


According to the World Health Organization (WHO), chronic diseases are defined as diseases of long duration and generally slow progression (1). Longer life expectancy and increasing numbers of people living with chronic diseases go along with the greater proportion of elderly people in Western society (Reference Barlow, Wright, Sheasby, Turner and Hainsworth2). In parallel, healthcare costs are increasing in Western countries. The cost of chronic diseases and their risk factors are significant and can rise to almost 7 percent of a country's gross domestic product (GDP) (Reference Suhrcke, Nugent, Stuckler and Rocco3). Governments face the challenge to meet, on the one hand, all of society's healthcare related needs and demands, and, on the other hand, the need to deal with scarce financial and material healthcare resources. The increased availability of new, often more expensive, healthcare interventions for chronic patients makes it imperative for policy makers to make a rational choice between alternatives.
Self-management is one of the healthcare interventions, which has recently become more prominent and important in chronic health care as it focuses on reaching optimization, efficiency, and sustainability of care by managing the existing intervention. In 1999, Lorig et al. (Reference Lorig, Sobel and Stewart4) developed the Stanford Chronic Disease Self-Management Program (CDSMP). The effectiveness of the CDSMP, based on Bandura's Social Learning Theory (Reference Bandura5), was recently investigated in a systematic review conducted by Franek (Reference Franek6). He found that, in comparison with care as usual, CDSMP resulted in significant, short term improvements in terms of health related quality of life and self-effectiveness. The popularity of this particular intervention has risen over the past two decades.
Defining self-management is a challenge, because a wide variety of interpretations and explanations exist. Self-management is often used interchangeably with self-care, self-help, and education, among others. Barlow et al. (Reference Barlow, Wright, Sheasby, Turner and Hainsworth2) defined self-management as: “An individual's ability to manage the symptoms, treatment, physical, and psychosocial consequences and lifestyle changes inherent in living with a chronic condition. Efficacious self-management encompasses the ability to monitor one's condition and to affect the cognitive, behavioral, and emotional responses necessary for maintaining a satisfactory quality of life and, thus, establish a dynamic and continuous process of self-regulation” (Reference Barlow, Wright, Sheasby, Turner and Hainsworth2). Because this definition adequately captures the domain of self-management, we choose to use this definition in this review and articles are selected in line with this definition.
There are four reasons for doing this review. First, the significance of self-management interventions (SMIs) in chronic health care and pharmaceutical therapy has been acknowledged (Reference Janson, McGrath, Covington, Cheng and Boushey7;Reference Warsi, Wang, LaValley, Avorn and Solomon8). Second, previous research shows positive results regarding the effectiveness of SMIs (Reference Willems, Joore, Hendriks, Wouters and Severens9). Third, there is potential for SMIs to be cost-effective for specific chronic diseases. However, current evidence on the cost-effectiveness of SMIs is limited. Fourth, following the previous arguments, this calls for new, up-to-date evidence concerning the methodological quality of these studies and the effect of this quality on the interpretation of cost-effectiveness results.
To our knowledge, there has been no overall systematic review focusing on the methodological quality of full economic evaluation studies of SMIs. Therefore, our aim was to systematically review the literature of full economic evaluation studies, both trial-based and model-based, of one or more SMIs in adult chronic patients to investigate the methodological quality of the studies and the cost-effectiveness of the interventions.
METHODS
Study Approach
This review is conducted according to the PRISMA guidelines, containing twenty-seven items. This study was not registered in the international prospective register of systematic reviews (PROSPERO) before starting but we used a predefined research protocol.
Selection Criteria
Full economic evaluation studies reporting on SMIs in line with Barlow's definition (Reference Barlow, Wright, Sheasby, Turner and Hainsworth2) of self-management were eligible for inclusion. A full economic evaluation is considered a comparative analysis of two or more interventions in terms of both costs (resource use) and consequences (outcomes, effects) (Reference Drummond and Jefferson10). It was our goal to include as many relevant papers as possible, however, we focused on studies reporting a chronic disease. Studies were excluded if patients could not be classified as having a chronic disease or receiving chronic care, if participants were younger than 18 years of age, if the study was not written in English or Dutch and/or was published before 1990. A chronic patient was defined as a person who experiences living with the affliction that often accompanies chronic disease (Reference Martin11). Furthermore, we excluded studies when they did not report on original data in a primary research paper (i.e., systematic reviews, congress abstracts, and commentaries, among others).
Information Sources
Two electronic databases were searched for relevant articles published between January 1990 and May 2014. Because the majority of SMIs was developed and studied for their efficacy in the past decade, we chose 1990 as the starting point for our search. We used PUBMED and the National Institute for Health Research Economic Evaluation Database (NHSEED). Although NHSEED makes an extensive search of PUBMED among others (CINAHL, Embase, PsycINFO, and MEDLINE) on a weekly basis, using a very efficient filter embedded in their search engine for economic evaluation studies, we performed a separate search in PUBMED as well as this combination is regarded as the most valid search strategy for economic evaluation studies (Reference Alton, Eckerlund and Norlund12;Reference Sassi, Archard and McDaid13). In addition, reference lists were screened for additional relevant publications.
Search Strategy
The search string used in this study was based on leading reviews of self-management and existing economic evaluation search strategies (Reference Barlow, Wright, Sheasby, Turner and Hainsworth2;Reference Alton, Eckerlund and Norlund12–Reference Newman, Steed and Mulligan16). The following set of keywords was used to search PUBMED, either as a MeSH term if possible, or as general search term title/abstract: [“self management”], [“self-management”], [“self care”], [“self-care”]; and [“economics”], [“cost analysis”], [“cost benefit analysis”], [“cost-benefit analysis”], [“cost effective”], [“cost-effective”]. Because NHSEED searches only databases for economic evaluation studies, only the set of keywords for self-management was used to identify relevant studies in this database. We used a “language” filter (either Dutch or English) and searched only for articles published in or after 1990. All results were downloaded into the bibliographic management software EndNoteX and duplicates were removed. A detailed search string is presented in Supplementary Figure 1.

Figure 1. Flowchart of study selection.
Study Selection
Eligibility assessment was performed by the primary researcher (M.v.E.) and three other reviewers (C.v.H., S.E., and G.v.M.). M.v.E. did the electronic database search and screened all articles on title and abstract. All papers that met the eligibility criteria were categorized in the group as “potential,” and papers that undoubtedly did not meet these criteria were immediately excluded. In case of doubt, decisions were made through consensus by two of the four reviewers (M.v.E. with C.v.H., and G.v.M. with S.E.). Subsequently, all articles meeting the eligibility criteria were assessed independently by two of the four reviewers. This assessment consisted of data extraction of all selected full-text articles in addition with a critical appraisal of the Consensus Health Economic Criteria List (CHEC-list). Any disagreement on data extraction between reviewers was resolved through consensus.
Data Extraction and Methodological Quality Assessment
By means of a predefined form (Reference Evers, Van Wijk and Ament17), the following data were extracted from the papers: First, general and randomized controlled trial (RCT) information was retrieved. Quality of RCTs was determined through assessment: the use of intention-to-treat analysis (ITT) (yes, no, unclear), allocation concealment (adequate, unclear), and blinding of outcome assessors (adequate, unclear) (Reference Higgins and Green18). If the paper reporting on the economic evaluation study did not contain sufficient information on trial design, the paper describing the original study design was used for data extraction. Second, economic information was assessed, including the economic evaluation design used, synthesis of costs and effects, and cost-effectiveness of the SMI (yes/no). The quality of the economic evaluation was determined by means of the adjusted CHEC-list which is fit for RCTs and model-based studies (Reference Odnoletkova, Goderis and Lore19) consisting of nineteen yes-or-no questions (Reference Evers, Goossens, de Vet, van Tulder and Ament20). The CHEC-list is recommended by Cochrane (Reference Higgins and Green18). Because no weighting exists for the CHEC-list, we used scores of 1 (yes) and 0 (no) to value the items and categorized studies as: low (<8 score), moderate (9–14 score) and high (>15 score). For studies that did not discount costs and/or effects due to a 12-month or less follow-up, item 14 (were future costs and outcomes discounted) on the CHEC-list was disregarded and for these studies a maximum score of eighteen could be obtained. However, this had no impact on the categorization of studies.
RESULTS
Review Profile
A total of 2,760 records were identified from the search (Figure 1). After removing duplicates (n = 248), 2,512 records were screened on title and abstract; of these, 2,454 records were excluded. The main reasons for exclusion were: not reporting data in a primary research paper, using a description of self-management not in line with the Barlow's definition and the absence of cost data. A total of fifty-eight full text records were then assessed by the reviewers, of which twenty-three fulfilled the inclusion criteria (Reference Bourbeau, Collet and Schwartzman21–Reference Wang, Smith and Bosworth43). One study performed by Kauppinen et al. was published as an additional publication (Reference Kauppinen, Vilkka, Sintonen, Klaukka and Tukiainen29) with respect to a previous study (Reference Kauppinen, Sintonen and Tukiainen28). The data of this publication were also extracted and presented in this review, but for simplification purposes only the reference of the original article (Reference Kauppinen, Sintonen and Tukiainen28) will be used in the text. Accordingly, the results are based on twenty-three publications from twenty-two studies.
General, RCT-Related and Economic Characteristics
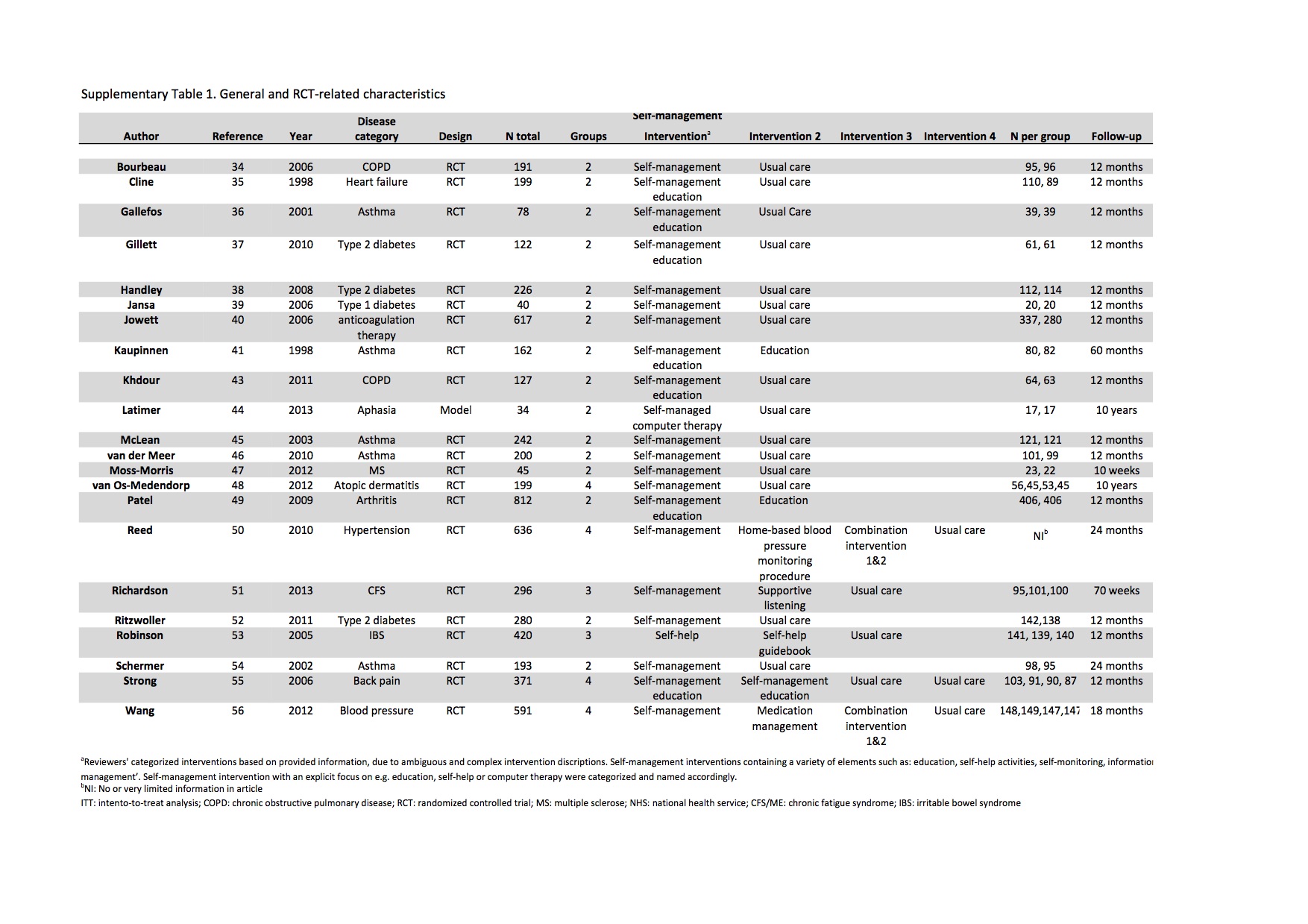
All twenty-two studies were published after 1998 (Table 1, Supplementary Tables 1 and 2), eight were based in the United Kingdom (Reference Gillett, Dallosso and Dixon24;Reference Jowett, Bryan and Murray27;Reference Khdour, Agus and Kidney30;Reference Latimer, Dixon and Palmer31;Reference Moss-Morris, McCrone and Yardley34;Reference Patel, Buszewicz and Beecham36;Reference Richardson, Epstein and Chew-Graham38;Reference Robinson, Lee and Kennedy40), six in mainland Europe: the Netherlands (Reference van der Meer, van den Hout and Bakker33;Reference van Os-Medendorp, Koffijberg and Eland-de Kok35), Finland (Reference Kauppinen, Sintonen and Tukiainen28), Sweden (Reference Cline, Israelsson, Willenheimer, Broms and Erhardt22), Norway (Reference Gallefoss and Bakke23), Spain (Reference Jansa, Vidal and Viaplana26), six in the United States (US) (Reference Handley, Shumway and Schillinger25;Reference Reed, Li and Oddone37;Reference Ritzwoller, Sukhanova and Glasgow39;Reference Schermer, Thoonen and van den Boom41–Reference Wang, Smith and Bosworth43) and two in Canada (Reference Bourbeau, Collet and Schwartzman21;Reference McLean, Gillis and Waller32). Asthma/chronic obstructive pulmonary disease (COPD) and diabetes were the most common disease categories in eleven studies. One study used data from an RCT to construct a Markov model. All others used an RCT design including two, three, or four intervention groups. A total of 23 percent (n = 5) of the studies evaluated two or more SMIs.
Table 1. General, RCT-Related and Economic Characteristics

a Disease categories are further explained in Supplementary Table 1.
b NI, no, or limited, information available.
c SMI, self-management intervention.
d QoL, quality of life.
e CQ, cost questionnaire.
f NHS, National Health Service.
The intensity of the SMI varied between studies, from two visits and a phone call up to sixty computer sessions per participant. The SMI was primarily delivered by a (trained) nurse in eleven studies. Almost one-third (n = 8) of the interventions were offered to patients at home. In three studies, interventions took place in the hospital, in three studies interventions were at a special clinic and in three other studies interventions were at the general practitioner's (GP) office. All SMIs consisted of multiple sessions (individual or group), sometimes combined with phone calls. Sixteen studies (73 percent) provided limited or missing information on the description of the control intervention(s), the other 27 percent of the studies were thorough in reporting on the control intervention(s). Only one study had a 10-week follow-up period. A 12-month follow-up period was chosen in fifteen studies, and the other seven studies had follow-up periods ranging from 18 months up to 10 years.
In seven studies (32 percent), ITT analyses were performed; in other words, all randomized patients were analyzed in the assigned group regardless of whether they completed the follow-up period or received the treatment (ITT). The remaining 15 studies either did not us an ITT analysis method (n = 8) or it was unclear whether an ITT analysis was conducted (n = 7). Twelve studies (n = 12) reported adequately concerning the concealment of allocation. Limited to no information on concealment of allocation was provided in the remaining ten studies. Only four studies (18 percent) reported blinding of the outcome assessor(s). The remaining eighteen studies either mentioned that a nonblinded study was concerned, or insufficient information was provided on blinding.
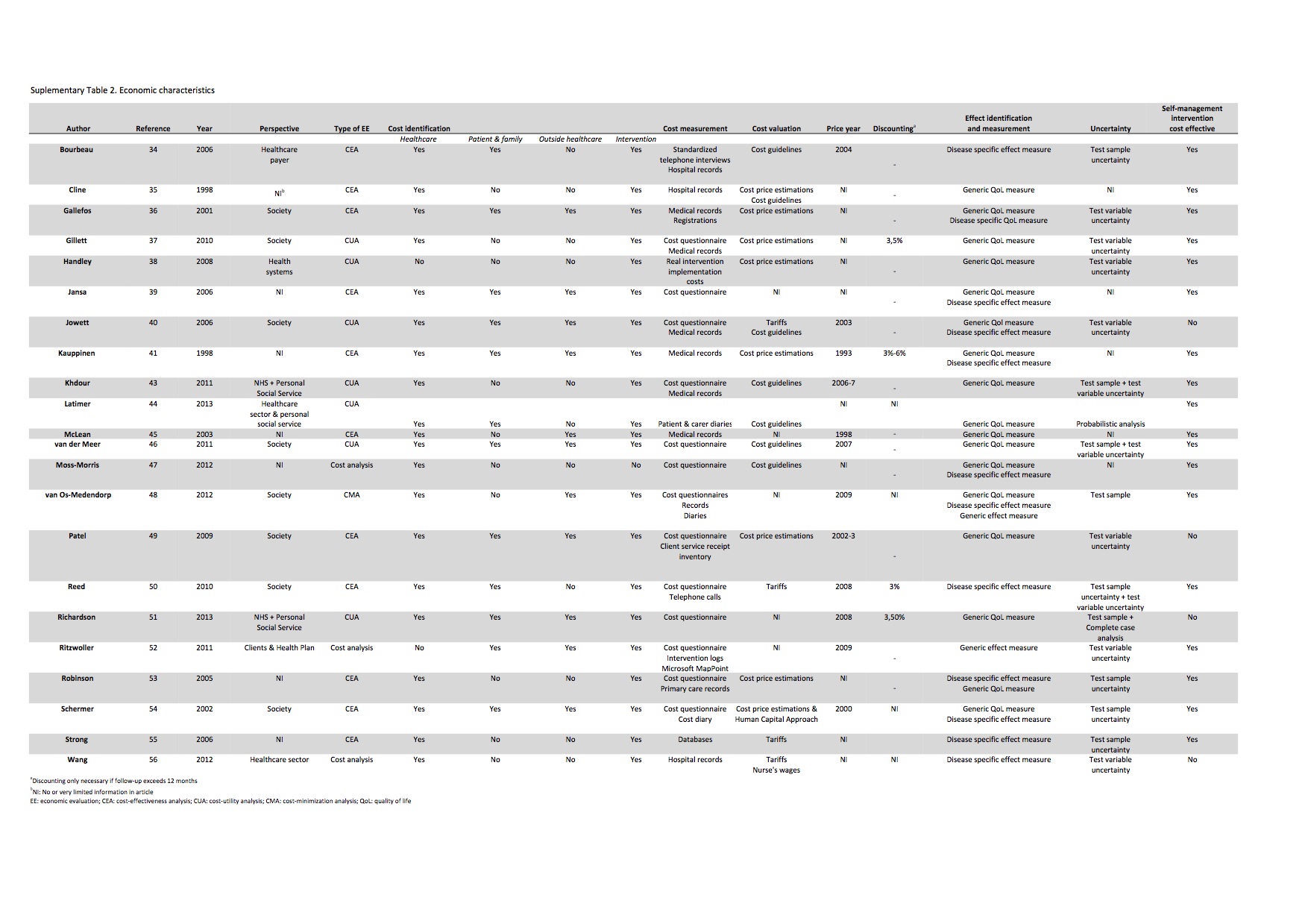
In 68 percent (n = 15) of the studies, a perspective of analysis was mentioned and almost half of these (n = 8) performed their analyses from a societal perspective. In 32 percent of the studies (n = 7), no information was provided on the chosen perspective. All but four of the studies performed either a cost-effectiveness analysis (CEA) or cost utility analysis (CUA), although it is worth mentioning that authors used both concepts interchangeably. The four other studies conducted either a cost analysis or cost-minimization analysis (CMA). Two studies did not measure any type of healthcare costs (categorized as hospital visits, GP visits, and other healthcare consumption, among others).
Patient and family costs (categorized as costs of informal care and travel costs, among others) were not identified in ten studies. In eleven studies, no costs outside the healthcare sector (categorized as productivity costs, among others) were identified. One study took intervention costs into account. All but three of the studies used a cost questionnaire, medical/hospital records, or both, among other instruments as means for measuring costs. Approximately 55 percent of the studies (n = 12) based their cost valuation on either cost price estimations, cost guidelines, or both. The remaining 45 percent of the studies (n = 10) used either tariffs, tariffs combined with cost guidelines, cost price estimations combined with the human capital approach, tariffs combined with nurse wages, or did not mention any form of cost valuation. Almost half of the studies (n = 10) did not mention a price year with respect to the cost calculation. Four of eight studies with a follow-up period of 18 months or more did not report a discount rate.
Ten studies used only generic effect measures, four used only disease specific effect measures and eight used both. In seven studies, uncertainty was handled using test variable uncertainty methods (e.g., sensitivity analysis), five studies used test sample uncertainty methods (e.g., bootstrapping) and in three studies a combination of these was used. Other methods of handling uncertainty were probabilistic analysis and test sample uncertainty combined with complete case analysis. In five studies, no handling of uncertainty was mentioned. Thirteen studies (59 percent) used an incremental cost-effectiveness ratio (ICER) to synthesize costs and effects, and one study combined the ICER with the calculation of a Net Monetary Benefit (NMB). The remaining nine studies did not mention any method for synthesizing costs and effects. Almost half of the studies (n = 10) made cost-effectiveness results visible. Seven studies presented a cost-effectiveness acceptability curve (CEAC), the remaining three used either a cost-effectiveness plane (CE plane), a CEAC and CE plane combined, or a cost-concentration curve.
Quality of the Economic Evaluation
A total of fourteen studies could obtain a maximum of 18 points on the CHEC-list (Table 2); the other eight could obtain nineteen points. Seven studies were categorized into the highest category (>15 score (Reference Handley, Shumway and Schillinger25;Reference Khdour, Agus and Kidney30;Reference Latimer, Dixon and Palmer31;Reference van der Meer, van den Hout and Bakker33;Reference van Os-Medendorp, Koffijberg and Eland-de Kok35;Reference Patel, Buszewicz and Beecham36;Reference Richardson, Epstein and Chew-Graham38), nine studies into the group “moderate” (9–14 score) (Reference Cline, Israelsson, Willenheimer, Broms and Erhardt22–Reference Gillett, Dallosso and Dixon24;Reference Jowett, Bryan and Murray27;Reference Kauppinen, Sintonen and Tukiainen28;Reference Reed, Li and Oddone37;Reference Ritzwoller, Sukhanova and Glasgow39;Reference Strong, Von Korff, Saunders and Moore42;Reference Wang, Smith and Bosworth43), and six studies received a “low” score (<8) (Reference Bourbeau, Collet and Schwartzman21;Reference Jansa, Vidal and Viaplana26;Reference McLean, Gillis and Waller32;Reference Moss-Morris, McCrone and Yardley34;Reference Robinson, Lee and Kennedy40;Reference Schermer, Thoonen and van den Boom41). On average, all studies included in this review scored 13.9 on the CHEC-list range 4–17. Studies published before 2007 (n = 10) had on average a lower score in comparison with the studies published in 2008 or later (n = 12). There were several CHEC-list items on which various studies did not score points. For instance, twelve studies did not justify their choice of perspective. Half of the studies (n = 11) did not give a full identification of all relevant costs in relation to the perspective. Twelve studies did not give a detailed description of the competing interventions and ten studies did not perform a sensitivity analysis. Thirteen studies reported no ethical aspects and did not elaborate on the characteristics of the population experiencing the disease and intervention and how this may have distributional implications.
Table 2. Critical Appraisal of the Quality of the Economic Evaluation (+ = the Article Sufficiently Handled the CHEC-List Criterion)

*Discounting not necessary due to follow-up up to 12 months.
Cost-Effectiveness
In eighteen studies (82 percent), the authors found the SMI to be cost-effective (Table 3), either due to increased costs and effects in comparison with the control intervention (Reference Gillett, Dallosso and Dixon24;Reference Handley, Shumway and Schillinger25;Reference van der Meer, van den Hout and Bakker33;Reference Reed, Li and Oddone37;Reference Strong, Von Korff, Saunders and Moore42), or decreased costs and increased effects in comparison with the control intervention (Reference Bourbeau, Collet and Schwartzman21–Reference Gallefoss and Bakke23;Reference Jansa, Vidal and Viaplana26;Reference Kauppinen, Sintonen and Tukiainen28;Reference Khdour, Agus and Kidney30–Reference McLean, Gillis and Waller32;Reference Moss-Morris, McCrone and Yardley34;Reference van Os-Medendorp, Koffijberg and Eland-de Kok35;Reference Ritzwoller, Sukhanova and Glasgow39–Reference Schermer, Thoonen and van den Boom41). One of the twenty-two studies did not find positive cost-effectiveness results at the 12 months follow-up, but in the additional publication focusing on long term cost-effectiveness the SMI proved cost-effective. Four studies concluded that the SMI was not cost-effective; three found no significant differences in comparison with the control intervention and in one study the control intervention was cheaper and more effective and, therefore, dominant over the SMI.
Table 3. Cost-Effectiveness Results

a ICER, incremental cost-effectiveness ratio; OK, Norwegian Krone; SGRQ, St. George's Respiratory Questionnaire; REV, forced respiratory volume; SMI, self-management intervention; FIM, Finnish Markka; 15D, Health State Descriptive System Questionnaire; FVC, forced vital captivity; PD, airway hyper responsiveness; PEF, peak expiratory flow; QALY, quality-adjusted life year; SF-36, short-form 36.
DISCUSSION
As far as we know, this is the first overall systematic review of the methodological quality and cost effectiveness of full economic evaluation studies of SMIs in adult chronic patients. Twenty-two studies of twenty-three publications were identified, in most cases published either in Europe or the United States. All studies were published from 1998 onward and more than half of the studies were published after 2006. This review included one model-based and 21 trial-based economic evaluations. Most of the studies performed either a cost-effectiveness analysis or a cost-utility analysis.
The reported SMIs were very heterogeneous in terms of time span, intensity, contents, interventions providers, and target populations. In general, the methodological quality was moderate, despite the fact that the majority of studies were RCTs. Nevertheless, only one study fulfilled all three evaluated quality criteria (ITT, allocation concealment, and blinding of outcome assessor), and in five studies, none of these criteria were met. Furthermore, there was lack of detailed information on the control intervention(s) among all studies and in some cases nothing was reported.
Only seven of the twenty-two studies that reported data on costs had an acceptable score on the CHEC-list and the majority of studies had either a moderate or low score. The methodological quality of the economic evaluation was very mixed, but this was insufficient in a greater part of the studies, which were unclear on synthesizing costs and effects and sensitivity analyses. Eleven studies did not report on the perspective of analysis but the majority of those who did used a societal perspective. However, the majority of studies with high methodological quality did show positive cost-effectiveness results of the SMIs. Also, these high quality studies were more likely to report a QALY as outcome measure compared with studies with moderate or even low methodological quality. Studies with higher methodological quality reported extensively on methods of analysis, and provided arguments for choices and considerations with regard to cost-analyses. We found that more recently published studies showed higher methodological quality. This might also be due to the fact that the economic evaluations were conducted as independent study and not integrated with the effect study.
We encountered several difficulties in selecting of studies reporting SMIs and in the categorization of these interventions. It was evident in advance that the absence of a clear and solid definition would pose difficulties. We chose a definition formulated by Barlow et al. (Reference Barlow, Wright, Sheasby, Turner and Hainsworth2) that in our view captured the full domain of self-management adequately and we used this definition as indicator for the selection of relevant articles for this review. Despite choosing this definition we found it a major challenge to use the definition in our research. This can be illustrated by the rejection of an article with self-management in its title as we found that the contents of the article and the description of self-management did not fit our definition (Reference Hurley, Walsh and Mitchell44).
Another difficulty was in categorizing SMIs. Self-management can serve as an intervention on its own with, for example, educational sessions and self-help activities as sub-elements, or self-management can be a sub-element of an educational intervention. Furthermore, self-management, education, self-care, and self-help are continuously being used interchangeably, sometimes even for the same activities or programs in one study. A review conducted by Nolte and Osborne (Reference Nolte and Osborne45) on the outcomes of chronic disease self-management interventions found that due to the different types of SMIs it is very difficult to estimate the true impact of these interventions. These findings are indicative of the highly ambiguous and complex character of an intervention becoming vastly more popular among scientists and healthcare providers and the difficulties, which researchers encounter when reviewing the literature on this topic.
The majority of studies (n = 18) found the SMI(s) to be cost-effective in comparison with other, mostly care as usual, interventions. SMIs are usually multi-faceted programs in which different strategies and techniques are used and applied to help patients to manage their disease over time. Furthermore, SMIs tend to increase understanding and awareness among patients considering their own disease. This allows them to, for example, get a better idea of which healthcare services are necessary to cope with their current situation and may improve medicine adherence. This could easily result in a decrease of healthcare consumption and, therefore, a decrease in costs; hence, it seems plausible for self-management interventions to prove to be cost-effective. However, the cost-effectiveness results of the studies included in this review must be interpreted with caution because thirteen studies with a moderate or low quality score conclude that the SMI is cost-effective. It is imperative that these conclusions are preceded by a solid methodological study quality on the one hand and a clear and explicit understanding of the theoretical context of the SMI on the other hand.
In this review, we explored the methodological quality of economic evaluation studies of SMIs in adult chronic patients, and investigated their cost-effectiveness. Our findings were in line with conclusions from previous related research. Willems et al. (Reference Willems, Joore, Hendriks, Wouters and Severens9) conducted a review on the cost-effectiveness of SMIs in asthma and concluded that due to wide diversity in interventions and poor methodological quality, conclusions had to be interpreted with caution. Dorn (Reference Dorn46) concluded that self-management has the potential to improve outcomes for chronic patients; however, the quality of studies was subpar due to the challenge of defining self-management and developing practical self-management interventions. In addition to previous findings, we find it remarkable that the increased popularity of SMIs has not been accompanied by the development of a clear, well-considered definition of the concept.
Limitations of This Review
First, the difficulties we encountered with the concept of self-management can be considered a limitation, as already mentioned in previous parts of the discussion. However, we chose a well-known definition of self-management after reviewing relevant literature, and two independent assessors decided whether the SMI was in line with our chosen definition of self-management. Second, we did not register this systematic review at PROSPERO but we did use a predefined research protocol. Third, we chose 1990 as the starting year for our search strategy, so we may have missed relevant articles published before this year. However, because the domain of both economic evaluation and self-management have been subject to scientific research mainly only for the past two decades (only two studies included in this review were published before 2000), we do not expect to have missed many relevant publications. Fourth, we used only two databases for our search strategy. Because NHSEED systematically searches multiple databases, all 23 studies included in this review can be found in both PUBMED and NHSEED, and a reference check of all included studies did not result in additional relevant studies we can argue that these two databases suffice for this review. Fifth, conference abstracts were excluded; hence, we could have missed some important on-going studies. However, because it would not be possible to analyze these data with the chosen research method we decided to exclude them. Finally, the use of the adjusted version of the CHEC-list may count as a limitation. The questions for the model-based studies were not valued by a Delphi panel yet (Reference Odnoletkova, Goderis and Lore19). However, as only one of the included studies in our review was a model-based economic evaluation this will not have influenced our study findings.
CONCLUSION
From this systematic review, we can conclude that the SMIs of adult chronic patients reported were heterogeneous and no clear, well-considered definition of self-management was used. Furthermore, the number of economic evaluation studies of SMIs is increasing, as is methodological quality. However, in general the methodological quality of the assessed full economic evaluation studies was moderate, the cost-effectiveness results must, therefore, be interpreted with caution.
RECOMMENDATIONS
For future research, we recommend that the methodological quality of economic evaluation studies of SMIs must be improved. One of the major difficulties we encountered was with the taxonomy of self-management and SMIs. We strongly recommend that future research efforts focus on defining the concept of self-management in such a way that it diminishes the fogginess around this concept. Not only researchers, but also healthcare decision makers, professionals and patients will benefit of this. Other difficulties related to the methodological quality of the economic evaluation studies. Up to date methods must be used for conducting economic evaluations such as the CHEERS guidelines (Reference Husereau, Drummond and Petrou47). Furthermore, more effort must be put in improving trial design and reporting. We would advise that future research uses the adjusted CHEC-list (Reference Odnoletkova, Goderis and Lore19) to assess model-based studies and to develop for CHEC-list items. In addition, we found a very limited number of economic evaluation studies in comparison with effect studies on self-management, which stresses the importance of conducting more economic evaluation studies attached to effect studies on self-management.
SUPPLEMENTARY MATERIAL
Supplementary Figure 1
Supplementary Tables 1 and 2 http://dx.doi.org/10.1017/S0266462316000027
CONFLICTS OF INTEREST
The authors declare that they have no competing interests.








 Open access
Open access