



The acronym CBRN stands for “Chemical, Biological, Radiological and Nuclear” and refers to the corresponding type of hazard one may encounter. CBRN is generally used to refer to the intentional release of hazardous materials, as would be the case in a terrorist attack, while the term HazMat is used to refer to accidental release of or exposure to toxic industrial materials and substances. Reference Calder and Bland1 Per the definition of the World Health Organization (WHO), a disaster is an occurrence disrupting the normal conditions of existence and causing a level of suffering that exceeds the capacity of adjustment of the affected community, while emergencies are states in which normal procedures are suspended, and extra-ordinary measures are taken to avert disasters. Reference Khankeh and Masoumi2 In 2020, a total of 389 natural disasters were registered at The Emergency Events Database (EM-DAT), amassing 15,080 fatalities, affecting another 98.4 million people and causing $171.3 billion in damages. 3
The capacity to respond to a specific incident or accident comprehensively necessitates establishing a task force with special training, as in the current, rather traditional, type of response, medical centers are often faced with a plethora of challenges. 4 Owing to the ever-rising worldwide growth of the chemical industry, accidents and disasters caused by hazardous substances are on the rise. According to recent reports of the WHO, more than 15 million chemicals are commercially used globally, of which between 60,000 and 70,000 substances are more frequently used. Reference Wanner, Atti and Jasper5,Reference Zellner and Eyer6
Since World War II, The Iraqi armed forces used the highest volume of chemical weapons against combatants and noncombatants during the Iran-Iraq war. In 1 case, approximately 5000 Kurdish civilians were massacred in the village of Halabja in March 1988. Various agents such as mustard and a sarin nerve agent were reportedly consumed in this genocide. 7 Various credible sources have mentioned 407 civilian radiological disasters worldwide from 1944 to 2018, which resulted in 120 fatalities 3000 injuries. The atomic bombings of Hiroshima and Nagasaki in World War II, the 1986 Chernobyl accident in the north of the Ukrainian SSR in the Soviet Union, and the 2011 Fukushima nuclear accident are the more prominent examples of such disasters in recent human history. Reference Dallas, Klein and Thomas8
In the event of perceived potential harm for the affected individuals, prompt and efficient medical response, optimal triage, evacuation, and transfer and distribution management of the affected individuals are of utmost significance in enhancing the clinical conditions thereof. Reference Napi, Zaidan and Zaidan9 Given the high significance of preparedness and response management in events of nuclear disasters, hospitals and medical centers should employ highly skilled employees or train them in-house to respond to nuclear disasters with any level of efficiency. 10 Forces tasked with responding to such accidents often face extremely dangerous and demanding scenarios that may hinder their physical and mental health. Prior planning and preparation can mitigate the negative effects, enabling efficient decision-making for vital periods. 11
Razak et al. (2018) evaluated the preparedness of the emergency department against CBRN threats, arguing in the aftermath that HSE employees should be prepared for effective treatment of CBRN victims. However, emergency departments have often proven inefficient in managing casualties. Reference Razak, Hignett and Barnes12 From March to May 2020, the United States Centers for Disease Control and Prevention (CDC) received technical assistance requests from 12 countries for COVID-19 rapid response teams (RRTs) guidance, outlining the following challenges in the aftermath: (1) there were not enough response teams available for COVID-19; (2) Limited capacity to monitor the health, safety, and resilience of team members; (3) emergence of challenges in evolving conventional team processes into the specialized crisis management process, especially using remote technology platforms; (4) the stigma of team members prevented COVID-19 interventions. Reference Rodriguez13 According to the CDC, all countries have reported having established rapid response; but with varying levels of performance of COVID-19. That is, only their established standard operating procedures (SOPs) have covered all management, budgeting, staffing, maintenance, pre-deployment, deployment, and postdeployment processes. Reference Moser and Korstjens14 To alleviate the challenges of taskforces responding to COVID-19, volunteers and respondents were instructed to use just-in-time procedures instead of SOPs. Reference Moser and Korstjens14
The purpose of the current is to provide a comprehensive examination on national models of CBRN Emergency & Disaster Medical Assistance Teams (EDMATs). Given the significant in-depth knowledge of the international experiences of CBRN disaster response teams, this study sought to examine the structural components of the CBRN EDMRTs in various countries.
Methods
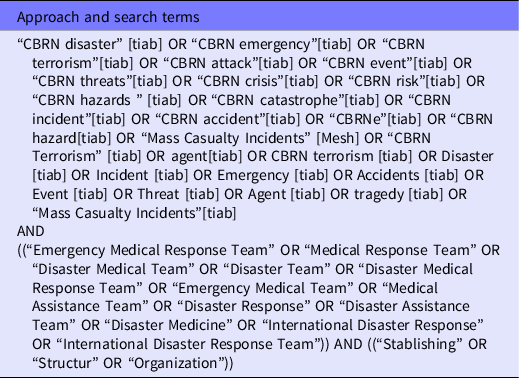
The current research is a comparative study that examined library sources, namely, articles, books, official reports, and website information, regarding CBRN EDMRTs. The study period was from November 1, 2021, to March 2022. All the texts obtained in the search process were reviewed and analyzed using content analysis. As shown in Table 1, published scientific articles regarding the establishment and deployment of RRTs were extracted using keywords-based multi-stage searching from various databases such as PubMed, CINHAL, Blackwell, Iranmedex, SID, Cochrane Database of Systematic Reviews, Google Scholar, and Scopus, as well as the websites of the Ministry of Health and other accountable organizations in different countries. Some countries did not produce any academic content regarding the matter, for which the websites of official organizations of the countries were used for information extraction. The search above procedures resulted in 35 articles, 8 books, and 3 CBRN RRT operational frameworks containing comprehensive information from teams in the United States, Australia, Japan, IAEA, NATO, and CDC.
Table 1. Search strategy
The selected structures consisted of various teams ranging from small to large teams in terms of size social to fully military structure, with different levels of responsibility in local, national, and international dimensions. Hence, each of the team structures was closely scrutinized. As a result, their structural elements were extracted and compared.
Inclusion and Exclusion Criteria
Because this study aimed to examine the effective elements in the formation of EDMRT CBRNs, all the texts deemed useful in providing complete information regarding the formation, training, and deployment of such teams were included in the study. Articles and studies missing the information above were excluded from this study.
Results
After an initial search of the relevant databases and websites, the countries or national and international organizations with a successful history of establishing CBRN EDMRTs were selected, and the required structure and elements of the teams were extracted. According to information obtained from published articles and texts, 5 prehospital radiological and nuclear response teams, namely, that of IAEA, CDC, US Department of Homeland Security, CDC Environmental Risk Unit, and NATO, and 5 prehospital CBRN response teams from Australia, NATO, the British Public Health Organization and the Japanese Red Cross Society were included for the study. The different team structures were examined and compared according to Table 2. The structure of these teams was examined and compared in Table 2. Following the extraction of the elements and components of the teams from various studies, the team composition, training, equipment, and requirements were divided into separate categories. The elements under each category were determined, which are presented in Table 2.
Table 2. A comparison of various components of CBRN teams

Discussion
The required structure and elements of CBRN EDMRTs were selected and extracted following the searching procedures on the relevant databases and websites. Based on the information obtained from published articles and texts, 9 CBRN EDMRT structures in IAEA, CDC, US Department of Homeland Security, Australia, United Kingdom, and Japan were compared and analyzed (Table 2). The elements and components of the teams were examined in 4 categories, namely, team composition, training, equipment, and requirements.
Careful planning and resource allocation are integral to any effective response that focuses on reducing the potential adverse health consequences of a CBRN-related emergency. Potential deficiency of medical support, including staff and facilities, lack of treatment strategies, and insufficient countermeasures may lead to increased risks during response. Reference Wickramarathne26 In the event of threats or incidents, these teams will be sent to areas affected yet perceivably lack the sufficient capacity to respond. It should be emphasized that these teams are not only trained for armed conflict but also are efficiently able to address natural disasters and industrial accidents where hazardous substances are present. Reference Romney27 Principles of prehospital health management in CBRN accidents include safety and PPE, zoning, command, communications, assessment (scene/casualty), triage, treatment, transportation, forensics, recovery, and rehabilitation. Reference Romney27
Elements and Components of Teams
Team Composition
A review of previous studies indicates that CBRN prehospital RRTs have different compositions and structures in countries and international institutions. The combination of radiation and nuclear teams includes operations manager, doctor, nurse, psychologist, radiation evaluator, police, public health officer, security team, emergency medical services(EMS), safety chief, resource coordination officer and coordination officer, 15–17 and epidemiologist. This person is an infection prevention and control expert, communication expert and laboratory expert, 18 and hazardous materials team, radiation specialists, National Guard support team and National Guard internal response force, 19 psychiatrist, health physicist, environmental specialist, and radiation therapy specialist. 20 Whereas the composition of CBRN teams includes a doctor, environmental medicine specialist, nurse and support Reference Heslop and Westphalen22 and identification team, decontamination team and infectious disease specialists 23 and medical incident officer, orthopedist, special care specialist, pain control specialist, triage officer, accident ambulance officer 24 and paramedics, pharmacist, psychologist, public relations and EMS. 25
As such, the authors propose establishing an efficient and specialized structure in CBRN EDMRT, under the supervision of corresponding organizations such as the Ministry of Health, Passive Defense Organization, Armed Forces, and the Fire Department, among others.
Training
Overall, the breadth of the task required in CBRN incidents is emergency services, search and rescue operations, cleaning released hazardous substances and risk assessment, and Detection, Identification, and Monitoring (DIM) procedures, regular training, and exercises at the regional and national level. Reference Morton and Johnson28
Training of radiation and nuclear teams includes Incident Command System (ICS), scene safety, triage, first aid, how to wear and remove PPE, search and rescue, decontamination, corpse management, 15–17 Interorganizational coordination, coordination of team members, progress evaluation, reporting, information evaluation, evaluation and improvement of tools, identification of vulnerable groups, increasing capacity, clinical management of patients, supply of materials, drugs, etc., overcapacity of employees, principles of prevention and control infection, detection of local rumors and misconceptions, identification of obstacles, encouraging participation in control measures, evaluation of the sampling process, sampling method, evaluation of reference laboratory capacity, 18 accident assessment, contamination assessment, risk communication, security command and control, evacuation, 19 screening, linguistic and cultural differences, transportation, registration, social acceptance centers, psychological assistance, volunteer management 20 and work with dosimeters. 21
The training of CBRN teams focused on decontamination, detection of CBRN agents, evacuation, how to wear PPE, toxicology, trauma, risk management, Reference Heslop and Westphalen22 control and command, first and advanced medical aid, clinical evaluation, and rapid antidotes, triage, risk communication, safety, demarcation, reporting by METHANE & AT-MIST-D method, evacuation chain, dead body management, 23 urban rescue, inland waterway operations, tactical medicine, infection control, quarantine, suspicious packages, call management, incident registration management, mass casualty incidents, security at the scene, 24 ethics in disasters, rapid and collaborative assessment, vaccination, search and rescue, psychosocial support, groups vulnerable are safety and security, legal issues, employee protection, waste water management, and shelters. 25
Equipment
Interventions of relief, rescue, and medical care without proper planning, preparation, and the required equipment availability lead to confusion, loss of available resources, and poor coordination between groups involved in the area. 29 Except for the CDC, which did not mention the equipment, other countries and international institutions combined the required equipment with the radiation and nuclear teams, including PPE, gloves, respiratory protection devices, boots, dosimeters, detectors, checklists, telephones. 15–17 temporary shelter, GPS, SCBA, 18 Geiger-Mueller measuring device (GM), clinical sampling equipment, 20 alarm dosimeter and manual radiation monitoring, gate monitor, and pollution control equipment 21 .
The equipment needed by CBRN teams includes PPE, Reference Heslop and Westphalen22–24 mask with activated carbon vapor filter, mask with filter for industrial toxic chemicals and biological and radioactive suspended particles, waterproof clothes with SCBA, surgical gown, medical evacuation equipment, detector, 23 potassium iodine, and personal dosimeter. 25 International CBRN medical RRTs and nongovernmental organizations do not always have the appropriate equipment and the expected ability to provide medical services appropriate to the incident, so structured, trained, and fully equipped specialized teams ensure the provision of appropriate medical services during accidents and disasters. Reference Heslop30
Requirements
The development, requirements, and limits of the prehospital RRTs in CBRN events should be established according to the experiences, demands, conditions, and grounds on which these teams are shaped. Reference Farhat, Gangaram and Castle31 The requirements of radiation and nuclear teams in the studied countries and international organizations include coordination and communication, radiation assessor, incident command post (ICP), transport of the injured, triage location, decontamination location, priority of actions, collection and isolation, registration, 15–17 experience in emergency response, team leadership and management, epidemiology experience in epidemics, familiarity with surveillance system, standards, paramedic, nurse, or doctor, experience in crisis, awareness of false beliefs and rumors related to diseases. Knowledge of leadership structures, familiarity with sampling requirements, knowledge of the location of reference laboratories, 18 radiation monitoring in 2 phases, PPE assuming a terrorist explosion, drafting warning messages, providing security for Hot Zone demarcation and entry restrictions, pollution assessment, 19 the maximum start of response in 24 to 48 h, determination of treatment and decontamination priorities, population monitoring, setting criteria, pollution level evaluation indicators, incidents with mass casualties, radiation triage groups, 20 the registration of all the persons encountered, and the entry of the implementing organizations to respond to terrorist incidents is a source of light. 21
While CBRN teams’ requirements focus on detection, identification and monitoring, warning and reporting, physical protection, risk management, medical support, vaccination, Reference Heslop and Westphalen22 start first aid as soon as possible and ideally within 10 min should be provided first and that first aid including bleeding control, basic airway management, rapid injection of antidote, oxygen supply, chest injury management (breathing) and transfer to a non-contaminated environment, psychological support, 23 mandatory use of PPE, use of plaque, if the released chemical agent is gas, there is no need for decontamination, 24 rapid diagnosis, preventive administration of potassium iodide (KI), action according to instructions, contingency plans, creation of a network of experts, levels of response: (1) strategic, (2) operational, (3) tactical, full-scale training, maintaining security, SOP, distribution of relief supplies, population movement and health promotion are focused. 25 The requirements of RRTs in the field of treatment may vary depending on the type of mission. However, overall, CBRN accidents require a risk assessment, detection, identification, and monitoring (DIM) procedures, development of mass decontamination center, injury assessment, triage, transportation of victims using a specialized ambulance, basic interventions and immediate medical treatment, advanced medical clinical care, zoning, and safe ringing. Reference Farhat, Gangaram and Castle31
Stockpile
As a source of materiel, the Strategic Logistics Depot serves as one of the medical response measures used to support the national health security response to a CBRN incident, whether natural or man-made. The strategic logistics warehouse is the most important supply and support system for medical emergencies in every country and the institution responsible for accidents and disasters. It was initially created with the realization that it would be cost-effective and logistically difficult for any locality and region to maintain their own stockpiles of critical drugs (mainly antibiotics) to deal with bioterrorism incidents and disasters. For this reason, the federal government is responsible for maintaining adequate stockpiles of key drugs, along with a rapid delivery system to receive these drugs in each region. Reference Bullock, Haddow, Coppola, Chester and Hodge32
Two important programs are the Public Health Emergency Preparedness Grant Program (PHEP), administered by the Centers for Disease Control and Prevention (CDC), and the Hospital Preparedness Program (HPP) grant program, through the Office of the Assistant Secretary for Preparedness and Response, US Department of Health and Human Services (DHHS). Specific operational plans such as the National Strategic Reserve. 29,33
Conclusions
Establishing prehospital health response teams in response to CBRN incidents is one of the tasks of health system managers, which aims to increase the capacity and capability of the prehospital system. The results of this study showed that: the structure of CBRN EDMRT with various elements such as disaster risk management system, organizations and institutions responsible for responding to CBRN disasters, risk assessment results, urgent medical needs of the affected area, increased risk for the first respondents at the scene are directly related to the high anxiety of the affected population as well as the deaths caused by the infection. Team requirements, population distribution, type of accident, level of team activity and training, equipment required by the team after the accident, according to which each country/organization should consider the above factors to design and build the structure of the CBRN EDMRT. Many disaster risk management systems are organized with a scalable structure at the local, regional, national, and international levels. To maintain the golden phase of response, timely and appropriate response to reduce the level of risk, responsible organizations and institutions should focus on capacity building/development, empowerment and resilience of available resources. For timely and appropriate response, the existence of an independent structure in the body of the health management system to organize the CBRN EDMRT seems necessary. In the end, the research team suggests that, based on a comparative study of the structures above, considering the need to determine the role and duties of the teams after announcing the accident and their presence in the affected area and observing some legal requirements in coordinating and organizing teams, a study should be conducted to design a comprehensive and evidence-based structure.
Limitations
The present study is a comparative method and in the prehospital field between different countries and institutions. For this reason, the countries and institutions included in the study had not done the exercises. To reach comprehensive patterns in each country and region, a qualitative study is needed in each region with the opinion of local experts.
Suggestions
It is recommended to install warehouses equipped with the equipment required for the prehospital field such as drugs, antidotes, PPE, detectors, etc., in each province, especially in high-risk areas for quick access. Also, due to the lack of mention of simulation exercises, it is suggested that the exercises be done in virtual reality and augmented reality to improve functional readiness.
Authors contributions
All authors were responsible for the study conception and design. All authors searched the relevant databases and included the appropriate articles according to the study objective. At the same time, Simintaj Sharififar supervised the whole thesis. All authors prepared the first draft of the manuscript. All authors performed the data analysis, made critical revisions to the paper for important intellectual content, and supervised the study. All authors have read and approved the final manuscript.
Funding
None declared.
Conflict of Interest
The authors have no conflict of interest to declare.
Informed Consent
Nil.


