


On April 21, 2017, the Department of Health and Human Services (HHS) and the Centers for Disease Control and Prevention (CDC) released updated pre-pandemic planning guidelines entitled Community Mitigation Guidelines to Prevent Pandemic Influenza – United States, 2017. Reference Qualls, Levitt and Kanade1 These guidelines replaced the 2007 interim pre-pandemic community mitigation planning guidance. 2 The updated guidelines encourage state, tribal, local, and territorial (STLT) public health officials to plan and prepare for implementing non-pharmaceutical interventions (NPIs) early in an influenza pandemic in community settings to help slow the spread and decrease the impact of an influenza pandemic. NPIs are 1 of the 15 Public Health Emergency Preparedness and Response Capabilities that serve as national standards for public health preparedness planning. 3 The 2017 guidelines delineate NPIs into 2 categories: (1) NPIs recommended at all times (i.e., for both seasonal influenza and influenza pandemics); and (2) NPIs reserved for influenza pandemics. Categories of the recommended NPIs at all times include personal protective measures for everyday use (voluntary home isolation of ill persons, respiratory etiquette, and hand hygiene) and environmental surface cleaning measures (routine cleaning of frequently touched surfaces and objects). During an influenza pandemic, these NPIs will be recommended regardless of the pandemic severity level. Categories of NPIs reserved for influenza pandemics include personal protective measures (voluntary home quarantine of exposed household members, and use of face masks in community settings when ill), and community measures aimed at increasing physical distancing (temporarily closing or dismissing schools, limiting face-to-face contact in workplaces, and postponing or cancelling mass gatherings). During an influenza pandemic, these additional personal and community NPIs might be recommended depending on the overall pandemic severity and local conditions.
Local decisions about the selection and timing of NPIs reserved for influenza pandemics will require flexibility and modification as a pandemic progresses and new information and data become available. The 2017 guidelines include examples of surveillance data that could be used to trigger the implementation of NPIs during an influenza pandemic. Reference Qualls, Levitt and Kanade1 In 2019, as part of ongoing pandemic influenza planning and preparedness activities, we evaluated how STLT public health officials intended to put the updated recommendations for NPIs reserved for influenza pandemics into practice in their communities. We assessed: (1) the feasibility and acceptability of and barriers to implementing the updated recommendations for NPIs reserved for influenza pandemics from the perspective of state, territorial, and local public health officials who are tasked with pre-pandemic planning, preparation, and decision-making for their respective communities; and (2) the availability and usefulness of influenza surveillance data in their jurisdictions for triggering implementation of NPIs.
Methods
Study population
The states/territories’ assessment comprised all 50 US states, the District of Columbia, 8 US territories and freely associated states (American Samoa, Guam, US Virgin Islands, Northern Mariana Islands, Puerto Rico, Federated States of Micronesia, Republic of the Marshall Islands, and Republic of Palau). The sampling frame for selecting LHDs comprised a universe of 2454 LHDs – the total population of LHDs used by the National Association of County and City Health Officials (NACCHO) in their distribution of the National Profile of Local Health Departments Survey. 4 Information on the size of the population served, US Census region, and degree of urbanization of the LHDs was obtained from the NACCHO Profile data. 4 After excluding 470 LHDs serving a population of fewer than 10000 (which collectively serve about 2 percent of the total US population), 822 LHDs were sampled from 47 states. Hawaii and Rhode Island were excluded because these states did not have LHDs, and Florida was excluded as all data collection instruments distributed to LHDs in Florida must receive pre-clearance review and approval from the state health department in an effort to reduce response burden. A stratified random sample was selected from 12 strata based on the size of the population the LHD served (small = 10000 to 49999; medium = 50000 to 499999; and large = 500000 and above) and the census region in which the LHD resided (Northeast, Midwest, South, and West). The CDC and The MayaTech Corporation determined that the project did not meet the definition of human subjects’ research. Data were collected under OMB Approval Number 0920-0879.
Assessment tool
The questionnaire covered the following 4 topic areas: background information on respondent; status of pre-pandemic planning; feasibility and acceptability of implementing NPI recommendations during a severe influenza pandemic; and availability and usefulness of influenza surveillance data for deciding when to trigger the activation of NPIs (questions are provided in Supplementary Material Table S1). A total of 8 individuals from state and local health departments across the United States piloted the questionnaire in November 2018. Feedback from the pilot test resulted in minor modifications.
The topic area of feasibility and acceptability included the following 8 NPIs: voluntary home quarantine, use of face masks by ill persons, temporary childcare facility closures, preemptive K-12 school closures (up to 2 weeks, up to 6 weeks, and up to 6 months), temporary closures of colleges and universities, social distancing measures at schools (e.g., dividing classes into smaller groups of students and rearranging desks so students are spaced at least 3 feet from each other), social distancing measures at workplaces (e.g., offering telecommuting, replacing in-person meetings with telephone or video conferences, staggering work hours), and social distancing measures at mass gatherings (e.g., modifying, postponing, or canceling large events). The questions had 4-point Likert response scales for feasibility and acceptability (high, moderately high, moderately low, low, do not know/not sure). If a respondent entered moderately low or low for feasibility or acceptability of an NPI, a text box was provided to explain the reason for their response and to describe the barriers.
Participants were provided with definitions of feasibility, acceptability, and barriers: Feasibility is ‘the extent to which the NPI recommendation is capable of being implemented in a severe pandemic in your jurisdiction,’ Acceptability is ‘the extent to which community stakeholders and partners are willing to comply with the implementation of the NPI recommendation in a severe pandemic in your jurisdiction,’ and Barriers are ‘factors that may make difficult or impede the implementation of the NPI recommendation in a severe pandemic in your jurisdiction.’ Guidance was provided regarding what constituted a severe pandemic: Pandemic scenarios include ‘mild to moderate’ like the 2009 H1N1 pandemic; ‘moderate to severe’ like the 1968 H3N2 pandemic; ‘severe’ like the 1957 H2N2 pandemic; and ‘very severe to extreme’ like the 1918 H1N1 pandemic. A weblink to the 2017 Community Mitigation Guidelines was also provided.
The topic area of availability and usefulness of influenza surveillance data for their jurisdictions included 3 indicators of clinical severity of influenza (influenza-associated hospitalizations, total deaths attributed to influenza, and influenza-associated deaths among those < 18 years old) and 5 indicators of the level of influenza activity or spread (patient visits to outpatient health care providers for influenza-like illness [ILI], proportion of respiratory specimens that test positive for influenza virus, weekly level of geographic spread of influenza, absenteeism rates due to ILI in childcare facilities, K-12 schools, or colleges and universities, and number of laboratory-confirmed influenza cases among students, teachers, and staff). The questions on the usefulness of influenza surveillance indicators had a 5-point Likert response scale (extremely useful, very useful, moderately useful, slightly useful, not at all useful, do not know/not sure).
Data collection
Data were collected during the period from July to December 2019. An initial recruitment email was sent to public health emergency preparedness directors in the 59 state and territorial jurisdictions requesting their participation. An automated email was subsequently sent via SurveyMonkey (Momentive, San Mateo, CA) with a link to the web-based questionnaire, with 3 follow-up email messages delivered 1 week apart to non-responders, resulting in 30 responses. After phone calls and up to 3 rounds of personalized emails were sent to non-responders, an additional 14 responses were obtained. The final response rate was 75% (44/59), with 39 states and 5 territories responding.
The same web-based questionnaire was sent to LHD preparedness coordinators and local health officials. A total of 4 reminder email notices were sent to non-responders, resulting in 190 responses. To increase the response rate, 3 additional follow-up emails were sent. Outreach efforts included an informational email to the State Associations of County and City Health Officials to inform their constituents and remind them to complete the assessment, and messages to relevant groups via e-mail, an e-newsletter, and social media. These efforts yielded approximately 16 additional responses for a final response rate of 25% (206/822).
Analysis
The responses to the questions on feasibility were recoded to high feasibility (high feasibility + moderately high feasibility) and low feasibility (moderately low feasibility + low feasibility). Similarly, responses to the questions on acceptability were recoded to high acceptability (high acceptability + moderately high acceptability) and low acceptability (moderately low acceptability + low acceptability). A feasibility score was computed by summing the responses for the 8 NPIs after assigning each NPI a score of 1 for high feasibility and a score of 0 for low feasibility. To avoid the disproportionate effect of K-12 school closures/dismissals on the score, the response to closures/ dismissals of up to 2 weeks was included in the score (the responses to closures/ dismissals of up to 6 weeks and up to 6 months were excluded). A similar process was used to compute an acceptability score.
As the LHDs were selected using stratified random sampling and the LHD response rate was low, sampling, and non-response weights were generated using the 12 sampling strata. Among the 206 responding LHDs, 19 LHDs that provided background information but did not respond to any of the other topic areas were classified as non-responders for the purpose of computing non-response weights. PROC SURVEYFREQ, PROC SURVEYMEANS, and PROC SURVEYREG in SAS (version 9.4) (SAS Institute Inc., Cary, North Carolina, USA) were used to compute weighted percentages, weighted means, and weighted linear regression coefficients. A finite population correction factor was applied to 95% confidence intervals. For the qualitative responses on barriers (open-ended items), content analyses were conducted manually using dual-rater review.
Results
The state/territorial health department respondents comprised mainly disaster/ emergency preparedness coordinators (41%), state public health officials (18%), and epidemiologists (18%). The LHD respondents were mainly local public health officials (66%) and disaster/ emergency preparedness coordinators (14%). The locations of the LHDs were urban for 43%, suburban for 38%, and rural for 19%. Among the urban LHDs, the jurisdiction size was large for 15%, medium for 55%, and small for 30%; among the suburban and rural LHDs, about a fourth were medium and 75% were small (none were large).
The proportion of the state/ territorial respondents who reported that they were aware of or had read the 2017 guidelines were 93% and 82%, respectively; the corresponding proportions for the LHD respondents were 71% and 44%. Regarding incorporation of the 2017 guidelines into their pandemic influenza preparedness plans, the responses of state/ territorial respondents were as follows: completed, 16%; in progress, 54%; not started, 23%; don’t know, 7%. The corresponding LHD responses were 9%, 42%, 18%, and 31%, respectively. The proportion of LHDs indicating that incorporation of the 2017 guidelines was completed or in progress was 58% for those located in urban areas, 50% for those in suburban areas, and 38% for those in rural areas.
The majority of the state/ territorial respondents stated that feasibility of implementation was high for the following NPIs: voluntary home quarantine (68%), use of face masks by ill persons (77%), pre-emptive closures of childcare facilities (61%), pre-emptive closures of K-12 schools for up to 2 weeks (70%), pre-emptive closures of colleges and universities (73%), social distancing at schools (68%), social distancing at workplaces (64%), and social distancing at mass gatherings (73%) (Figure 1). However, feasibility was perceived to be substantially lower for K-12 school closures of up to 6 weeks or 6 months (41% and 16%, respectively). For the LHDs, about 30% to 45% of respondents indicated that they did not know what the feasibility was across all NPIs (Figure 1). However, the response pattern was similar with substantially lower feasibility for K-12 school closures of up to 6 weeks or 6 months compared to the other NPIs. The findings for acceptability were generally like those for feasibility (Figure 2).

Figure 1. Perceived feasibility in state/territorial and local health department jurisdictions of implementing non-pharmaceutical interventions during a severe influenza pandemic, 2019. Abbreviations: SC, school closure; SD – school, social distancing at schools; SD – workplace, social distancing at workplaces; SD – gathering, social distancing at mass gatherings (e.g., modifying, postponing, or canceling large events). Notes: No. of observations for state/territorial and local health department jurisdictions are 44 and 187, respectively (unweighted). Percentages for local health department jurisdictions are weighted.

Figure 2. Perceived acceptability in state/territorial and local health department jurisdictions of implementing non-pharmaceutical interventions during a severe influenza pandemic, 2019. Abbreviations: SC, school closure; SD – school, social distancing at schools; SD – workplace, social distancing at workplaces; SD – gathering, social distancing at mass gatherings (e.g., modifying, postponing, or canceling large events). Notes: No. of observations for state/territorial and local health department jurisdictions are 44 and 187, respectively (unweighted). Percentages for local health department jurisdictions are weighted.
The feasibility and acceptability scores for the LHDs are shown in Table 1. The feasibility scores were significantly higher for urban (regression coefficient 1.02, P < 0.05) and suburban (regression coefficient 1.13, P < 0.05) LHDs compared to rural LHDs. The acceptability scores were also higher for urban and suburban LHDs than for rural LHDs.
Table 1. Perceived feasibility and acceptability of implementing non-pharmaceutical interventions during a severe influenza pandemic, by urbanicity of local health department, 2019

Abbreviation: CI, confidence interval.
Notes: Number of observations (n) are unweighted. Means and regression coefficients are weighted.
a Feasibility and acceptability scores, each ranging from 0 to 8, were computed by summing the responses to 8 questions on feasibility and the corresponding 8 questions on acceptability (excluding the questions on school closures for up to 6 weeks and school closures for up to 6 months) (high = 1; low = 0; do not know/ not sure/ blank = missing). Jurisdictions with missing responses on all 8 questions (43 for feasibility and 45 for acceptability) were excluded. Information on urbanicity was missing for 2 jurisdictions.
b Linear regression models were run separately for feasibility score and acceptability score (dependent variables). The independent variables in the models were urbanicity and census region. Jurisdiction size was dropped from the models because of collinearity with urbanicity.
c P < 0.05.
The barriers to implementing NPIs are presented in Supplementary Material Tables S2-S13. Among state/ territorial and LHD respondents that rated the feasibility and acceptability of implementing NPI recommendations as moderately low or low, the financial impact of the recommendations on individuals, businesses, and the community was a recurring theme of barriers reported. Barriers to prolonged school closures (up to 6 weeks, up to 6 months), indicated that the financial burden was particularly tied to employment issues (e.g., inability to miss work, limited childcare options, and inability to telework); other barriers included loss of school meals for vulnerable children and disruption of education.
Other recurring themes included difficulty in enforcement, perceived level of disease threat, and concerns regarding political implications. Compliance and enforcement were cited as barriers for all NPIs except for K-12 school closures. Perceived level of threat (disease severity, and likelihood of becoming ill) was mentioned as a barrier for quarantine and closure of childcare facilities, K-12 schools, and colleges/universities. Concerns regarding political implications of certain NPIs (quarantine, use of face masks, and canceling or postponing mass gatherings) included issues such as perceived infringement upon personal freedom/civil liberty, mistrust of the government, and public resistance to canceling or postponing popular events.
Figure 3 shows the availability of influenza surveillance data that might provide information for triggering implementation of NPIs. For the states/ territories, about 50% of the jurisdictions reported having near real-time data on outpatient ILI visits, geographic spread of influenza cases, proportion of specimens positive for influenza, influenza-associated hospitalizations, and influenza deaths in children; about a third reported having near real-time data on total influenza-associated deaths; and about 10% reported having near real-time data on ILI-related absenteeism and influenza cases in schools. For the LHDs, about 30% to 40% reported that they did not know whether near real-time data were available for the surveillance indicators for their jurisdiction. For the state/ territorial and LHD respondents who had near real-time data, most of the respondents indicated that the indicators were extremely useful or very useful for deciding when to trigger the activation of NPIs in their jurisdictions (Tables 2 and 3).

Figure 3. Availability of surveillance data in state/territorial and local health department jurisdictions for triggering implementation of non-pharmaceutical interventions during an influenza pandemic, 2019. Abbreviations: ILI, influenza-like illness; DK, don’t know. Notes: No. of observations for state/territorial and local health department jurisdictions are 44 and 187, respectively (unweighted). Percentages for local health department jurisdictions are weighted.
Table 2. State/territorial health department perceptions of usefulness of surveillance data for deciding when to trigger implementation of non-pharmaceutical interventions during an influenza pandemic, by timeliness of data, 2019
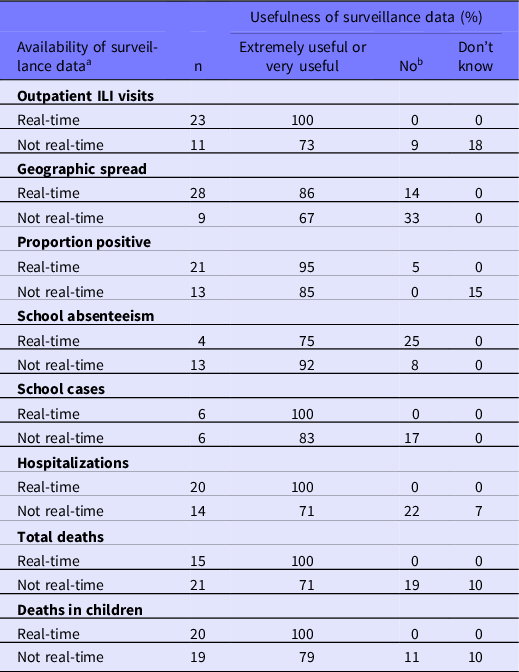
Abbreviations: ILI, influenza-like illness
a Among 44 jurisdictions, those that reported that surveillance data were available in ‘real-time’ or ‘not real-time’ are included in this table (those that reported ‘no’ or ‘don’t know’ are excluded).
b No: Moderately useful, Somewhat useful, or Not at all useful.
Table 3. Local health department perceptions of usefulness of surveillance data for deciding when to trigger implementation of non-pharmaceutical interventions during an influenza pandemic, by timeliness of data, 2019

Abbreviations: ILI, influenza-like illness
Notes: Number of observations (n) are unweighted. Percentages are weighted.
a Among 187 jurisdictions, those that reported that surveillance data were available in ‘real-time’ or ‘not real-time’ are included in this table (those that reported ‘no’ or ‘don’t know’ are excluded).
b No: Moderately useful, Somewhat useful, or Not at all useful.
Discussion
Most of the state/territorial respondents stated that the feasibility and acceptability of implementing the NPIs reserved for influenza pandemics were high, except for prolonged K-12 school closures. The LHD respondents also indicated that feasibility and acceptability were lowest for prolonged school closures. The feasibility and acceptability scores were lower for LHDs located in rural areas than those in suburban or urban areas. Recurring themes pertaining to the barriers included financial impact, compliance and difficulty in enforcement, perceived level of disease threat, and concerns regarding political implications.
Our findings on perceived NPI acceptability, feasibility, and barriers are consistent with those of previous studies. A study conducted in 2006 indicated that most individuals would comply with community mitigation recommendations during a severe influenza pandemic. Reference Blendon, Koonin and Benson5 A national survey of adults during the 2009 H1N1 influenza pandemic showed high public approval for government recommendations related to school closures (80%), wearing masks in public (71%), and avoiding places where many people gather (69%). Reference SteelFisher, Blendon, Ward, Rapoport, Kahn and Kohl6 A survey of public health officials in 50 US states and 8 territories and freely associated states in 2015 indicated that 85 percent of the jurisdictions had or did not need the legal authority to temporarily close child care facilities, K–12 schools, and colleges /universities, or cancel mass gatherings. Reference Naik, Vagi, Uzicanin and Dopson7 About 68% of state/territorial respondents in our evaluation indicated that feasibility of social distancing in K-12 schools was high. A previous report indicated that within-school social distancing practices were generally more feasible for elementary schools than secondary schools; for reduced-schedule practices, shortening the school week for the entire school was more feasible than shortening the school day. Reference Uscher-Pines, Schwartz and Ahmed8 Our evaluation found that feasibility and acceptability were lowest for prolonged K-12 school closures, and that barriers included parents’ inability to work and loss of income, missing school meals, and continuity of education. A previous study reported that the social and economic effects of school closures include loss of income for parents who may have to stay home to take care of their children, difficulties sustaining teaching and learning, and loss of school meals for underprivileged children who rely on free or reduced-price school lunches. Reference Cauchemez, Ferguson and Wachtel9 Another study reported that a substantial proportion of adults would face severe financial problems if they had to stay home from work for several weeks to comply with community mitigation recommendations, with a disproportionate effect for persons with lower incomes and racial/ ethnic minorities. Reference Blendon, Koonin and Benson5 A study found that working adults would be less able to comply if they were unable to work from home or did not have paid sick leave. Reference Blake, Blendon and Viswanath10
We found that feasibility and acceptability scores were lower for LHDs located in rural areas. This finding is consistent with a previous report that that social distancing orders were issued less often in rural areas in response to communicable disease outbreaks. Reference Katz, Vaught and Simmens11 Evaluations conducted in 2020 during the coronavirus disease 2019 (COVID-19) pandemic reported higher use of cloth face coverings in urban compared to rural areas, Reference Czeisler, Tynan and Howard12 and lower adoption of stay-at-home orders in states with higher proportion of rural residents. Reference Gigliotti and Martin13
We found that availability of influenza surveillance data was lowest for ILI absenteeism rates and influenza cases in schools. This may be because these 2 indicators are not a part of the US Influenza Surveillance System. Reference Brammer, Blanton and Epperson14 School absenteeism data collected by school districts are not standardized and rarely include information about the illness that caused the absence. Reference Enanoria, Crawley, Tseng, Furnish, Balido and Aragon15 Lack of data on ILI absenteeism and influenza cases in schools may hamper the ability to decide when to trigger proactive school closures. Reference Germann, Gao and Gambhir16 Recent research suggests that routine school systems for student absenteeism monitoring could be feasibly modified to close this gap and provide early warning on increases of influenza activity in schools and surrounding communities. Reference Temte, Barlow and Goss17
A survey of LHDs in 2015 indicated that the most common concern about the use of social distancing (including quarantine, isolation, school closures, and work closures) was the magnitude of public health impact; other concerns included legal, political, financial, and sociocultural issues, and the impact to vulnerable populations. Reference Katz, Vaught and Simmens11 A survey administered in 2015 to 62 Public Health Emergency Preparedness directors in the 50 US states, 8 US territories and freely associated states, and 4 cities indicated that the most important factors for selecting and triggering the implementation of NPIs during an influenza pandemic were severity of illness, transmissibility, and populations most affected. Reference Naik, Vagi, Uzicanin and Dopson7 Other important factors were CDC and subject matter expert recommendations, geographic spread of the disease, disease impact in relation to available mitigation resources, and vaccine availability.
Our evaluation has some limitations. First, although we requested that respondents consult with colleagues, if necessary, the responses may not be reflective of the perspective of the entire health department. Second, the LHD response rate was low. Although we used non-response weights to align the responding sample to the original sample in terms of jurisdiction size and census region, the findings may not be generalizable. In addition, a substantial proportion of LHD respondents indicated that they did not know the feasibility and acceptability of the NPIs, which may reflect lower awareness and familiarity with the 2017 guidelines. Finally, because we did not have the names of the jurisdictions in the state/ territorial and LHD analytic datasets to preserve respondents’ confidentiality, we could not conduct an in-depth assessment of geographic variability.
Our data collection was completed just 1 month before the first cases of COVID-19 were reported in China and the disease subsequently spread around the world. Due to the severity of the COVID-19 pandemic, NPIs that were implemented during the spring of 2020 in the United States included stay-at-home orders, business closures, and preemptive K-12 school closures for several months. Reference Gigliotti and Martin13,Reference Tolbert, Kates and Levitt18–Reference Zviedrite, Hodis, Jahan, Gao and Uzicanin20 Most K-12 public schools that closed offered distance learning and meal services for students Reference Zviedrite, Hodis, Jahan, Gao and Uzicanin20,21 and about 45 percent of the general population worked from home instead of their normal workplaces. 22 The US government provided economic assistance to American workers and businesses, and required covered employers to provide paid sick leave or expanded family and medical leave if an employee was unable to work because of COVID-19 illness or quarantine or to take care of a quarantined family member or a child whose school or child care provider was closed. 23,24
About 43 percent of US public school districts, as of 2016, had pandemic preparedness plans that included procedures for ensuring the continuity of education during unplanned school closures. Reference Kersten, Chamberlain, Jones, Uzicanin and Ahmed25 Although most schools developed emergency remote learning systems during the COVID-19 pandemic, learning loss has been reported. Reference Zviedrite, Hodis, Jahan, Gao and Uzicanin20,Reference Donnelly and Patrinos26,Reference Slavin and Storey27 The annual occurrence of prolonged unplanned school closures (≥ 5 school days) before the COVID-19 pandemic further supports the need for the timely development of effective high-quality distance learning tools. Reference Jahan, Zviedrite, Gao, Ahmed and Uzicanin28 Distance learning strategies require several components to be successful, including a learning management system, policies to address student access to devices and to the Internet, and high-quality online course content, as well as adaptation of content to student learning needs, and training and support for teachers to deliver instruction online. Reference Schwartz, Ahmed, Tamargo, Uzicanin and Pines29 K-12 teachers who transitioned to distance learning during the COVID-19 pandemic reported that support would have been helpful in the following areas: previous training on learning management system, student internet and computer access, more time to prepare for distance learning, better guidance on platforms and tools to use, and teaching resources available for distance learning. Reference Francom, Lee and Pinkney30
Concerns regarding political implications of select NPIs emerged as 1 of the perceived barriers in our evaluation, almost as a premonition on the part of the respondents of the situation that soon ensued in many US jurisdictions. While the majority of the population in the United States adhered to the facemask recommendations during the COVID-19 pandemic, a small but vocal minority – often with a particular political alignment – did not, leading at times to anti-mask actions. Reference Taylor and Asmundson31 Lower government trust and greater COVID-19 pseudoscientific beliefs were associated with lower adherence to facemask use and other social distancing measures. Reference Gratz, Richmond and Woods32 Reasons for anti-mask attitudes included political beliefs that mask mandates were infringing on personal liberty; some even claimed that facemask recommendations were primarily politically driven to control the thinking and behavior of the people. Reference Taylor and Asmundson31,Reference He, He and Reynolds33 Harassment and threats directed to LHD officials were reported. Reference Ward, Stone, Mui and Resnick34 Anti-mask attitudes subsequently converged with the anti-vaccine stance, often in the same population groups, and at times escalating into protests both in US jurisdictions and in other industrialized nations. Reference Kelleher35,Reference Doherty36
Conclusion
To our knowledge, our assessment is the first national-scope investigation to systematically evaluate perceived NPI feasibility, acceptability, and barriers and the availability and usefulness of influenza surveillance data for timely and appropriately triggering implementation of NPIs during influenza pandemics by surveying all state/ territorial health departments and a random sample of LHDs. The results of our assessment were intended to help inform NPI implementation considerations 2 years after release of the 2017 community mitigation guidelines. Reference Qualls, Levitt and Kanade1 The findings, in conjunction with observations during the COVID-19 pandemic, can provide insights for future pandemic planning and preparedness. The prolonged disruptions of in-person learning associated with the COVID-19 pandemic illustrates a need for high-quality, well-established distance learning programs before a new pandemic strikes. Proactive strategies to systematically address perceived barriers and promote disease prevention ahead of a new pandemic, are needed to increase receptivity and consistent adoption of both NPIs and other evidence-based countermeasures, most notably vaccines. The experiences during the COVID-19 pandemic, which strained healthcare systems during periods of intense transmission, and resulted in over 18 million excess deaths worldwide as of December 2021, underscore the importance of public trust and adherence to NPIs as the first line of defense in influenza pandemics, and a key element in the control of future emerging infectious diseases. Reference Qualls, Levitt and Kanade1,37–39
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/dmp.2022.174
Acknowledgments
We would like to acknowledge the contributions of the project’s stakeholder engagement group consisting of representatives from the Association of State and Territorial Health Officials (ASTHO), Council of State and Territorial Epidemiologists (CSTE), National Association of County and City Health Officials (NACCHO), and the National Public Health Information Coalition (NPHIC); MayaTech’s internal evaluation support team: Jamie Weinstein, Barbara Draley, and Mitch Wang, and their subject matter expert, Barbara Goldrick; and fellow CDC project team members: Neha Kanade, Jasmine Kenney, and Tiffani Phelps. We also would like to acknowledge that the data collection for the local health department assessment was implemented by NACCHO under the direction of Debra Dekker (PhD) and her team.
Funding
This project was fully funded by Centers for Disease Control and Prevention (MayaTech: Task Order 0001, Contract 200-2014-59291; NACCHO: Cooperative Agreement Grant No. 6 NU38OT000306-01-01).
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.








