The coronavirus disease 2019 (COVID-19) pandemic has led to >6.54 million deaths worldwide. 1 Although the complete impact of the pandemic remains to be elucidated, healthcare disparities in vulnerable populations have been made evident. Reference Andraska, Alabi and Dorsey2 The risk of COVID-19, hospitalization, and deaths in Black and Latinx communities are 1.5–2.3 higher than White, non-Hispanic communities. 3 Vaccine research has been streamlined by entities such as the National Institutes of Health. Despite these efforts, vaccine hesitancy and access barriers in racial and ethnic minorities has continued. Reference Padamsee, Bond and Dixon4,Reference Andrasik, Broder and Wallace5 Historical injustices and misinformation are important barriers at play in fostering trust toward the medical community and belief in vaccine efficacy for these communities. Reference Andrasik, Broder and Wallace5,Reference Hildreth and Alcendor6
A promotoras model intended to lessen the disparities gap and improve COVID-19 vaccinations rates was proposed. In this model, local community members are frontline outreach workers who represent a bridge between healthcare infrastructures and the communities they serve. Reference Cáceres, Shirazipour, Herrera, Figueiredo and Salvy7 Prior studies have proven the success of promotoras in promoting lifestyle modifications and chronic disease management. Reference Cáceres, Shirazipour, Herrera, Figueiredo and Salvy7 Data supporting their role in mass vaccination campaigns are limited. Reference Cáceres, Shirazipour, Herrera, Figueiredo and Salvy7 However, promotoras were an important part of our efforts during the COVID-19 pandemic and were critical for our mass vaccination campaign. We implemented a culturally sensitive, multilingual, community outreach model with promotoras to further vaccine administration in marginalized communities. Here, we describe our model and its impact on vaccination rates in our community.
Methods
Study setting
Saint Anthony Hospital (SAH) is a 151-bed, urban, community hospital on the west side of Chicago, Illinois. The service area for SAH includes underserved populations with 26.5% below the federal poverty level, unemployment rate at 12.2%, preventable hospitalization rate 35.2% higher compared to Chicago overall. This region is designated as Health Professional Shortage Area (HPSA). The hospital and community were heavily affected by COVID-19. Reference Sabino8
Study design
We conducted a retrospective comparative study of publicly available data reported to the Chicago Department of Public Health (CDPH). Reference Clair, Mahr and Schencker9 We compared initial doses of COVID-19 vaccinations provided between SAH and other facilities in the Chicagoland area, sorted by ZIP codes to assess the reach of first doses to vulnerable communities. The Chicago COVID-19 community vulnerability index is a formula adapted by CDPH from Surgo Ventures. The CDC social vulnerability index identifies communities disproportionately affected by COVID-19 and uniquely vulnerable to barriers to COVID-19 vaccine uptake. We used these indices to define ZIP codes as being areas of low, medium, or high vulnerability to COVID-19. 10 The University of Illinois at Chicago Institutional Review Board approved this study.
Intervention
Promotoras were trained on COVID-19 topics as well as frequently asked questions about COVID-19 vaccines. They were deployed to high-traffic areas of the community, such as supermarkets, churches, and laundromats, between February 1 and May 31, 2021. All promotoras lived in the community, reflected the language, ethnicities, and cultures of the communities where they were deployed. Promotoras provided COVID-19 vaccine education and discussed attitudes, beliefs, and concerns in an individual’s preferred language. They attended check-in sessions 3 times each week to discuss questions and concerns from within the communities, and they provided answers to these questions and information sheets listing vaccine eligibility and requirements. For individuals who expressed interest in vaccination, the promotoras immediately contacted SAH via telephone and scheduled first-dose appointments.
Results
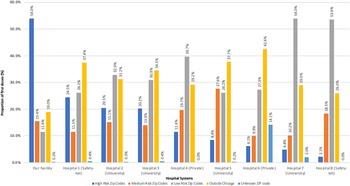
In total, 109 promotoras were hired, of whom 73 (67%) identified at Hispanic or Latinx, 29 (27%) identified as Black or African American, and 7 (6%) identified as Asian orAsian American. Promotoras were multilingual in languages such as English, Spanish, and Chinese. The promotoras had 8,806 encounters and made 5,567 appointments (acceptance rate, 63%) for 3,192 first doses (attendance rate, 57%). In total, 14,636 initial doses were administered during the study period. The mean age of individuals receiving their first dose at SAH was 45.5 years (range, 12–98 years), the preferred languages were Spanish (54%), English (38%), and Chinese (8%). The most common reported ethnicity was Hispanic (66%), and the most common race was White (54%) (Fig. 1). Moreover, 69.4% of first-dose vaccinations at SAH lived in high-to-medium COVID-19 vulnerability ZIP-code areas (Fig. 2).

Fig. 1. Racial distribution of vaccinated individuals at our facility.

Fig. 2. First-dose COVID-19 vaccines administered by hospitals stratified by recipients’ ZIP-code–based Chicago COVID-19 community vulnerability index.
Discussion
We implemented a culturally sensitive outreach model that proved successful at providing COVID-19 vaccines to vulnerable populations in the Chicago area. The SAH administered initial shots to 54% of residents in high COVID-19–risk ZIP codes and 15.45% of residents in medium COVID-19–risk ZIP codes. These rates outpaced other hospital systems in the area despite their proximity. We hypothesize this success was due to the promotoras model. The promotoras were recruited from within the communities they eventually served, and many had prior experience as community health workers. This enhanced their ability to relate and gain the trust of the individuals from within their communities as they discussed the benefits of COVID-19 vaccinations and facilitated appointment scheduling. A key lesson learned related to barriers for scheduling, which may have been lowered by the ability to instantly link potential patients to the healthcare system without requiring an Internet connection. Many early vaccine appointments relied on existing patient lists and computer scheduling, presenting further challenges and barriers. In these vulnerable communities, individuals may not have had a pre-existing relationship with a particular hospital system, may have lacked access to reliable technology, and/or may not have been able to manage interfacing with rapidly evolving scheduling platforms. Hospital systems with the most success in vaccinating vulnerable communities shifted methods to calling residents directly, reserving appointments for populations with increased COVID-19 risk, and opening care to all versus only previously established patients. The promotoras likely had an impact beyond facilitating scheduling for the first appointment by increasing awareness of COVID-19 vaccine, answering questions, and becoming ambassadors for the mass vaccination campaign in the community.
Long-standing healthcare inequities were reflected in both the impact of COVID-19 and the acquisition of initial COVID-19 vaccine doses in Chicago. Of the first 1 million doses administered, >60% were provided to residents of neighborhoods with the lowest COVID-19 risk, and <40% were provided to communities deemed high or medium risk for COVID-19 that were primarily Black and Latinx. Reference Clair, Mahr and Schencker9 The use of community outreach workers and promotoras may help reduce this gap in future mass vaccination campaigns. Future pandemics and future healthcare initiatives may experience greater success via increased development and utilization of the promotoras model described in this study.
The strengths of this study included the comparative data across health systems, cultural competency of hospital leadership (administration, infectious diseases physician) who are also members of the communities served, and real-time data collection. The limitations of this study included a lack of comparison of first-dose vaccination rates to second-dose or booster vaccination rates using the promotoras model, lack of specific descriptions of other hospitals vaccination rates and experiences, and lack of surveys of the community to determine the perceived impact of the promotoras.
In conclusion, the promotoras, recruited from the communities they served, likely contributed to the greater rater of vaccination in these areas compared to other communities in neighboring areas at similar COVID-19 risk but without promotoras.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2023.1
Acknowledgments
The authors acknowledge the colossal efforts of healthcare workers and essential workers during the COVID-19 pandemic, including our outreach workers and promotoras.
Financial support
No financial support was provided relevant to this article.
Conflicts of interest
All authors report no conflicts of interest relevant to this article.