



Introduction
Image-guided radiotherapy (IGRT) is a well-established means of improving accuracy of daily external beam therapy for a range of tumours including prostate cancer. Reference Dang, Cao, Kishan, Agazaryan and Kupelian1 The process involves daily pre-treatment imaging of the patient to verify the treatment position Reference Dang, Cao, Kishan, Agazaryan and Kupelian1,Reference Goyal and Kataria2 which is then compared with the planned isocentre position. IGRT can detect positional changes of the prostate arising from internal organ variation, typically due to bowel gas or bladder variability. Reference Dang, Cao, Kishan, Agazaryan and Kupelian1,Reference Goyal and Kataria2 Cone-beam computed tomography (CBCT) is the most commonly adopted imaging modality for IGRT Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3–Reference Osman, Russell and King5 and can be used to support manual matching of structures by eye or automated matching by software algorithms. Reference Dang, Cao, Kishan, Agazaryan and Kupelian1–Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3 Matching can be performed in three orthogonal planes, but the inherent poor soft-tissue contrast, particularly between prostate and muscular tissues, inhibits matching and can potentially lead to reduction in accuracy, increased treatment times and risk of intra-fraction errors. Reference Osman, Russell and King5 A common aid to visualisation of the prostate for IGRT is the use of implanted gold fiducial markers (FM). Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3,Reference McNair and Buijs4 FM matching can speed up both manual and automated matching processes and has been shown to reduce planning target volume (PTV) margins for prostate-only treatments. Reference Dang, Cao, Kishan, Agazaryan and Kupelian1,Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3,Reference Beltran, Herman and Davis6 However given the variability and independence of motion between the prostate and pelvic nodes, Reference Björeland, Jonsson, Alm, Beckman, Nyholm and Thellenberg-Karlsson7 CBCT may be superior for these patients to ensure complete positional verification. Barney et al. identified a preference for FM-based matching due to reduced daily radiographer input and reduced time requirement. Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3 Daily manual registration of FM has also been shown to be more reliable in maintaining accuracy than CBCT with soft-tissue-based automatic corrections. Reference Shi, Li and Zlotecki8
While FM-based IGRT is considered safe and effective, the transrectal implantation procedure has been linked to pain, dysuria, haematuria, bleeding from the rectum, and urinary infection. There is also a concern about the danger of post-operative multi-drug-resistant infectious disease. Reference Deegan, Owen and Holt9,Reference Saad, Goldstein and Lawrence10
‘UroLift’ implants are an increasingly utilised means of relieving obstructive urethral symptoms arising from benign prostatic hyperplasia. Reference Denisenko, Somani and Agrawal11–Reference Roehrborn, Chin and Woo13 This minimally invasive surgery involves the insertion of four implants, each comprising two brackets connected by a suture as seen in Figure 1. One bracket embeds in the prostatic capsule, while the other stays in the urethra lumen; the resulting combined strain from the sutures opens the prostate lumen. UroLift implantation causes minor and short-lasting (1-month) occasional side effects of irritation, dysuria and haematuria, Reference Denisenko, Somani and Agrawal11 does not require hospital admission and has been shows to improve sexual function Reference Tastemur, Yilmaz, Kasap, Olcucuoglu and Ardicoglu14 compared to transurethral resection of the prostate.
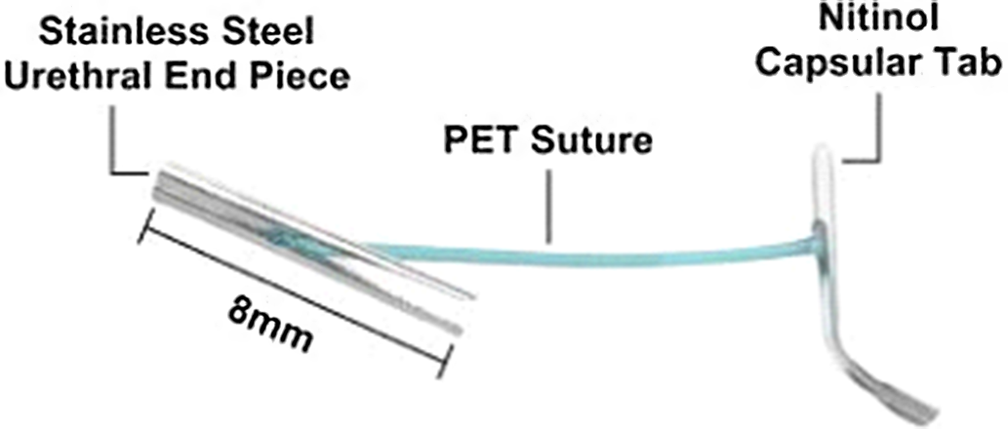
Figure 1. Schematic of the UroLift implants (courtesy of Teleflex Medical Limited).
There is increasing interest in the possibility of using extant UroLift implants in lieu of FMs. The implants are situated in prostate tissue and are radio-opaque, so visualisation of these could be a feasible alternative means of confirming treatment position on a daily basis. Reference Keehn, Fram, Garg and Maria15,Reference Biswal, McKenna, Singh and Swann16 This would eliminate the overall cost and time of an extra procedure for the increasing numbers of patients presenting with the UroLift system in place. Reference Ray, Morgan, Wilkes, Carter and Carolan-Rees17 Indeed, the prevalence of obstructive dysuria arising in prostate radiotherapy patients has been highlighted as a potential rationale for replacing FM with UroLift. Reference Keehn, Fram, Garg and Maria15
Both Keehn Reference Keehn, Fram, Garg and Maria15 and Biswal Reference Biswal, McKenna, Singh and Swann16 identified how the radio-opaque UroLift implants could be used for orthogonal image matching, yet there is a paucity of research on their use as a FM substitute in CBCT matching, and accordingly this study aimed to evaluate the feasibility of this technique for a single case.
Method
Patient selection
This study was classed as a service evaluation and approved by the local clinical audit committee. The dataset in this study comprised a series of both planar kilovoltage and CBCT images from a prostate cancer patient who had previously received radical external beam radiotherapy to their prostate, seminal vesicles and pelvic nodes. All therapy and imaging had been performed on a Varian OBI Linac. Prior to radiotherapy, the patient had undergone an UroLift system implantation.
At the time of treatment, the imaging protocol included both daily kV imaging and CBCT on days 1–3. The frequency of CBCT was then reduced to weekly, with additional images scheduled as required. In total, throughout the duration of treatment, 32 kV images and 10 CBCT scans were taken. Copies of all patient and imaging data were fully anonymised before being passed forward for data collection.
Data Collection
Volunteers were invited from the treatment radiographers within the department who had experience of image registration for prostate patients. Volunteers were requested to perform manual co-registration of the cone-beam CT images with the planning CT images. This was performed for each image using two approaches:
A UroLift clip match ‘CBCTUroLift’
A soft-tissue (prostate only) match ‘CBCTProstate’
The Urolift match was performed first for all participants, and the resulting shift values in each orthogonal plane were recorded from both CBCTProstate and CBCTUroLift matches.
Volunteers were also asked to complete a simple questionnaire which asked them to rate the ease of match for each co-registration. The rating scale ran from 0 to 4; 0 = impossible, 1 = barely possible, 2 = possible with difficulties, 3 = possible with little difficulty and 4 = very easy.
Data Analysis
Both CBCTUroLift and CBCTProstate matches were subjected to Bland–Altman analysis using Microsoft Excel. The standard UroLift implant location was first calculated using the mean of the five observers in each plane. The mean and standard deviation of the differences in the methods were then calculated using a limit of agreement (LoA) of 95% with the mean. The clinically acceptable threshold was set at 2 mm for the UroLift alignment and 3 mm for prostate alignment. These threshold values matched those of the clinical department for FM and soft-tissue match and were also used in a similar study. Reference Deegan, Owen and Holt18 Analysis was performed for the five observers’ overall 95% LoA and also for each plane individually.
Results
Overall, there were five participants in this study. Two of the five radiographers had less than 5 years of experience, while the other three radiographers had over 20 years of experience in the field. The group included one pelvic advanced imaging treatment expert practitioner and two consultant radiographers in prostate radiotherapy. The participants reported that the implants were visible on all planes of CBCT images as seen in Figure. 2.
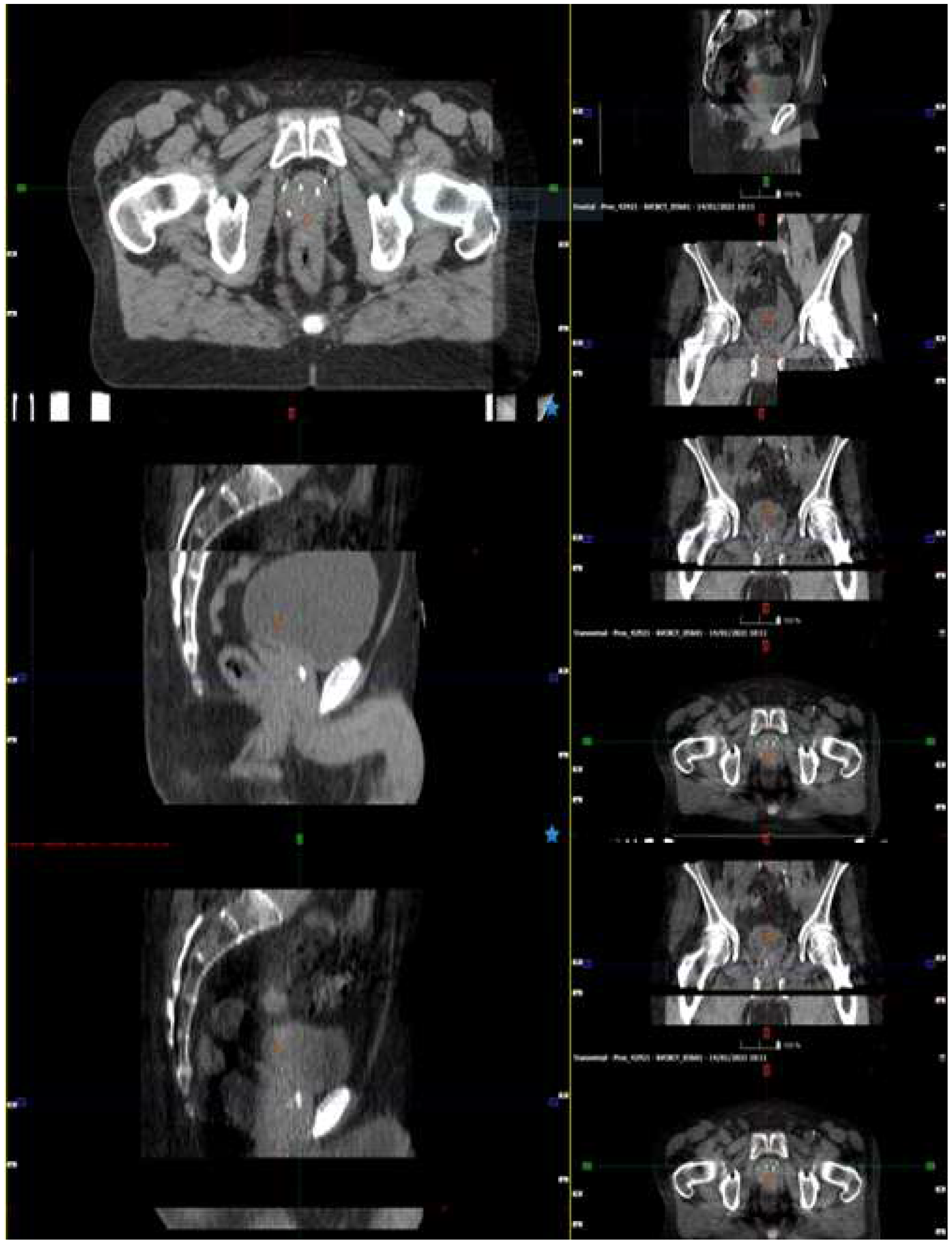
Figure 2. Visibility of UroLift implants on Axial, Sagittal and Coronal images.
Bland–Altman Comparison of Methods
Table 1 illustrates the Bland–Altman comparison between CBCTUroLift and CBCTProstate. The overall mean difference showed a minimal mean shift (0·02mm) with 97% of displacement agreements within the 2-mm threshold. The mean difference between the two methods shows a shift of 0·40 mm anteriorly and 0·39 mm laterally for UroLift matching when compared with prostate tissue matching. This can be seen clearly in the Bland–Altman plot (Figure 3).
Table 1. CBCTUroLift alignment to UroLift CBCTProstate


Figure 3. Bland–Altman plot of overall match.
Directional Dependence
Vertical
There was a 0·40 mm mean difference in the isocentre shift between CBCTUroLift and CBCTProstate match with a standard deviation of 0·71 mm as seen in Figure 4. The percentage of displacement agreements in both 2 and 3 mm thresholds was 96%.

Figure 4. Bland–Altman plot of vertical match.
Longitudinal
There was a 0·04 mm mean difference in the isocentre shift between CBCTUroLift and CBCT prostate match with a standard deviation of 0·27 mm as seen in Figure 5. The percentage of displacement agreements in both 2 and 3 mm thresholds was 100%.

Figure 5. Bland–Altman plot of longitudinal match.
Lateral
There was a 0·39 mm mean difference in the isocentre shift between CBCTUroLift and CBCTProstate match with a standard deviation of 0·73 mm as seen in Figure 6. The percentage of displacement agreements in both 2 and 3 mm thresholds was 96%.

Figure 6. Bland–Altman plot of lateral match.
Match Feasibility
Out of the 25 individual Urolift matches (5 participants using 5 CBCT datasets each), there were 12 scores of 3 (‘possible with little difficulty’) and 13 scores of 4 (‘very easy’). None of the participants gave a score of less than 3.
Discussion
Using FM in prostate matching is the optimal method of localisation as it adds a highly visible landmark to the low-contrast soft-tissue structures. Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3,Reference Shi, Li and Zlotecki8 Unfortunately, some patients are contraindicated for surgery and others refuse FM insertion. Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3,Reference Keehn, Fram, Garg and Maria15 This study’s findings suggest that it is feasible to use UroLift implants in lieu of FM insertion for CBCT matching in these patients and for those who have already had a UroLift procedure.
There were some slight differences in alignments between CBCTUroLift and CBCTProstate, although these were all less than 3 mm in magnitude. One of the likely causes of shift variations over this small number of matches is the image quality of the CBCT. Reference Barney, Lee, Handrahan, Welsh, Cook and Sause3,Reference Shi, Li and Zlotecki8 This in turn can be influenced by motion during the treatment delivery. Reference Létourneau, Martinez and Lockman19–Reference Ingrosso, Miceli and Ponti21
The slight difference in shifts based on CBCTUroLift and CBCTProstate contrasted with those found in a 2015 study by Deegan. Reference Deegan, Owen and Holt9 This work compared CBCT FM matches to a CBCT prostate tissue match and found a lower 95% LoA within a 2-mm threshold than in this study. Their agreements were 84·1%, 94·6% and 76·0% for vertical, longitudinal and lateral, compared to 96%, 100% and 96%, respectively, for this study. According to Deegan’s study, comparing soft-tissue and FM matches was challenging due to the lack of ‘standard’ position for the prostate and its capacity for deformation compared to FMs. Thus, the differences between soft-tissue and FM matches may be due to the FM position not accurately describing the prostate location. Reference Deegan, Owen and Holt9,Reference Ingrosso, Miceli and Ponti21
In our study, the UroLift match was performed before the prostate tissue match by the observers. It was found that the UroLift implants aided in visualising the prostate gland, resulting in faster data collection for the observers on duty. Although Deegan’s participants also used FM to assist them in soft-tissue match, a significant difference was still observed between their matching methods compared to the UroLift matching.
Ease of Match
Only a few papers have reported ratings of match quality. Delouya Reference Delouya, Carrier, Béliveau-Nadeau, Donath and Taussky22 discovered that matching was easy in 77% of 31 cases and challenging in only 6·5%, while Chung Reference Chung, Haycocks and Brown23 reported easy matches in 85% of 17 patients’ imaging data. Our lower rate of 40% of CBCT matches deemed ‘Easy’ suggests that UroLift implants are not as visible as FM but with no scores indicating difficulties, it is clear that an Urolift-based match is feasible on CBCT for this patient. The impact of body mass index (BMI) on image quality Reference Wood, Moore, Horsfield, Saunderson and Beavis24 should be acknowledged at this point; for the single case presented, this was not an issue.
Limitations
The volunteers performing the matches had a variation in their levels of experience, which may result in a slight difference in the results. A wider sample comprising only highly experienced radiographers may have improved the consistency of the co-registration. In addition, due to low numbers, randomisation of order of the matching was not feasible, so all participants matched with Urolift first. It is possible that this influenced the subsequent soft-tissue match.
Other limitations arose from the use of a sole patient dataset at one clinical site only. Participants were not asked how easy the soft-tissue match was for this patient for comparison with Urolift matching. Feasibility of this match was, however, proven as the patient had previously had successful matching during treatment.
Following this preliminary feasibility test, a larger study with a large sample size is being planned to provide formal comparison of matches along with timing and ease of use data. This will include multiple patients with a range of BMI.
Conclusion
This quantitative, single-case-based feasibility study has shown clinically acceptable agreement between the two methods of CBCT matching. Radiographers were able to use UroLift implants on CBCT images to perform retrospective image matching to the prostate efficiently and accurately.
Future work should expand on this feasibility study to identify the value of this method within a large patient cohort. It would also be useful to identify how feasible this method would be using planar kV images produced by new high-resolution detectors.
Acknowledgements
The authors wish to acknowledge the kind assistance of the study participants
Conflicts of Interest
There are no conflicts of interest







