



Introduction
In 2015, there were an estimated 44 million family caregivers in the nation (National Alliance for Caregiving and AARP Public Policy Institute, 2015). By 2030, the population of older adults residing in the US is estimated to increase by 50% (Mather et al., Reference Mather, Jacobsen and Pollard2015). Many of these older adults will have chronic health conditions and disabilities and may be dependent on a caregiver. Mounting demands for caregiving and an increasingly ethnically diverse population have prompted a number of studies aimed at investigating the role of cultural values in caregiving experiences and health and mental health outcomes. These studies have expanded previous models of caregiver distress by exploring the role of sociocultural and contextual variables. One such model is Knight and Sayegh (Reference Knight and Sayegh2009)’s sociocultural stress and coping model, which elaborates on Pearlin et al. (Reference Pearlin, Menaghan, Lieberman and Mullan1981)’s stress process model and is particularly useful for the current study.
The sociocultural stress and coping model highlights the impact of sociocultural variables on caregiver health outcomes and incorporates not only broad racial/ethnic differences, but nuances in experiences and heterogeneity within racial/ethnic groups, such as acculturation level and immigration experiences. According to the U.S. Census Bureau (2020), over 44 million of the US population were foreign-born with a majority emigrating from Latin America and Asia.
Caregiving is an integral part of the cultural identities and practices held by many immigrant communities (Angel et al., Reference Angel, Rote, Brown, Angel and Markides2014; Montenegro, Reference Montenegro2014; Rote and Moon, Reference Rote and Moon2016). According to the National Alliance for Caregiving and AARP Public Policy Institute (2015) report, it is found that a higher percentage of Asian and Latino populations are caregivers compared to non-Hispanic White (NHW) populations. In the same report, the number of Latino and Asian surveyed participants 21% and 19.7% were caregivers, respectively, while only 16.9% of NHW participants were caregivers.
Theoretical/conceptual framework
Acculturation was first defined as changes in the “cultural patterns” of individuals that have had “firsthand contact” with each other (Redfield et al., Reference Redfield, Linton and Herskovits1936). Berry (Reference Berry2005)’s model of acculturation posited that factors which are external to the individual, including host culture dynamics, play an essential role in acculturation. Recent studies of acculturation have sought to capture these contextual elements using proxies such as generational status and language use or preference (Abraído-Lanza et al., Reference Abraído-Lanza, Echeverría and Flórez2016; Lara et al., Reference Lara, Gamboa, Kahramanian, Morales and Hayes Bautista2005; Salant and Lauderdale, Reference Salant and Lauderdale2003). In general, acquisition of the host language is thought to be positively correlated with the degree to which an individual is acculturated. Immigrant/generational status is a variable reflecting a time dimension and indicates exposure to host sociocultural norms, with succeeding generations conceptually more acculturated than preceding generations (Portes, Reference Portes1996).
Studies have shown that interview language and self-rated language use proficiency are reliable measures of acculturation (Lee et al., Reference Lee, Nguyen and Tsui2011; Lopez-Class et al., Reference Lopez-Class, Castro and Ramirez2011). Using data from the 2007 California Health Interview Survey (CHIS), Kim et al. Reference Kim(2011) found that Latino and Asian immigrants with low English language proficiency reported more psychological distress than English proficient and English-only speaking groups. In another California sample, Chang and Moon (Reference Chang and Moon2016) showed that immigrants with low English proficiency consistently reported higher psychological distress compared to only English-speaking groups. Whereas these findings fall in line with the acculturative stress model, in which acculturation is associated with less distress, other studies have found the opposite: acculturation being associated with more distress, a phenomenon referred to as the Healthy Immigrant Effect or Immigrant Paradox (Berry, Reference Berry1970).
In a study of US Mexican women, those who spoke English only had higher levels of psychological distress compared to their counterparts who were bilingual or did not speak English at all (Bekteshi et al., Reference Bekteshi, Xu and Van Tran2015). Our own studies revealed that among Chinese- and Vietnamese-American caregivers, those with higher levels of educational attainment and therefore were potentially more acculturated, reported more distress (Meyer et al., Reference Meyer, Liu, Nguyen, Hinton and Tancredi2018). Mancenido et al. Reference Mancenido, Williams and Hajat(2020) found that first-generation immigrants reported higher psychological distress than second-generation non-immigrants in a recent cohort surveyed in the 2015 CHIS.
Most of these studies have sought to define the role of acculturation on psychological distress reported by diverse racial/ethnic, non-caregiving groups. However, little is known about how caregiving interacts with acculturation level and immigration experiences to affect psychological distress. This is important as both acculturation and caregiving may be associated with greater distress, and their interaction may eventually lead to poor mental health. Results from a study on US ethnic minority caregivers found a significant association between acculturation, as measured by generational status, and caregiving practices (Miyawaki, Reference Miyawaki2016). Studies have suggested that various caregiving practices, which are impacted by cultural factors, significantly affect psychological distress among caregivers (Acton and Kang, Reference Acton and Kang2001; Knight and Sayegh, Reference Knight and Sayegh2009; Lawton et al., Reference Lawton, Kleban, Moss, Rovine and Glicksman1989; Novak and Guest, Reference Novak and Guest1989). In addition, though the relationship between acculturation and stress has been widely discussed, it is unknown how caregiving impacts this relationship. Thus, it is important to understand the intertwining relations of caregiving, acculturation, and psychological distress in these diverse populations.
This study aims to investigate the role of acculturation and caregiving status on psychological distress among Latinos and Asian Americans and Pacific Islanders (AAPIs) in a population-based sample. Moreover, we build on the social determinants of health literature and ecological theories of caregiver distress by examining how education, income, and neighborhood safety influence distress (Dilworth-Anderson et al., Reference Dilworth-Anderson, Williams and Gibson2002). Multiple studies examining non-caregiving populations match the healthy immigrant perspective (Booth et al., Reference Booth, Ayers and Marsiglia2014; Dey and Lucas, Reference Dey and Lucas2006; Frisbie et al., Reference Frisbie, Cho and Hummer2001; Gomez et al., Reference Gomez, Kelsey, Glaser, Lee and Sidney2004; Kennedy et al., Reference Kennedy, Kidd, McDonald and Biddle2015; Markides and Eschbach, Reference Markides and Eschbach2005). Thus, based on prior literature, we hypothesize that Latinos and AAPIs who are more acculturated will have more psychological distress, and that being a caregiver will further exacerbate this relationship (Booth et al., Reference Booth, Ayers and Marsiglia2014; Meyer et al., Reference Meyer, Liu, Nguyen, Hinton and Tancredi2018).
Methods
Sample
Data from the 2009 California Health Interview Survey (CHIS) were available as a public dataset (California Health Interview Survey, 2012). The CHIS has been conducted every other year since 2001 and is one of the largest population-based telephone health surveys in the nation. Surveys were conducted in English, Spanish, Mandarin, Cantonese, Vietnamese, and Korean. In California Health Interview Survey (2009), CHIS surveyed 47,614 adults that were representative of California’s non-institutionalized population. From the full sample, we limited our study sample to only those who reported their ethnicity as Latino/Hispanic or AAPI, bringing our sample to N = 13,161.
Measures
Outcomes. Psychological distress was measured using the Kessler-6 (K6) scale (Kessler et al., Reference Kessler2002). Participants were asked to recall the worst month in the past year when they had experienced serious psychological distress and were asked to report, during that time, how often they felt nervous, hopeless, restless, depressed, worthless, or that everything was an effort. Values ranged from 0 to 24, with higher values representing more distress.
Race/ethnicity and acculturation. Participants were coded into self-reported monoracial categories based on the US Office of Management and Budget’s federal race/ethnicity classification standards: (1) Hispanic/Latino, (2) Asian American, and (3) Native Hawaiian or Pacific Islander; we combined the latter two categories (AAPIs). We assessed acculturation in three different ways, via generational status, language of interview, and English language proficiency. Examining these acculturation proxies separately allowed us to compare and validate the acculturation proxies against one another. A categorical measure was created to indicate whether participants were third generation or higher (US born with both parents born in the US), second generation (US born with at least one non-US born parent), or first generation (non-US born). Language of interview was dichotomized as 0 = English and 1 = Spanish/Asian language. Self-reported English language proficiency was dichotomized as 0 = not well or 1 = well or only speak English.
Caregiving variables. Caregiver status was determined if participants endorsed providing care to a spouse, parent/parent-in-law, or grandparent in the last year. Co-residence with the care recipient and use of respite care were dichotomous variables (0 = no, 1 = yes). The support variable was created from two separate CHIS variables: caregivers were asked if there was someone else who could help them if they were unable to do it; those who said yes were noted as having informal support. Caregivers were also asked if they had paid for caregivers; those who said yes were noted as having formal support. Those who said no to both items received a 0 on the support variable, indicating no support.
Covariates. Education level was coded as 0 = less than high school diploma, 1 = high school diploma or equivalent, 2 = some college or Bachelor’s degree, and 3 = some graduate school or graduate degree. Marital status was coded by widowed/separated/divorced/never married or married/living with partner. Participants self-reported their gender (male versus female) and health status (on a scale from 1—Poor to 5—Excellent). Age was a continuous variable and centered at 50 in regression analyses. Income was computed by dividing total annual household income (in dollars) by the number of adults residing in the household. Neighborhood safety fears were assessed with the question, “How often do you feel safe in your neighborhood (1 = All of the time to 4 = None of the time)?” Responses were reversed coded so that higher values represented greater perceptions of neighborhood safety.
Data analysis
To account for the complex sampling design of CHIS, analyses were conducted via survey data analysis procedures (PROC SURVEYFREQ, PROC SURVEYMEANS, and PROC SURVEYREG) using SAS software, version 9.4 (SAS version 9.4, 2022). Weighted chi-square and linear regression analyses with the jackknife method for variance estimation and replicate weights (as recommended by CHIS) were conducted to examine Latino and AAPI group differences on the main variables of interest and demographic covariates. To assess associations between caregiver status, acculturation variables, and possible interactions, four separate linear regression models were fit to the data: Model 1 included indicator variables for race/ethnicity, caregiver status, generational status, and a generational status by caregiver status interaction, adjusting for covariates. Model 2 was the same as Model 1 except that the other acculturation proxy – language of interview – and its interaction with caregiver status was examined. Model 3 used English language proficiency as the acculturation proxy. Lastly, we examined whether acculturation by caregiver status interactions were further moderated by race/ethnicity. Unstandardized regression coefficient estimates and their standard errors are reported in the tables.
Results
Descriptive analyses
Table 1 presents the characteristics of participants in the study by generational status. Among non-caregivers, the mean age was 43.8 (SD = 0.2), 33.3 (SD = 0.4), and 39.9 years (SD = 0.8) in first-, second-, and third-generation groups, respectively. These means were comparable to those among caregivers, which were 43.3 (SD = 0.8), 36.5 (SD = 1.2), and 39.6 years (SD = 1.3) in first-, second-, and third-generation groups, respectively. Among both caregivers and non-caregivers, a higher percentage of the third generation was Latino compared to the second or first generation; in contrast, a higher percentage of the first generation was AAPI compared to the second or third generations. First-generation caregivers and non-caregivers had the highest proportion of individuals who did not achieve a 12th grade education, while second- and third-generation caregivers and non-caregivers had the highest proportion of individuals who graduated from college compared to their first generation counterparts. Among both caregivers and non-caregivers, first generation individuals had the lowest incomes.
Table 1. Weighted demographic characteristics of the sample (n = 13,161)

a Unweighted sample size.
b Mean and standard error for continuous variables and percentages for categorical variables.
c Asian American Pacific Islander.
Factors associated with psychological distress
Table 2 shows the results of the separate regression models. Model 1 showed that first-generation caregivers had more distress than first-generation individuals who were not caregivers (β = 0.92, 95% CI: (0.18, 1.65)); moreover, the difference in distress level between caregivers and non-caregivers was smaller in the third generation than in the first (β = −1.21, 95% CI: (−2.24, −0.17)). Among non-caregivers, those in the third generation had more distress than those in the first generation (β = 0.82, 95% CI: (0.22, 1.42)). Figure 1 illustrates the significant interactions. In Model 2, caregivers had higher levels of distress than non-caregivers among those interviewed in a language other than English relative to those assessed in English (β = 1.17, 95% CI: (0.13, 2.22)). The difference in distress was not significant between caregivers and non-caregivers who were interviewed in English (p = 0.15). In Model 3, results were consistent in that among those with low English proficiency, caregivers had higher psychological distress than non-caregivers (β = 2.60, 95% CI: (1.21, 3.98)); this difference was not as large among those proficient in English (β = −2.28, 95% CI: (−3.65, −0.91)). There was no evidence to suggest that the association between acculturation and caregiving status differed by race/ethnicity or gender for each of the three-way interactions (results not shown).

Figure 1. Generation status, interview language, and English proficiency by caregiver status interaction on psychological distress. Model adjusts for continuous covariates centered at the mean. Caregiving status is a dichotomous variable.
Table 2. Multivariate regression of variables associated with psychological distress a
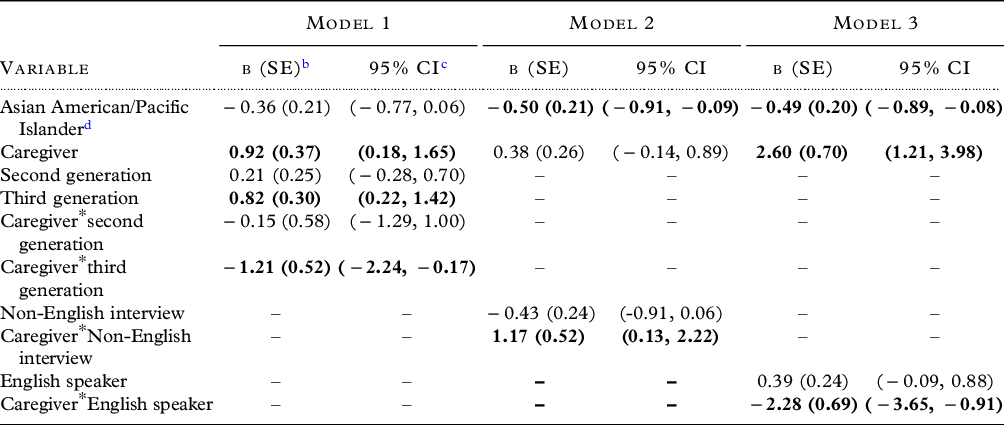
a Unstandardized regression coefficient estimates and their standard errors from the regression models are reported.
b Standard error.
c Confidence interval.
d Reference categories are Latino, first generation, non-caregivers, English interview, and non-English proficient speaker.
Each model used a different acculturation proxy: Model 1 – generational status; Model 2 – language of interview; Model 3 – English language proficiency. All models adjusted for education, gender, marital status, age, income, neighborhood safety and self-reported health. Bolded values have p < 0.05.
Discussion
We hypothesized that individuals who were more acculturated would experience more psychological distress, and that the additional role of being a caregiver to an older adult would further exacerbate this distress. That is, acculturated caregivers would have the highest levels of distress. Our results only partially confirmed our hypothesis. The healthy immigrant hypothesis was supported in our findings with non-caregivers, while findings among caregivers were indicative of models of acculturative stress. Among caregivers, those who were less acculturated experienced more psychological distress than those who were more acculturated. These acculturation–distress associations were supported in all acculturation proxy models – generational status, language of interview, and English language proficiency. Furthermore, race/ethnicity did not moderate these associations: the association between acculturation proxies and psychological distress was the same in both Latinos and AAPIs.
Acculturative stress is induced when there are pressures to adapt to a lifestyle and environment that is different from those in the native country and is exacerbated when an individual cannot reconcile and adapt to these changes (Berry, Reference Berry1970). Acculturative stress can affect multiple generations, and can be intensified for first-generation immigrants who are also caregivers (Cervantes et al., Reference Cervantes, Padilla, Napper and Goldbach2013). These individuals may face significant limitations to accessing psychological and social resources including support networks and educational and financial resources compared to their counterparts in later generations (Cervantes et al., Reference Cervantes, Padilla, Napper and Goldbach2013; Sörensen and Pinquart, Reference Sörensen and Pinquart2005). Caregiver burden studies have shown worse psychological distress outcomes among those with low-resource accessibility (Sörensen and Pinquart, Reference Sörensen and Pinquart2005). Furthermore, we found that caregivers who did not speak English well or completed the interview in a language other than English also experienced higher distress. This suggests that linguistic barriers may underlie this lack of resource accessibility and acculturative stress experienced by first-generation caregivers.
In alignment with the healthy immigrant effect, our study found that among non-caregivers, first-generation immigrants reported lower psychological distress than third generation. Both mechanisms proposed by the healthy immigrant effect, self-selection, and the salmon bias theory support our findings among less acculturated individuals (who were not caregivers). Self-selection is a premigration process and suggests that only the “healthiest” individuals leave their country and emigrate to the new host country. Salmon bias occurs when acculturative stress drives those who are unable to thrive in the host country to return to their country of origin (Abraído-Lanza et al., Reference Abraído-Lanza, Dohrenwend, Ng-Mak and Turner1999). Our results suggest that less acculturated non-caregivers, or rather first-generation immigrants, who experienced more acculturative stress, possibly caused by language barriers associated with having low-English proficiency, may return to their country of origin, while their counterparts who are caregivers might stay due to their caregiving responsibilities (Abraído-Lanza et al., Reference Abraído-Lanza, Echeverría and Flórez2016; Palloni and Arias, Reference Palloni and Arias2004). However, this speculation requires more in-depth study in future research.
In our study, two language variables served as the acculturation proxies: English proficiency and language of interview. In alignment with models of host language use as a proxy for acculturation, we found that both caregivers who were interviewed in a language other than English and those who were not proficient in English (i.e., less acculturated) had significantly higher psychological distress. These associations using the language variables mirrored results we obtained for generational status. Differences in psychological distress by acculturation status were much larger when English language proficiency was the proxy rather than language of interview. This difference was especially apparent among caregivers, in which the difference in psychological distress between less acculturated and more acculturated individuals was almost twice as large when using English proficiency rather than using language of interview. Thus, although both English proficiency and language of interview seem to mirror one another in their associations with psychological distress, they varied in strength as predictors, suggesting the importance of using varied language-based acculturation proxies.
Our results can also be understood in the context of a structural model of acculturation which acknowledges the role of structural barriers to acculturation (California Health Interview Survey, 2012 Castañeda et al., Reference Castañeda, Holmes, Madrigal, Young, Beyeler and Quesada2015; Viruell-Fuentes, Reference Viruell-Fuentes2007). For example, our findings indicated that third-generation individuals reported higher neighborhood safety scores than first- and second-generation non-caregivers. Furthermore, first-generation caregivers experienced more distress than second- and third-generation caregivers. Analysis of socioeconomic variables within the caregiver group revealed that first-generation caregivers had the lowest proportion of college graduates and lowest annual incomes compared with first-generation non-caregivers and caregivers in later generations. These results highlight that structural and contextual factors, such as education and financial resources, may contribute to health disparities among first-generation caregivers in both Asian and Latino immigrants.
Our study was not without limitations. We did not disaggregate findings based on AAPI or Latino ethnicity, and we know that within-group heterogeneity can be quite large in these populations. However, these groupings allowed us to observe psychological distress across broader populations and to test for interactions. Our findings may not be generalizable to individuals living outside of California, who may have different resources for caregiving. The 2009 CHIS had a response rate of 36.1% which raises concerns about selection bias (California Health Interview Survey, 2012). Although we know that caregivers were caring for an adult, because CHIS did not collect data on the care recipient’s characteristics (e.g., health problems and presence of dementia), we were unable to control for these important characteristics. Perceptions of neighborhood safety may be indicative of anxiety or negative affect rather than objective features of the neighborhood. The latter should be combined with subjective measures of neighborhood safety in future research (Robinette et al., Reference Robinette, Piazza and Stawski2021). Finally, although we are confident in the robustness of our results given consistent findings across acculturation proxies, future research should include a validated acculturation measure in addition to using proxies such as generational status and language use/proficiency.
To our knowledge, this study is the first to examine the relationship between multiple acculturation proxies and their impacts on psychological distress in caregivers and non-caregivers in a large, diverse, and population-based sample. Using three related but different measures allows for checking the robustness of the relation between acculturation and psychological distress. Our results showed that that among caregivers, differences in psychological distress were about 1–1.8 points between those who were least acculturated and those who were most acculturated. While these are relatively small effects for a scale that ranges from 0 to 24, identifying factors associated with any change in distress are theoretically important and can inform targets for intervention. In addition, our study highlights the need to build on discussion of within-group differences for understanding caregiver distress. Psychological distress and demographic variables of first-generation immigrants and subsequent generations differed markedly from each other (e.g., income level). Acculturation and generational differences need to be further dissected to create interventions and resources for caregivers that are context relevant. As US immigration policies continue to change rapidly, it is important to expand our understanding of how health disparities among first-generation and limited English proficient immigrants manifest, especially among those who may experience additional resource constraints due to their dual roles as immigrants and caregivers. Our study expands the sociocultural caregiving literature by demonstrating that nuances within AAPI and Latino racial/ethnic groups, such as level of acculturation, may have profound impacts on caregiver outcomes.
Conflict of interest
The authors have no conflict of interest. This research was partially supported by the National Institute on Aging [P30AG072972, K01AG052646, R01AG067541, and R24AG063718] and the Alzheimer’s Association [AARGD-19-619832]. The sponsors had no role in the conduct of the research.
Description of authors’ roles
JN formulated the research question, led the literature review, and wrote the manuscript. KZ and DH were responsible for the statistical analysis and interpretation and writing of the results. DH assisted with conceptualizing the study and assisted in writing the literature review. QD assisted in putting the results together. OM assisted in formulating the research question and guiding the conceptualization of the study. All authors assisted in writing the manuscript.



