requirements, or adhering to medical treatment plans. Reference Ryan, Patrick, Deci and Williams43 Perception of control plays a crucial role in how people formulate judgments and make decisions about risk. Nordgren et al Reference Ryan and Deci42 differentiated between risk control (ie, command over the result) and volition (ie, command over risk exposure). Although people tend to underestimate risk outcomes which they perceive to control, Reference Nordgren, Van Der Pligt and Van Harreveld44–Reference Beisswingert, Zhang, Goetz, Fang and Fischbacher46 volition increases risk perceptions. Reference Nordgren, Van Der Pligt and Van Harreveld44 When an individual can influence their risk exposure, the risk is potentially avoidable and, therefore, voluntary. Control, on the other hand, reflects an ability to prevent negative outcomes (eg, infection) once risky behavior has been initiated. Although many people generally find voluntary risks more acceptable, Reference Starr47 regret may arise in the event of negative outcomes. Reference Nordgren, Van Der Pligt and Van Harreveld44 People tend to avoid or delay decisions they may regret, which they can anticipate and account for in the decision-making process. Yet, prompt decision making and early intervention can improve clinical outcomes. Reference Gupta, Wang and Hayek48,Reference Moscana49
Nuanced understanding of how these phenomena interrelate and unfold is critical in our mission to create safer healthcare environments for both patients and workers. As the COVID-19 pandemic has highlighted, risk perceptions powerfully influence behavioral choices. Reference Bruine de Bruin and Bennett50 The results of our review point to the need for more empirical work to thoroughly understand the interplay between HCW risk perceptions of distinct AGPs, affective responses to conducting these procedures under various conditions, and the resulting decision to participate in these procedures. Studying the intricacies of HCW perceptions regarding the volition and control they experience while conducting specific AGPs as well as the severity of the risk they believe various AGPs pose, is essential for advancing clinical practice. Results from such studies will point to methods for mitigating provider distress and better recommendations for when and how to conduct AGPs.
Our review had several limitations. The small sample size limits the power and generalizability of our findings. AGPs and pathogens of focus as well as geographical location varied significantly among the included studies. These variances, especially within such a small sample, can cloud our understanding of perceived risks and the resulting emotional response. The various pathogen types represented in our sample are not all respiratory diseases (eg, HIV), and their perceived risk during performance of AGPs, may be significantly lower than for respiratory diseases. These limitations in our results underscore the importance of rigorously designed and conducted clinical studies that distinguish and quantify occupational risks posed by AGPs, including a clear understanding of procedures that do, and do not, produce aerosols or otherwise increase the risk of airborne transmission. Natural experiments and observational studies with ambiguous clinical significance are hypothesis generating but do not sufficiently answer essential clinical questions about person-to-person transmission to resolve clinicians’ uncertainties about the risks of AGPs. Sufficiently powered, robust, prospective studies with clinical end points designed to achieve unequivocal answers for specific AGPs, pathogens, and the context in which AGPs are performed (emergent vs elective) are an important resource for those who perform AGPs.
In conclusion, the perception of AGP risk is complex and context dependent. New and unfamiliar hazards paired with uncertainty regarding what precisely constitutes an AGP and how to appropriately mitigate risk has a significant effect on HCWs including experiences of fear and anxiety about personal and others’ safety. Reference Elliott, Ochieng and Jepson27 These fears may create a psychological burden conducive to burnout. More research is needed to appropriately categorize medical procedures as AGPs, to document the actual risks to HCWs performing or in proximity to the performance of AGPs, to empower HCWs to decide when and how to safely perform these procedures, and to support HCWs experiencing a negative emotional reaction to the psychological burden of their decisions.
Acknowledgments
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. Mention of any company or product does not constitute endorsement by the US government, National Institute for Occupational Safety and Health, or Centers for Disease Control and Prevention.
Financial support
This work was supported by the National Institute for Occupational Safety and Health (grant no. NIOSH COVID IPA 10003508 to L.E.B.).
Conflicts of interest
All authors report no conflicts of interest relevant to this article.

 Open access
Open access