Introduction
Severe traumatic brain injury is common in Canada and is associated with a high morbidity and mortality rate.Reference Turgeon, Lauzier and Simard 1 , Reference Zygun, Laupland and Hader 2 Increased intracranial pressure, a frequent consequence of traumatic brain injury, is strongly associated with mortality in this patient population.Reference Giulioni and Ursino 3 To control this increase in pressure, several interventions were proposed, including cerebrospinal fluid drainage,Reference Bullock, Chesnut and Ghajar 4 barbiturate coma, 5 and decompressive craniectomy.Reference Bullock, Chesnut and Ghajar 4 Hyperosmolar solutions are also widely used as a resuscitation technique to control intracranial pressure. 5
Among hyperosmolar solutions, mannitol is the most frequently administered and is the solution recommended by clinical practice guidelines. 5 It is considered the gold standard for hyperosmolar therapy in the treatment of increased intracranial pressure. 5 , Reference Brown, Johns and Jafar 7 , Reference Sakowitz, Stover and Sarrafzadeh 8 However, concerns have been raised with regards to the diuretic properties of mannitol solutions, which may lead to volume depletion, hypotension, and secondary decrease in cerebral perfusion.Reference Sakowitz, Stover and Sarrafzadeh 8 - Reference Wakai, Roberts and Schierhout 10 Indeed, patients with severe traumatic brain injury have both increased morbidity and mortality with the occurrence of hypotension.Reference Marshall, Smith and Rauscher 11 Recently, hypertonic saline solutions have been suggested as the preferred solution in traumatic brain injury due to their volume repletion properties and their osmotic effect.Reference Mattox, Maningas and Morre 6 Hypertonic saline solutions are also considered an alternative in hypotensive trauma patients because of their volume expansion properties,Reference Vassar, Perry and Gannaway 12 leading to their increased usage, when compared to mannitol, for the management of intracranial pressure.Reference Marko 13 - Reference Wenham, Hormis and Andrzejowski 15
Six systematic reviews aiming to evaluate the effect of hypertonic saline in neurocritically ill patients have been published showing inconsistent results.Reference Barbic, Barbic and Lang 16 - Reference Wade, Grady and Kramer 21 However, these systematic reviews have important methodological flaws, notably the inclusion of studies with different designs and search strategies with low sensitivity. Furthermore, these reviews did not include the most recent publications. We conducted a systematic review of randomized controlled trials to investigate the clinical benefits and harm associated with the use of hypertonic saline when compared to any alternative solution in patients with severe traumatic brain injury.
Materials and Methods
Search strategy
We developed a standardized protocol (not published) prior to conducting this systematic review and meta-analysis. We used a three-pronged strategy to identify randomized controlled trials investigating the use of hyperosmolar solutions in patients with traumatic brain injuries. Our sensitive search strategy was created by using both key words and Medical Subject Heading (MeSH) or Emtree terms; these were connected using Boolean operators. An information specialist collaborated on the development of our search strategy. We systematically searched electronic databases, including OVID MEDLINE, EMBASE, Cochrane Central Register of Controlled Studies, Scopus, Web of Science, and BIOSIS (from their inception to July 2014). The complete search strategy for OVID MEDLINE is presented in Appendix 1. We used OpenGrey and National Technical Information Service databases to search relevant grey literature. We examined the individual references of included studies and relevant narrative reviews to identify potentially missed studies. No language restriction was applied.
Study selection
We i) selected randomized controlled trials of adults (ages 18 years and older) suffering from severe traumatic brain injury (Glasgow Coma Scale ≤8) and ii) assigned them randomly to receive either hypertonic saline or any other type of solution (e.g., mannitol, normal saline) to treat an increased or suspected increased intracranial pressure. When case-mix populations were evaluated, studies enrolling more than 80% of eligible patients with traumatic brain injury and adult patients were included in the meta-analysis. Our primary outcomes were death and control of intracranial pressure, regardless of the primary outcome of the included studies. Our secondary outcomes included neurological outcomes at discharge, length of stay in the intensive care unit (ICU) and hospital, and the occurrence of adverse events (including plasmatic osmolality and natremia). We included studies presenting mortality and/or intracranial pressure data according to treatment groups.
Two independent reviewers (EBP, JFS) screened citations based on title and abstract. Studies were then evaluated according to the information found in the full publication. Discrepancies between reviewers were resolved by discussion and revision of the source material. When consensus could not be achieved, a third party arbitrator was consulted (AFT).
Risk of bias assessment
The methodological quality was assessed using the Cochrane Collaboration’s tool for assessing the risk of bias. 22 This six-item tool classifies studies as either having a low, high, or unclear risk of bias.
Data abstraction
Two reviewers extracted data from the included studies independently using a standardized data extraction form developed by our research team. The form was piloted on three initial articles to confirm inter-rater agreement. When data were ambiguous or missing, the authors of the studies were contacted for clarification or additional data.
Data synthesis
We used the Cochrane Review Manager software (Version 5.1.6 Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration) to pool individual studies. To determine the effect of hypertonic saline solutions on mortality, outcomes were pooled using the DerSimonian and Laird method with Mantel-Haenszel random effect models. We expressed summary effect measures for mortality using risk ratio (RR) with 95% confidence intervals (95% CIs). An RR of less than one suggests a decrease in mortality in the hypertonic saline solution group. The inverse variance method was used to assess the impact of the intervention on the control of intracranial pressure. The effect measure was expressed as weighted mean differences (WMDs) with 95% CI. In order to assess the largest potential effect of hypertonic saline solution, we used the lowest mean intracranial pressure measured at least 120 minutes after the administration of the solution.
We assessed the presence of statistical heterogeneity using the I2 index.Reference Higgins and Thompson 23 We planned a priori to investigate potential sources of heterogeneity and explore the robustness of the findings by conducting subgroup and sensitivity analyses based on care setting (prehospital setting v. ICU setting); intervention (dose regimen) and comparative agent (mannitol v. isotonic fluids); and risk of bias (low v. high risk). We visually explored potential publication bias for each outcome using funnel plots.Reference Sterne and Egger 24
Results
Of the 506 records identified, 485 were excluded based on title or abstracts (Figure 1); 21 articles were considered for full-text analyses, of which 13 met our selection criteria. Two of the retrieved stud iesReference Baker, Rhind and Morrison 25 , Reference Rhind, Crnko and Baker 26 were subgroup studies of a larger trial,Reference Morrison, Baker and Rhind 27 which was already eligible for inclusion, leaving 11 included studies. Two studies met our inclusion criteria, but no data on mortality or intracranial pressure could be extracted from the publications, and we could not obtain additional data after contacting the authors.Reference Sakellaridis, Pavlou and Karatzas 28 , Reference Scalfani, Dhar and Zazulia 29 These studies were thus not included in our pooled analyses.

Figure 1 Flow diagram of studies.
Study characteristics
A total of 1,820 patients were enrolled in the 11 included studies.Reference Morrison, Baker and Rhind 27 - Reference Vialet, Albanese and Thomachot 37 All studies were published in English. Of the 11 studies, only 3 included more than 100 patientsReference Morrison, Baker and Rhind 27 , Reference Bulger, May and Brasel 31 , Reference Cooper, Myles and McDermott 32 (Table 1). All studies specified adult population; however, three studies defined adult population as 16 years of age and older,Reference Morrison, Baker and Rhind 27 , Reference Boudreaux and Brown 30 , Reference Cottenceau, Masson and Mahamid 33 and one study as 15 years of age and older.Reference Bulger, May and Brasel 31 One study randomized intracranial hypertension episodes, instead of randomizing patients.Reference Boudreaux and Brown 30 In one study, three patients (0.01% of our total population) with stroke were also included, which represented less than 15% of that study’s patient population.Reference Francony, Fauvage and Falcon 34
Table 1 Characteristics of included studies

* Including both TBI and non-TBI patients.
HSS=hypertonic saline solution; ICP=intracranial pressure; ICU=intensive care unit.
Three comparators were identified: hyperosmolar solution (mannitol or sodium bicarbonate),Reference Sakellaridis, Pavlou and Karatzas 28 , Reference Cottenceau, Masson and Mahamid 33 - Reference Ichai, Armando and Orban 35 , Reference Vialet, Albanese and Thomachot 37 iso-osmolar solution (normal saline or ringer’s lactate),Reference Morrison, Baker and Rhind 27 , Reference Bulger, May and Brasel 31 , Reference Cooper, Myles and McDermott 32 and hypo-osmolar solutionReference Shackford, Bourguignon and Wald 36 (see Table 1).
Risk of bias assessment
In general, allocation concealment was respected in most studies (63%),Reference Morrison, Baker and Rhind 27 , Reference Boudreaux and Brown 30 - Reference Ichai, Armando and Orban 35 and the randomization method was specified in slightly more than half of them (54%).Reference Morrison, Baker and Rhind 27 , Reference Bulger, May and Brasel 31 - Reference Cottenceau, Masson and Mahamid 33 , Reference Ichai, Armando and Orban 35 , Reference Shackford, Bourguignon and Wald 36 In six studies (63%), the research staff, patients, and medical staff were not blinded to the intervention studied.Reference Morrison, Baker and Rhind 27 , Reference Sakellaridis, Pavlou and Karatzas 28 , Reference Boudreaux and Brown 30 , Reference Cottenceau, Masson and Mahamid 33 , Reference Francony, Fauvage and Falcon 34 , Reference Vialet, Albanese and Thomachot 37 The information regarding blinding was missing in three studies (27%).Reference Scalfani, Dhar and Zazulia 29 , Reference Ichai, Armando and Orban 35 , Reference Shackford, Bourguignon and Wald 36 In one study (9%), an additional source of bias was identifiedReference Shackford, Bourguignon and Wald 36 : the study treatment and control groups were not comparable because the baseline Glasgow Coma Scale score was lower in the hypertonic saline solution group.
Two studies (18%) were deemed to have a low risk of bias, having respected all but one criteriaReference Bulger, May and Brasel 31 , Reference Cooper, Myles and McDermott 32 (Table 2). Due to the limited number of studies, it was not possible to undertake a sensitivity analysis according to the risk of bias.
Table 2 Risk of bias assessment

Data synthesis
Mortality
Four studies presented data on mortality.Reference Morrison, Baker and Rhind 27 , Reference Bulger, May and Brasel 31 , Reference Cooper, Myles and McDermott 32 , Reference Vialet, Albanese and Thomachot 37 One study used mannitol as a comparator.Reference Vialet, Albanese and Thomachot 37 Our meta-analysis showed that hypertonic saline was not associated with a significant reduction in mortality rate (k=4; n=1,638; RR 0.96; 95% CI 0.83 to 1.11; I2=0%) (Figure 2). Sensitivity analysis with studies comparing hypertonic saline solutions to isotonic solutions only yielded to similar results (k=3; n=1,618; RR 0.96; 95% CI 0.83 to 1.11; I2=0%).

Figure 2 Mortality associated with the use of hypertonic saline.
Intracranial pressure
Data on intracranial pressure managed with hypertonic saline solutions were available in six studies.Reference Boudreaux and Brown 30 , Reference Bulger, May and Brasel 31 , Reference Cottenceau, Masson and Mahamid 33 - Reference Shackford, Bourguignon and Wald 36 We pooled data on the best (lowest) mean intracranial pressure measurement from each study in order to capture the intervention with the greatest effect (see Table 1). We did not observe a significant better control of intracranial pressure with the use of hypertonic saline as compared with other solutions (k=6, n=532, WMD −0.39, 95% CI −3.78 to 2.99, I2=79%) (Figure 3). Excluding the study that included three patients with strokeReference Francony, Fauvage and Falcon 34 did not modify these results (k=5, n=512, WMD −0.27, 95% CI −4.41 to 3.60), nor did removing the studies that included patients <18 years oldReference Boudreaux and Brown 30 , Reference Bulger, May and Brasel 31 , Reference Cottenceau, Masson and Mahamid 33 (post hoc analyses). When we only considered studies performed in an ICU setting, we obtained similar results (k=4, n=159, WMD −0.94, 95% CI −5.46 to 3.58, I2=80%). Finally, the sensitivity analysis of studies using mannitol as control was also non-significant (k=3, n=125, WMD −1.72, 95% CI −6.71 to 3.27, I2=83%) (Figure 3).

Figure 3 Intracranial pressure associated with the use of hypertonic saline.
As for our aforementioned secondary outcomes—notably neurological outcomes at ICU or hospital discharge, length of stay in the ICU and hospital—less than three studies reported these outcomes, and a meta-analysis was not performed.
Functional outcomes
Two studies reported data on neurological outcome measured using the Glasgow Outcome Scale extended in 85% (1087/1282)Reference Bulger, May and Brasel 31 and 31% (33/107) of the patients,Reference Morrison, Baker and Rhind 27 at 6 and 4 months respectively. Pooled estimates using imputed data for one studyReference Bulger, May and Brasel 31 showed no difference between groups (RR 1.12, 95% CI 0.92 to 1.36, I2=52%). Data on the modified Rankin Scale were also collected in these two studies but could not be pooled due to the type of measures of central tendency used (median in one study).Reference Morrison, Baker and Rhind 27 No effect of the intervention based on the modified Rankin Scale was observed in both studies. The Functional Independence Measure and the Cerebral Performance Category Scale were also provided in one studyReference Morrison, Baker and Rhind 27 without showing clinical and statistical difference between groups.
Other outcomes
One studyReference Bulger, May and Brasel 31 looked at ventilator-free days, days alive out of the ICU, and days alive out-of-hospital without observing any benefit of the intervention.
Adverse events
All studies monitored osmolality and natremia. However, the monitoring was not standardized enough to allow a meta-analytic approach. Hypernatremia was observed in all studies, but no subsequent related adverse events were monitored except in one trial.Reference Bulger, May and Brasel 31 Nosocomial infections and seizures were evaluated, and no difference was observed. Renal insufficiency was noted in one study.Reference Shackford, Bourguignon and Wald 36
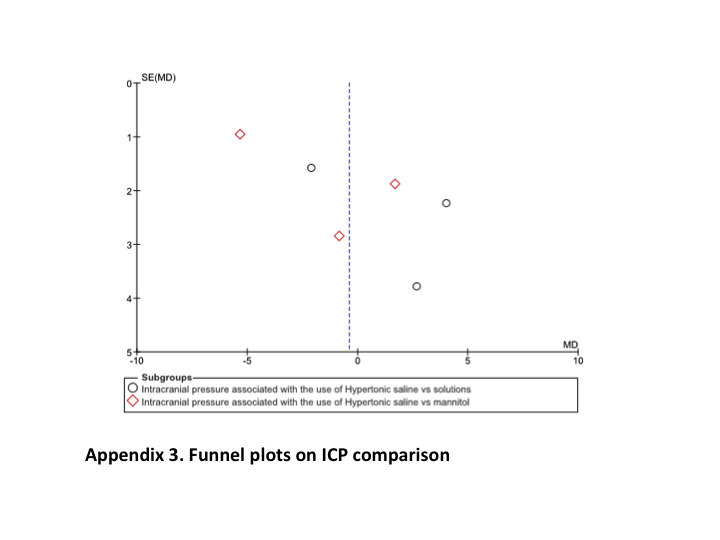
Publication bias
We performed a visual inspection of potential publication bias using funnel plots. We did not observe any obvious patterns. However, due to the small number of studies, we cannot exclude potential publication bias (see Appendix 2 for the studies on mortality and Appendix 3 for the studies on intracranial pressure).
DISCUSSION
In our systematic review, we did not observe any clinically significant benefit with the use of hypertonic saline solutions compared to other resuscitation fluids for patients with severe traumatic brain injury. Indeed, we did not observe an effect of hypertonic saline solutions on mortality or on the control of increased intracranial pressure as compared to other solutions. Mortality data were mostly from studies conducted in prehospital settings with normal saline or ringer’s lactate as the control solution. Our systematic review and meta-analysis is the largest overview on the clinical effect of hypertonic saline solution in the traumatic brain injury patient population.
Our findings support the conclusions from the most recent edition of the Guidelines for the Management of Severe Traumatic Brain Injury: Hyperosmolar Therapy (2007) by the Brain Trauma Foundation 5 and the 2008 Advance Trauma Life Support (ATLS), 38 which states that the paucity of data precludes any recommendation for the use of hypertonic saline.
Six systematic reviews evaluating the effect of hypertonic saline in the treatment of increased intracranial pressure were previously published.Reference Barbic, Barbic and Lang 16 - Reference Wade, Grady and Kramer 21 All reviews posed a different clinical question and used different inclusion criteria. One review, as with ours, concluded that hypertonic saline solution has no effect on mortalityReference Wade, Grady and Kramer 21 ; another study reporting on mortality suggested a decreased mortality with the use of hypertonic saline.Reference Barbic, Barbic and Lang 16 With regards to the five systematic reviews evaluating intracranial pressure management, they identified a reduction in intracranial pressureReference Barbic, Barbic and Lang 16 - Reference Rickard, Smith and Newell 20 associated with hypertonic saline solution, in contrast with our results. These discrepancies may be due to several factors. First, our study provides a more exhaustive review of the current evidence as compared to the previous reviews. Second, our inclusion criteria were different from previous reviews. Two reviewsReference Lazaridis, Neyen and Bodle 18 , Reference Mortazavi, Romeo and Deep 19 included all study designs (retrospective, observational, randomized controlled trials). Four reviewsReference Kamel, Navi and Nakagawa 17 - Reference Rickard, Smith and Newell 20 included several neurosurgical pathologies beyond severe traumatic brain injury (e.g., tumor, stroke). By only including randomized controlled trials of patients with severe traumatic brain injury, we achieved less clinical heterogeneity. Consequently, our review presents a comprehensive targeted review of the evidence regarding the use of hypertonic saline for patients with traumatic brain injuries.
Nonetheless, our study has some important limitations. The risk of bias of the primary studies included in our systematic review, overall, was high. Only two studies were deemed to be at low risk of bias using the Cochrane Collaboration’s tool for risk of bias assessment. Furthermore, the limited number of studies included the pooled analyses precluded or limited the performance of our planned sensitivity analyses. Consequently, several potential sources of heterogeneity and the rigor of certain findings could not be explored. Nonetheless, our systematic review followed a strict and concise protocol following the recommended methodological standards to conduct systematic reviews.Reference Liberati, Altman and Tetzlaff 39 Our systematic review and meta-analysis is currently the largest overview on the clinical effect of hypertonic saline solution in traumatic brain injury.
Conclusions
With consideration of quality of the studies included, we observed no mortality benefit or effect on the control of intracranial pressure with the use of hypertonic saline as compared to other solutions. However, only two studies were at low risk of bias. Thus, based on current level of evidence, hypertonic saline could not be recommended as a first-line agent for managing patients with severe traumatic brain injury.
Key Messages
-
∙ The use of hypertonic saline solution did not decrease mortality or improve intracranial pressure when compared to other solutions for the care of patients with severe traumatic brain injury.
-
∙ Hypertonic saline solution cannot be recommended as a first line agent in the management of patients with traumatic brain injury.
Financial support: This project was funded by the Fonds de la Recherche du Québec – Santé (FRQS) through research career awards and by the Traumatology Research Consortium of the FRQS.
Competing interests: None declared.
Supplementary Material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/cem.2016.12