



Music festival events present unique challenges to the effective delivery of health-care services. Patients present with a wide range of problems, ranging from simple presentations through to life-threatening issues, such as serotonin toxicity. After successful initial triage and immediate treatment, clinicians must make difficult decisions regarding which patients require transport to hospital as opposed to being safely able to treat on site. Determining which patients should be transported to hospital is a core responsibility for event health-care providers. Reference Stagelund, Jans and Nielsen1 A failure to transport a patient in need of critical care may be life-threatening, because although the services available on-site have grown substantially in recent years, most hospitals still retain significantly greater capacity for treatment than services at events. Conversely, inappropriate transport to hospital presents several risks, including overloading local ambulance services and emergency departments, while for patients being transported from a music festival site will separate them from their friends, supports, and property. This inconvenience is particularly frustrating in Australia where music festivals may be operated several hundred kilometers from major population centers, and consequently hospitals. At many festivals, overnight camping from cars is required, and transport to hospital may mean that patients are stranded a long way from their transport home.
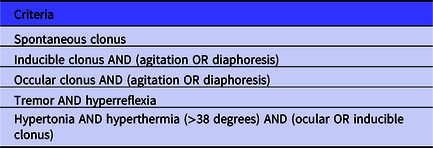
This question has come into focus in recent years in Australia, due to the emergence of serotonin toxicity as a health hazard at music festivals. The disease is caused by the ingestion of serotonergic drugs, a group which includes many stimulants taken by music festival participants (MDMA, cocaine, GHB, synthetic cannabinoids, methamphetamines) as well as several prescription medications. It is life-threatening, with symptoms including extreme fever, muscle rigidity, altered conscious states, rhabdomyolysis, and seizures. Full diagnostic criteria are found in Table 1.
Table 1. Hunter criteria for serotonin toxicity (features found in the context of serotonergic substance ingestion): serotonin toxicity present if any criteria is met Reference Dunkley, Isbister and Sibbritt2
Whereas serotonin toxicity had only rarely been seen at music festivals in Australia previously, it has been documented around the world Reference Chhabra, Gimbar and Walla3,Reference Friedman, Plocki and Likourezos4 and caused a series of presentations to event health-care providers Reference Miles, Austin and Eade5,Reference Douglas, Carew and Johnson6 and deaths at festivals in Australia. Before this threat emerged, event health-care providers had focused on providing on-site services to allow patients to recover safely. However, coronial inquests suggested that several patients who subsequently died should have been immediately transported to hospital, rather than being cared for on-site. These events demonstrated a gap in the literature regarding how to identify patients who should be immediately transported to hospital, and separately which patients could be safely cared for on-site. An empiric evidence base for making such decisions is lacking, and no evidence-based guidelines existed, meaning that, guidelines to identify which patients require transport to hospital were designed using a risk-avoidance strategy, 7 resulting in several patients being unnecessarily transported to hospital for assessment.
Hospitals often use physiology-based triage systems to identify deteriorating patients and patients who require intensive care unit (ICU) support. These scores rely on the identification of physiological abnormalities as drivers for increasing intensity of care. These commonly take the form of Medical Emergency Team (MET) calling criteria. Reference Rocha, de Castro Alcântara and Rocha8 An example system is the NSW Health “Between the flags” system, Reference Pain, Green and Duff9 presented in Table 1. The utility of these criteria in identifying patients requiring transport to hospital from a music festival has not been previously examined. There is moderate to strong evidence that MET systems triggered by physiological variables are associated with decreased mortality and cardiac arrest rates, and weak evidence that systems reduce the rate of ICU admission. Reference Laurens and Dwyer10 The benefits of the MET in terms of absolute inpatient mortality and cardiac arrest rates are still not well defined. However, MET systems empower inexperienced staff to call for immediate assistance in cases where they are seriously concerned about a patient and consequently may have a role in protecting patients in the music festival environment. MET systems have been validated in hospital inpatient populations, Reference Smith, Prytherch and Jarvis11 which tend to be dominated by older patients compared with the usual demographic found at music festivals. Reference Friedman, Plocki and Likourezos4 It is possible that a similar system would perform differently in the different patient population found at music festivals compared with hospitals.
In prehospital practice, triage systems originally developed for trauma patients are used to detect critically unwell patients with a higher risk of death. These systems are used to determine the need for urgent (lights and sirens) transport to hospital. Reference Sharma12,Reference Jiang, Jiang and Mao13 No specific evidence demonstrates that implementation of such systems reduces mortality. A systematic review demonstrated that the quality of evidence supporting such triage systems is inadequate to demonstrate impacts on patient outcomes and quality of care when considering all patients presenting to ambulance systems, Reference Lidal, Holte and Vist14 while a review focused on trauma patients found that the only physiology-based system with excellent predictive value was the combination of Glasgow Coma Scale (GCS), age, and systolic blood pressure (SBP), with an area under the receiver operating characteristic curve (AUROC) of 0.96. Single physiological predictors, such as SBP, heart rate (HR), shock index, respiratory rate (RR), and peripheral oxygen saturation (SpO2) all reported AUROCs of between 0.67 and 0.77 and were considered to have poor to fair predictive power. Reference Totten, Cheney and O’Neil15 Triage systems using physiological variables to predict the need for transport to hospital have not been comprehensively studied in the mass gathering literature.
Previous evidence has shown that first aid staff can appropriately triage patients requiring hospital transport using either a formalized process, Reference Cannon, Roitman and Ranse16 or gestalt-based decision-making. Reference Douglas, Leverett and Paul17 Most of these systems are designed for the disaster-medicine context, rather than music festivals. The role of solely physiology-based systems at music festivals has not been examined previously.
The objective of this research was to explore the value of initial physiological variables at identifying patients who were determined to require transport to hospital from music festival venues by event health-care staff. This study sought to clarify if any variable, or combination of variables, was associated with the decision to transport to hospital at music festivals.
Methods
Study Design
An retrospective observational cohort study was conducted of patients presenting for care at mass gatherings by a single organization (Event Medical Services Australia) supplying medical services in Victoria (Australia) from 2018 to 2019, using that organization’s presentation database. The study was prepared using the STROBE checklist.
Ethical Approval
The study received ethical approval from the Edith Cowan University (Joondalup, Western Australia, Australia) Human Research Ethics Committee in April 2019. The study was conducted in accordance with the Declaration of Helsinki.
Setting and Database
The audit was conducted using a database of patient presentations owned by Event Medical Services Australia. The data entry methods and abstraction from the database have previously been reported. Reference Douglas, Leverett and Paul17
Raw data were the patient care records of the organization. The database recorded the first set of observations taken after presentation. Data entry staff were trained by 1 of the investigators, who directly supervised the data entry work on an ongoing basis and was available to answer questions when required. Data were entered using a standardized template after receiving standardized training, and accuracy was monitored during entry by 1 of the investigators. Accuracy of data abstraction was not measured. A previous audit of 5% of entries demonstrated a data accuracy rate of 98.4% for all entries. Where errors were discovered, they were corrected.
Funding
The study was supported by the staff of Event Medical Services Australia who donated their time toward data entry, analysis, and writing the study. No specific monetary support was used for the project.
Participants, Inclusion, and Exclusion Criteria
Inclusion Criteria
The study included all adult (age ≥ 18 y) patients presenting to the provider for care at music festivals during the period of 2018-2019. Patients were included if a valid set of observations were taken.
Exclusion Criteria
Patients were excluded if their presentation did not require a set of observations to be taken because they undertook self-care (eg, seeking band aids, cleaning of very minor wounds, treating blisters from footwear, seeking water or sun protection). These patients were excluded because the patients would not have had their vital signs measured under the organization’s clinical practice guidelines and, hence, the information was not be available to the staff to use to make a transport decision. Additionally, it was known that these presentations had not resulted in any hospital transports, so including them would not add to the power of the study.
Variables and Outcomes
Measured variables included the patient’s presentation observations including HR, SBP, RR, peripheral oxygen saturation (SpO2), GCS score, and temperature.
The primary outcome was transport to hospital by ambulance from the event site. The outcome was analyzed for each of the physiological variables recorded. The decision for hospital transport was made by the treating paramedic or medical practitioner (doctor) in accordance with the organization’s clinical procedures. Transport to hospital generally occurred when the patient required clinical services that were beyond the capability of the on-site medical service, or where the patient was critically unwell.
At the events in question, the medical team provided a range of services including medications and fluids for drug and alcohol related presentations, plastering of suspected fractures and suturing of wounds and temperature management, as has been previously described. The team was unable to provide imaging services, and did not provide on-site care for intubated and ventilated or otherwise critically unwell patients. The team was staffed by a mixed workforce of first aid staff, paramedics, primary care doctors, and critical care doctors including anesthetists, intensive care, and emergency physicians.
Equipment
Measurement of variables was standardized over the study period. Reference Douglas, Leverett and Paul17 The physiological variables were measured either with standard clinical approaches, or using the Philips M3001A Multi-Measurement Server (Philips GMBH; Amsterdam, The Netherlands) for HR, blood pressure, and oxygen saturation.
Temperature was measured using the Braun Thermoscan 6000 tympanic thermometer (B Brauna; Melsungen, Germany). The GCS was measured by staff trained in the evaluation of this scale.
Statistical analysis was performed using SPSS Statistics v25 (IBM; Armonk, NY). The receiver operating characteristic (ROC) analysis was performed using easyROC (Hacettepe University; Ankara, Turkey).
Control of Bias
Several sources of bias were addressed. First, an attempt to reduce selection bias was made by including a large number of patients presenting across many festivals with a wide variety of staff providing services. Data and measurement error were minimized by standardizing the equipment used to gather the data. Confounding is difficult to address in the study design, but a variety of staff members were involved in making decisions, reducing the confounding introduced by practitioner variability. Other possible confounders included patient willingness to be transported to hospital, and availability of ambulance resources. Other sources of bias including time-lead bias, ecological fallacies, and Simpson’s paradox are not relevant in this design.
Sample Size Calculation
A sample size calculation assuming an AUROC for the null hypothesis of 0.5 and a desired AUROC of at least 0.7 produced a required sample size of 48 per variable considered. Multiplying this by the planned 7 ways of comparing the variables produced an overall sample size requirement of 2016. To achieve this sample size, a convenience sample of all presentations at major music festivals the provider serviced for the proceeding 2 y were selected.
Analyzed Prediction Systems
The predictive power of the initial physiological variables was analyzed in 3 ways. First, as continuous variables. Second, based on whether they exceeded a certain threshold, in line with common practice and government recommendations 7 in Australia. Third, on the assumption that having more than 1 physiological abnormality was worse than having a single abnormality, the system used in many Early Warning Score systems in use of Europe and the United Kingdom, Reference Gardner-Thorpe, Love and Wrightson18 each variable was marked as exceeding or not exceeding a commonly used cutoff and then the combination of the 5 scores was used to produce a “summary” early warning score.
Statistical Methods
The performance of each initial physiological variable in identifying presentations requiring ambulance transport to hospital was assessed using the AUROC. A prespecified threshold of 0.7 was set, in line with commonly recommended thresholds. The sensitivity and specificity were reported. The optimal cutpoint for physiological variable was determined using the Youden Index. Reference Ruopp, Perkins and Whitcomb19 In comparing the variables and combinations of variables, the method described by DeLong et al. was used. Reference DeLong, DeLong and Clarke-Pearson20 A prespecified threshold for significance was set at P < 0.05, corrected to 0.005 using a Bonferroni correction for the number of comparisons. No sub-group analyses were planned. Missing data were handled by exclusion on a case-wise basis. No sensitivity analyses were performed.
Follow-Up
The study ethical approval and local privacy regulations did not allow for follow-up of patient outcome in hospital, and did not allow the study to enquire if patients transported themselves to hospital rather than attending by ambulance.
Results
Participants
A total of 2045 patients were included and none dropped out over the study. Complete physiology data were available for 91% of presentations. The median age was 21 y, and equal proportions of males and females were enrolled. The median participant age was 21 y. A total of 75 patients were transported to hospital by ambulance from the festival site. No patients died.
Patients presented for care at 38 separate music festivals. These festivals were exclusively ticketed outdoor events, conducted during summer and early autumn, as is typical of music festivals in Australia. Thirty festivals were single-day only events, running from mid-morning to late evening, and the remaining 8 were multi-day camping events running from 3 to 5 d. Music genres were focused around electronic dance music, rock, grunge, R&B, hip hop, and country music. Alcohol and illicit drug use was common at these events, and was planned for in service provision.
Of the enrolled patients, 663 (32.4%) presented due to injuries sustained at the event site, while 894 (43.7%) had medical problems such as asthma, gastrointestinal illnesses, and allergies, 76 (19.8%) had drug- or alcohol-related problems, and 33 (1.6%) had environmental problems, such as hypothermia or heat stroke.
The triage system used to initially assess patients has been previously described. Of the included patients, 70 (3.4%) required immediate treatment of which 26 (22.9%) were transported to hospital, 344 (16.8%) required semi-urgent treatment of which 26 (7.6%) were transported to hospital, 1460 (71.4%) required routine treatment of which 23 (0.16%) were transported to hospital, and 172 (8.4%) did not have a triage code recorded of which 10 (4.1%) were transported to hospital. All patients were transported to the most appropriate local hospital by the statutory ambulance service.
The majority of patients were able to be cared for by first aid staff, with 1162 (56.8%) receiving care that did not involve a health-care professional, while 883 (43.2%) were seen by a paramedic, nurse, or doctor or combination of these team members.
Predictive Value of Initial Physiological Variables Analyzed as Continuous Variables
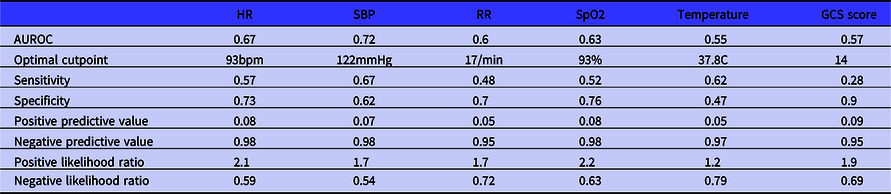
Each variable is reported as the area under the receiving operator characteristic curve, expressed as a proportion and 95% confidence interval. The AUROC for HR was 0.67 (0.60-0.74). The optimal cutpoint was 93 bpm. The AUROC for SBP was 0.72 (0.66-0.76). The optimal cutpoint was 122 mmHg. The AUROC for RR was 0.60 (0.53-0.68). The optimal cutpoint was 17 bpm. The AUROC for SpO2 was 0.63 (0.57-0.69). The optimal cutpoint was 93%. The AUROC for temperature was 0.55 (0.48-0.61). The optimal cutpoint was 37.8°C. The AUROC for GCS was 0.57 (0.48-0.61). The optimal cutpoint score was 14. Full details of the sensitivity, specificity, positive and negative values, and likelihood ratios are found in Table 3.
Table 2. Between the flags criteria for UCR and MET call for adults

Abbreviations: AVPU, Alert, Voice, Pain, Unresponsive; BP, blood pressure; HR, heart rate; RR, respiratory rate; SpO2, peripheral oxygen saturation; UCR, urgent clinical review.
Table 3. ROC analysis for predictors as continuous variables
Trigger Systems
No variable, either singly or in combination with others, exceeded the prespecified threshold for AUROC when analyzed using commonly accepted binary cutpoints. The binary cutpoints were also combined together to explore if this approach would increase their predictive power. While the predictive power of the combination did increase, it did not reach the prespecified threshold of acceptable AUROC and further demonstrated only poor sensitivity and marginal specificity.
The AUROC for each variable cut at a threshold is outlined in Table 4, alongside the relevant performance statistics.
Table 4. ROC analysis for predictors using binary cutpoints


Figure 1. ROC curve for each predictor analyzed as a continuous variable.

Figure 2. ROC curve for binary cutpoints for predictors.

Figure 3. ROC curve for the combination of binary cutpoints of predictors.
Discussion
These data are the first to examine the predictive value of initial physiological observations alone or in combination to predict the decision for hospital transport from music festivals. The data do not support the use of initial physiological variables as the sole determinant for transport to hospital, on the basis that the values are insufficiently sensitive or specific either alone or in combination.
The fact that none of the strategies of continuous measurement other than SBP, and none of the cutpoints or combinations of cutpoints reached the prespecified threshold for adequate prediction supports this point. Further reinforcing this finding is that the optimal cutpoints for most of the variables fell in the normal physiological range for adults. The potential utility of SBP with an optimal value of 122 mmHg as a transport predictor is important to consider. It was the only variable that exceeded the prespecified threshold. However, a SBP of 122 mmHg falls well within the normal range for adults and would not be considered abnormal by most clinicians. This is reflected in SBP’s poor sensitivity and positive predictive value. The finding can be explained because this sample included a group of patients with serotonin toxicity. Most patients with serotonin toxicity are hypertensive, and often require transport to hospital. Their inclusion likely drove the predictive power of SBP. A higher cutpoint may be more useful, but this was not able to be demonstrated in these data. On its own, a SBP of more than 122 mmHg is of very limited utility in identifying patients who require transport to hospital.
The performance of the variables was similar to previously reported data in hospital settings at identifying the need for ICU admission. 21 Implementation of MET systems have been associated with reductions in cardiac arrest in low quality trials, but have not been shown to definitively improve patient outcome in randomized controlled trials, and do increase health-care use and, hence, cost. Reference Rocha, de Castro Alcântara and Rocha8,Reference Smith, Prytherch and Jarvis11,Reference Jansen and Cuthbertson22 On the basis of these data, it is likely that mandating the transport to hospital of will increase use of ambulance resources and increase costs without improving patient outcome.
The reason the initial physiological variables performed poorly is likely related to the complex nature of transport decisions at music festivals, and the increasingly complex on-site services being offered at event sites. Services have become increasingly sophisticated in the Australian context, with reports emerging from multiple providers of intensive care level treatment of life-threatening syndromes such as serotonin toxicity. Reference Douglas, Carew and Johnson6,Reference Wing, Johnson and Fowler23,Reference Holbery-Morgan, Carew and Bourke24 Teams now incorporate a wide variety of health-care professionals and deliver complex intervention sets. As such, it is likely that some patients with significantly deranged physiology may now be successfully recovered on-site, avoiding the need for hospital transport and reducing the predictive value of physiological markers for this question. Reference Douglas, Carew and Johnson6 In this study, the services provided on site were relatively complex and plans had been developed to treat selected patients with serotonin toxicity on-site rather than transporting all patients to hospital. Reference Douglas, Carew and Johnson6 The capacity to treat patients with abnormal initial physiological markers may explain the low specificity for many markers seen in this analysis.
The low sensitivity and positive predictive values, in combination with the relatively high specificities and negative predictive values suggest that using the variables as the sole determinant of the transport decision would result in few false positive transports, but many missed patients who would have usually been transported to hospital. This arrangement is only safe if there are alternative systems to detect patients needing transport to hospital, and further reinforces the role for senior clinical decision-makers to be present at music festivals.
Patients may be transported to hospital for a wide variety of reasons ranging from the immediately life threatening (eg, serotonin toxicity) to relatively simple (eg, surgical closure of wounds or the need for radiological imaging such as an x-ray to exclude bone fracture). These presentations are unlikely to have abnormal physiology, and are consistent with the low sensitivity and observed optimal cutpoints in the data. Transport decisions made by clinicians likely incorporate many factors, of which the patient’s presenting physiology is only 1 of several considerations. The findings are consistent with other studies and systematic reviews of decision-making regarding transport to hospital in ambulance environments. Similarly in presentations involving trauma the utility of physiological predictors to identify patients at risk of needing interventions is low, and must be supplemented by provider experience and situational factors. Reference Totten, Cheney and O’Neil15 Likewise, this problem exists in the wider prehospital context, where there is a very poor evidence base for any triage system to predict patient- or system-level outcomes of interest. Reference Lidal, Holte and Vist14
Clinical Interpretation
Given the observed poor performance of the initial physiological markers, it appears reasonable to conclude that the decision to transport a patient to hospital should be made through using more information than the patient’s physiological variables at presentation. Incorporating information such as the cause of the patient’s presentation, likely diagnosis, trend of stability or deterioration over time, and need for specialized treatment is likely to produce a more accurate decision on the need to transport the patient to hospital than simply examining the initial physiology. In many ways, this describes the role of senior clinicians in event health care, especially in differentiating between stable and critically unwell patients. These data support a role for senior clinical decision-makers to be present at music festivals, rather than junior staff. Clinical guidelines for event health care should reflect this understanding. Support from senior decision-makers considering a range of factors should result in both fewer patients requiring transport from an event are missed, while also avoiding substantial loads on ambulance services and emergency departments and inconvenience and dislocation for patients.
Limitations
These findings are drawn from a retrospective analysis rather than a controlled experiment and, therefore, may be subject to unrecognized confounding. In addition, the scope of the audit is specific to 1 single organization in 1 country, and as such, results may not be broadly generalizable to other providers or contexts. This study also included all patients presenting for care, which included patients who had problems that could not managed at the event site (eg, complex wounds or fractures), but who did not have abnormal physiology. These patients will have reduced the predictive value of the trigger systems. It is likely that a specific analysis examining serotonin toxicity would yield different results. Unfortunately, this sample included an insufficient number of patients with serotonin toxicity to conduct such an analysis with adequate statistical power.
Future Directions
There is a need to develop clear, clinically relevant and well validated decision support tools regarding transport to hospital for the event health-care environment. Ideally such tools would be validated across multiple providers, festival types, and geographical locations to control sources of unmeasured confounding. With a larger patient group, the opportunity to explore physiological variables over time rather than simply at the time of presentation may emerge. A particularly useful area of focus would the development of physiological trigger points for transport for patients reporting ingestion of serotonergic or sympathomimetic drugs.
Conclusions
Physiological variables measured at the time of presentation alone are poor predictors of the decision to transport a patient to hospital from a music festival, either alone or in combination. Transport decisions are complex and should incorporate more information than patient presentation physiology. There is an urgent need for validated transport decision support tools for music festival health-care service provision. Development of validated guidelines regarding transport decision should reduce the impact of events on local ambulance services and hospitals while substantially decreasing both risk and inconvenience for patients.
Author contributions
N.D.: Conceptualization, study design, ethical approval, data collection, data analysis, manuscript drafting and review, publication. J.D.: Conceptualization, data collection, data analysis, manuscript review. J.C.: Conceptualization, study design, data collection, data analysis, manuscript review. K.B.: Conceptualization, data collection, data analysis, manuscript review. E.E.: Conceptualization, data collection, data analysis, manuscript review. M.G.: Conceptualization, data collection, data analysis, manuscript review. J.L.: Conceptualization, data collection, data analysis, manuscript review. J.Pa.: Conceptualization, data collection, data analysis, manuscript drafting and review. L.H.M.: Conceptualization, study design, data collection, data analysis, manuscript review, publication. J.Pr.: Conceptualization, data collection, data analysis, manuscript review. E.B.: Conceptualization, study design, manuscript drafting and review, publication. E.S.: Conceptualization, study design, ethical approval, data collection, data analysis, manuscript drafting and review.
Funding statement
The study received no direct funding.








 Open access
Open access