



Introduction
Serious bacterial infection (SBI) is one of the leading causes of mortality in the ICU and accounts for 16.7% of mortality [Reference Shane and Stoll1, Reference Tsai, Chu, Hsu, Lien, Huang, Chiang, Fu, Lee and Huang2]. Owing to the poorly developed immune system, the neonatal population in the ICU is considered the high-risk group to suffer from infections [Reference Steiner, Diesner and Voitl3, Reference Baier, Pirr, Ziesing, Ebadi, Hansen, Bohnhorst and Bange4]. Early identification of SBI might be contributed to favourable treatment outcomes; however, there are few obvious clinical symptoms and signs to indicate SBI in neonates [Reference Dorney and Bachur5]. Therefore, it is a challenging task for the early diagnosis of neonatal SBI in the ICU.
Routine blood examination is an easy and common way used to examine infectious diseases [Reference Zhu, Chen, Wang, Zhang, Lu and Sun6]. Some studies have reported a high diagnostic accuracy of routine blood parameters in infectious diseases [Reference Mentis, Garcia, Jiménez, Paparoupa, Xirogianni, Papandreou and Tzanakaki7, Reference Tschoellitsch, Dünser, Böck, Schwarzbauer and Meier8]. Mentis et al. confirmed that routine blood parameters can be effectively used for the diagnosis of meningitis [Reference Mentis, Garcia, Jiménez, Paparoupa, Xirogianni, Papandreou and Tzanakaki7]. Tschoellitsch et al. [Reference Tschoellitsch, Dünser, Böck, Schwarzbauer and Meier8] found that machine learning methods based on routine blood examination can reliably diagnose pneumonia. In addition, combined routine blood parameters, such as neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio, have been used as markers for the diagnosis of infectious diseases [Reference Liu, Li, Peng, Xiang, Xia, Wu, Yang and He9, Reference Carpio-Orantes, García-Méndez and Hernández-Hernández10].
In the neonates admitted to ICU, the diagnostic value of routine blood parameters in SBI was also reported [Reference Guo and Sun11, Reference Yang, Liu, Yue, Wang, Yang and Yang12]. Guo et al. [Reference Guo and Sun11] reported that red cell distribution width (RDW) was an important factor to diagnose SBI in neonates in the ICU. Moreover, neutrophil and white blood cell counts (WBC) were identified as effective markers for the early diagnosis of neonatal SBI in the ICU [Reference Yang, Liu, Yue, Wang, Yang and Yang12]. Although these markers have been reported, the diagnostic value of routine blood parameters for SBI in neonates admitting to the ICU needed to further explore.
In this study, we aim to develop a diagnostic model for neonatal SBI based on routine blood parameters using the data from the Medical Information Mart for Intensive Care III (MIMIC-III) database.
Methods
This study on the diagnostic model was reported according to the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) statement [Reference Collins, Reitsma, Altman and Moons13].
Study design and data source
This was a cross-sectional study, and data were extracted from MIMIC-III. MIMIC-III was a large and single-centre database, comprising clinical data on patients admitted to the ICU in the Beth Israel Deaconess Medical Center in Boston, Massachusetts [Reference Johnson, Pollard, Shen, Lehman, Feng, Ghassemi, Moody, Szolovits, Anthony Celi and Mark14]. The clinical data were collected based on laboratory measurements, medications, vital signs, length of hospital stay, survival, and so forth. This database supported applications including academic research, higher education coursework, and quality improvement initiatives. Our study was not required to sign the informed consent because MIMIC-III was a publicly available database.
Participants
Neonates (<28 days) admitted to the neonatal intensive care unit (NICU) ≥ 24 hours were included in this study, and neonates of missing data on routine blood examination were excluded.
Variables for diagnostic model
Candidate variables
Data were extracted within 24 hours after neonates were admitted to the NICU based on demographic characteristics (gender, weight, race, premature delivery, and cesarean section delivery) and routine blood examination (monocyte, mean corpuscular volume (MCV), haemoglobin (HGB), RDW, WBC count, lymphocyte count, neutrophil count, and platelet count)], and systemic immune–inflammatory index (SII). SII was a new marker of inflammation, which was calculated by the combination of platelet, neutrophil, and lymphocyte counts (that is platelet counts × neutrophil counts/lymphocyte counts) and reflected the balance between inflammatory and immune statuses [Reference Güngör, Göktuğ, Yaradılmış, Güneylioğlu, Öztürk, Bodur, Karacan and Tuygun15]. Premature birth was categorised into extremely preterm (< 28 weeks), very preterm (28 to 32 weeks), moderate preterm (32 to 34 weeks), and late preterm (34 to 37 weeks) [Reference Blencowe, Cousens, Chou, Oestergaard, Say, Moller, Kinney and Lawn16].
Dependent variable
The dependent variable was SBI. According to the previously reported study [Reference Vandenberk, de Bondt, Nuyts, Toelen and Verbakel17], SBI was defined as suffering from one of the following diseases: pyelonephritis, bacteraemia, bacterial meningitis, sepsis, pneumonia, cellulitis, and osteomyelitis. These diseases were identified from the medical record.
Development and internal validation of the model
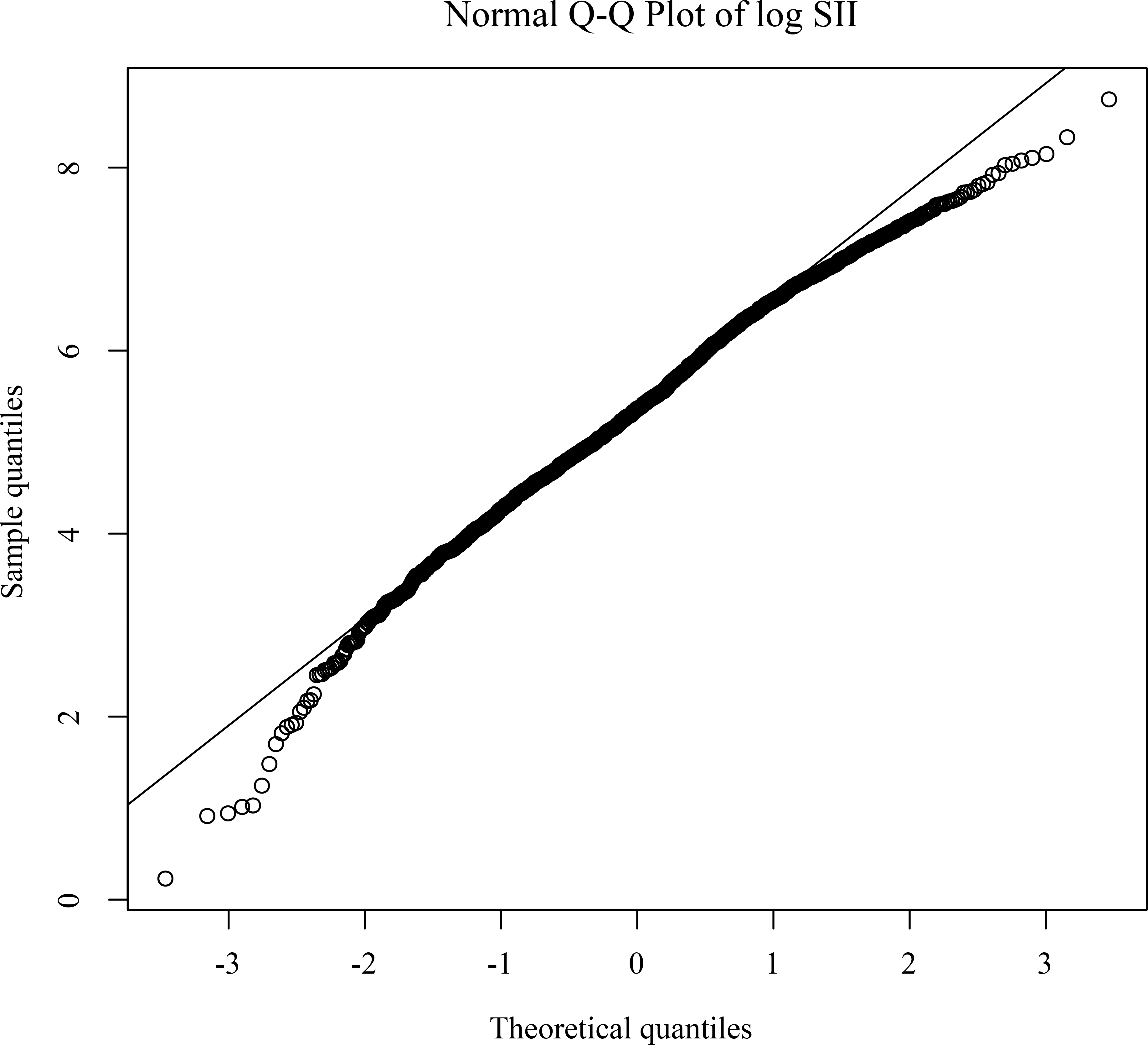
This diagnostic model was developed using the logistic regression method. Participants were divided into training set and testing set in a ratio of 7:3. Variables with a statistical significance in the univariate logistic regression analysis were selected to develop the model. Considering that SII was reported as an effective marker to diagnose SBI in age groups where the immune system was immature [Reference Güngör, Göktuğ, Yaradılmış, Güneylioğlu, Öztürk, Bodur, Karacan and Tuygun15], SII was also included in the model. Quantile–quantile (Q-Q) plot was used to graphically assess whether the dataset was in a normal distribution [Reference Vetter18], and SII in skew distribution was normalised using logarithm method (log SII) (Supplementary Figure S1A,B).
The performance of this model was evaluated by calculating the area under the curve (AUC), accuracy, specificity, sensitivity, positive predictive value, and negative predictive value (NPV). Calibration was evaluated using a visual calibration plot. This diagnostic model was internally validated using 10-fold cross-validation. The discrimination capacity in each of the 10-fold cross-validation subsamples was calculated, and the mean cross-validated AUC was reported. The diagnostic result of this model was visualised using a nomogram.
Statistical analysis
Continuous data in normal distribution were described as mean ± standard deviation (mean ± SD), and differences between the two groups were compared using an independent sample t-test. Continuous data in skew distribution were described as a median and interquartile range [M (Q1, Q3)], and differences between the two groups were compared using Mann–Whitney U rank-sum test. The categorical data were described as number and percentage [N (%)], and differences between the two groups were compared using a chi-square test. Missing data were processed by deletion. Univariate logistic regression analysis was used to select factors to develop the diagnostic model, and the results were reported as odds ratio (OR) and 95% confidence intervals (95% CI). Statistical analysis was performed using SAS 9.4 (SAS Institute Inc., Cary, NC) and R (version 4.0.3, Institute for Statistics and Mathematics, Vienna, Austria), and the statistical significance was displayed by P < 0.05.
Results
Participants
A total of 4,022 neonates admitted to the NICU ≥24 hours were extracted from the MIMIC-III database. Of these, 1,879 neonates missing data on routine blood examination were excluded (1,842 neonates missing data on lymphocytes, 11 neonates missing data on platelets, 21 neonates missing data on HGB, and 5 neonates missing data on RDW). Further, 263 neonates missing data on weight were excluded. Finally, 1,880 neonates were included for analysis, with 179 neonates in the SBI group and 1,701 neonates in the non-SBI group (Figure 1). There was 55.90% of males in the included participants. A significant difference was observed in weight, premature delivery, monocyte, MCV, HGB, WBC, and platelets between the SBI group and non-SBI group (Table 1).

Figure 1. The flowchart of participant selection.
Table 1. Characteristics of neonates with and without SBI

Abbreviations: HGB, haemoglobin; MCV, mean corpuscular volume; RDW, red blood cell distribution width; SBI, serious bacterial infections; SII, systemic immune–inflammation index; WBC, white blood cell.
Model development and performance
Supplementary Table S1 shows that weight (OR = 0.43, 95%CI: 0.34–0.53), premature delivery (extremely preterm: OR = 27.34, 95%CI: 12.72–58.74; very preterm: OR = 2.74, 95%CI: 1.25–6.04), monocyte (OR = 1.33, 95%CI: 1.13–1.57), MCV (OR = 1.09, 95%CI: 1.06–1.11), HGB (OR = 0.64, 95%CI: 0.53–0.77), and WBC (OR = 1.83, 95%CI: 1.20–2.79) were associated with SBI. Therefore, the diagnostic model was developed based on weight, HGB, MCV, WBC, monocyte, premature delivery, and log SII (Supplementary Table S2). The AUC of this model was 0.805 (95%CI: 0.759–0.852) (Table 2). At a cut-off value of 0.082, the maximum specificity and sensitivity were 0.809 (95%CI: 0.787–0.831) and 0.719 (95%CI: 0.641–0.797), respectively (Figure 2). The calibration plot demonstrated that the predictive probability of SBI fitted well with the actual probability (Figure 3), indicating good calibration of our model.
Table 2. Performance of the diagnostic model for neonatal SBI based on routine blood examination

Abbreviations: AUC, the area under the curve; CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value; SBI, serious bacterial infections.

Figure 2. ROC curve of the training set.

Figure 3. Calibration plot of the diagnostic model for the probability of SBI in ICU neonates.
The performance of this model was verified by internal validation using the testing set, and the AUC was 0.812 (95%CI: 0.737–0.888) (Table 2), indicating a good discrimination capacity of this diagnostic model. In addition, the 10-fold cross-validation in the full dataset showed that the mean AUC within the 10 folds was 0.818 (95%CI: 0.814–0.821) (Supplementary Table S3).
Nomogram
A diagnostic nomogram was developed based on the factors in the diagnostic model. A total score was obtained by summing up the single score of each factor and used to estimate the probability of SBI. For example, a patient with a weight of 1.78 kg, moderate preterm, 6 * 103/uL of monocyte, 126 fL of MCV, 17.5 g/dL of HGB, 15.8 K/uL of WBC, and log SII in 5.49 had a total score of 350 points, with 11.7% of probability to diagnose as SBI (Figure 4).

Figure 4. Nomogram for the diagnosis of SBI in ICU neonates.
Discussion
Neonates are the high-risk group to suffer from SBI due to their immature immune system, which raises the risk of disability and death in the world [Reference Shane and Stoll1, Reference Steiner, Diesner and Voitl3]. Some studies have reported the potential diagnostic utility of routine blood parameters in infectious diseases [Reference Mentis, Garcia, Jiménez, Paparoupa, Xirogianni, Papandreou and Tzanakaki7, Reference Tschoellitsch, Dünser, Böck, Schwarzbauer and Meier8]. In this study, we developed a diagnostic model based on routine blood parameters for SBI in neonates admitted to the ICU. Weight, HGB, MCV, WBC, monocyte, premature delivery, and log SII were used to develop the model. Results showed that the model performed well in the diagnosis of SBI for neonates admitted to the ICU. The model was visualised using a nomogram, which may be convenient to use and be helpful for clinicians to improve treatment recommendations.
SII was an integrated parameter based on platelet, neutrophil, and lymphocyte counts, which gained extraordinary popularity as a routine blood-based marker in the clinic since Hu et al. introduced it in 2014 [Reference Hu, Yang, Xu, Sun, Sun, Guo, Zhang, Wang, Qiu, Zhou and Fan19]. As an integrated indicator, SII might be better to reflect the balance between host inflammatory and immune status [Reference Güngör, Göktuğ, Yaradılmış, Güneylioğlu, Öztürk, Bodur, Karacan and Tuygun15, Reference Hu, Yang, Xu, Sun, Sun, Guo, Zhang, Wang, Qiu, Zhou and Fan19]. Previous studies have reported the clinical values of SII in cancers, coronavirus disease 2019 (COVID-19), and urinary tract infections [Reference Fu, Yan, Tan and Liu20–Reference Gu, Huang, Zhang, Qian, Cao and Ge23]. SII also showed usability in age groups where the immune system was immature [Reference Güngör, Göktuğ, Yaradılmış, Güneylioğlu, Öztürk, Bodur, Karacan and Tuygun15]. Güngör et al. [Reference Güngör, Göktuğ, Yaradılmış, Güneylioğlu, Öztürk, Bodur, Karacan and Tuygun15] found that SII was a predictor for urinary tract infections in infants. In our study, SII was identified as an important factor to diagnose SBI in neonates. Although the diagnostic performance of SII might be dissimilar in different age groups, diagnosed diseases, and severity of diseases, its advantages in a straightforward calculation from hemogram results and not requiring additional costs and further blood collection cannot be ignored [Reference Güngör, Göktuğ, Yaradılmış, Güneylioğlu, Öztürk, Bodur, Karacan and Tuygun15].
WBC, HGB, MCV, and monocyte were also used to develop the model. WBC is the main immune cell in human bodies and has been reported to diagnose bacterial infections and assess the severity of diseases effectively [Reference Honda, Uehara, Matsumoto, Arai and Sugano24, Reference Li, Xiao and Zhang25]. In the clinic, WBC is needed to combine with other hematological indexes to diagnose infectious diseases because its level could be regulated by some inflammatory responses and infections [Reference Li, Xiao and Zhang25]. HGB was also one of the hematological indexes and has been reported to be associated with the prognosis of SBI patients [Reference Tan, Zhang, Chen, See and Feng26]. The association between monocyte and bacterial infection has been reported, and mean monocyte volume increased in postsurgical bacterial infection [Reference Zhu, Cao, Fang, Zhong and Xu27]. In addition, MCV was a measure of the mean size of erythrocytes and has long been a useful index for diagnosing infectious diseases [Reference Hsieh, Chang, Kor, Yang, Wen and Chiu28, Reference Sakamoto, Ogawa, Inoue, Shine, Matsui, Nishi, Utsunomiya, Tamura, Takai and Takada29]. The mechanism underlying the association between MCV and SBI was unclear. One potential explanation was that there was an association between a high MCV and malnutrition, which caused a decrease in immunologic function, thereby increasing the susceptibility to infections [Reference Jomrich, Hollenstein, John, Ristl, Paireder, Kristo, Asari and Schoppmann30, Reference Prendergast31]. In addition, evidence has shown that premature delivery and weight were also influencing factors for the diagnosis of SBI [Reference Barak-Corren, Elizur, Yuval, Burstyn, Deri, Schwartz, Megged and Toker32, Reference Pathak, Upadhayay, Mathur, Rathi and Lundborg33]. Our model developed based on log SII, WBC, HGB, MCV, monocyte, weight, and premature delivery showed a good performance to diagnose SBI, with an AUC of 0.812.
Also, we developed a nomogram based on the diagnostic model. Nomogram was a visual tool that could simplify a large number of complex factors into a single simple numerical estimation model to determine the probability of events [Reference He, Zhu, Chen, Chen, Wang, Ouyang, Yang, Huang, Zhuang, Mao, Ben-Horin, Wu, Ouyang, Qian, Lu, Hu and Chen34]. The nomogram in this study may be convenient for clinicians to use. Using the nomogram, clinicians could make individualised predictions of SBI probability for each patient. Our model showed high performance for the prediction of negative results due to the high value of NPV and specificity. For individuals who were predicted with positive results, more examinations should be performed to further verify the diagnostic results. Our model was developed based on routine blood parameters, which were easy to obtain using a routine analyser [Reference Zhu, Chen, Wang, Zhang, Lu and Sun6]. If an algorithm was embedded within a blood analyser to report a probability of SBI in the lab results, it might be helpful for clinicians to determine to start or stop the use of antibiotics. In future, more effort is still needed to optimise this diagnostic model to make it be practicable in the clinic.
There are several limitations to this study. First, our data are extracted from the MIMIC-III database, and data missing is inevitable. Participants with missing data are excluded from our study, which may cause a decrease in the sample size, thereby reducing the statistical power of the model. Second, SBI is defined based on medical records rather than the results of bacterial culture, which may exist reporting bias. Third, our model is short of external validation and validation in non-ICU settings. Future studies are needed to verify the performance of our model in external patients and non-ICU populations.
Conclusion
We developed a model based on routine blood examination to diagnose SBI in neonates admitted to the ICU, and this model showed a good performance. Nomogram was developed to make the model convenient to use in the clinic. By applying this model, clinicians could predict each individual’s probability of SBI and improve treatment recommendations for a high-risk population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0950268823001231.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author contribution
Conceptualization: R.L., F.X.; Writing – original draft: R.L., F.X.; Writing – review & editing: R.L., F.X.; Data curation: Z.W., X.L., J.Y., S.Y., Z.C.; Formal analysis: Z.W., X.L., J.Y., S.Y., Z.C.; Investigation: Z.W., X.L., J.Y., S.Y., Z.C.; Methodology: Z.W., X.L., J.Y., S.Y., Z.C.
Financial support
This research received no specific grant from any funding agencies, commercial sectors, or not-for-profit sectors.
Competing interest
The authors declare none.
Ethical standard
This study was exempt from signing informed consent because MIMIC-III is a publicly available database.










 Open access
Open access