



Introduction
Common mental health problems, such as anxiety and depression are a leading cause of disease burden (Whiteford et al., Reference Whiteford, Degenhardt, Rehm, Baxter, Ferrari, Erskine and Vos2013). Estimated high prevalence of common mental health problems in children and adolescents is of particular concern as early onset symptoms often persist into adulthood (Last, Hansen, & Franco, Reference Last, Hansen and Franco1997; Pine, Cohen, Gurley, Brook, & Ma, Reference Pine, Cohen, Gurley, Brook and Ma1998), causing substantial health and social costs in adult life (Colman et al., Reference Colman, Murray, Abbott, Maughan, Kuh, Croudace and Jones2009; Goodman, Joyce, & Smith, Reference Goodman, Joyce and Smith2011; Ploubidis, Batty, Patalay, Bann, & Goodman, Reference Ploubidis, Batty, Patalay, Bann and Goodman2021). Mental ill-health frequently occurs in childhood and adolescence, with one in eight 5–19 year olds with a diagnosable disorder and a higher proportion of young people reporting high levels of internalising and externalising symptoms (Deighton et al., Reference Deighton, Lereya, Casey, Patalay, Humphrey and Wolpert2019; Sadler et al., 2018). It has also been observed that the prevalence of mental ill-health symptoms is changing across generations, with twice as many young people in the UK reporting frequent feelings of depression and anxiety from 1986 to 2006 (Collishaw, Maughan, Natarajan, & Pickles, Reference Collishaw, Maughan, Natarajan and Pickles2010), and almost twice as many adolescents experiencing high depressive symptoms in 2015 compared to 2005 (Patalay & Gage, Reference Patalay and Gage2019).
Studies providing evidence for the association between adolescent mental ill-health and psychosocial adult outcomes have been recently reviewed (Clayborne, Varin, & Colman, Reference Clayborne, Varin and Colman2019; Erskine et al., Reference Erskine, Norman, Ferrari, Chan, Copeland, Whiteford and Scott2016), highlighting that adolescent mental ill-health has negative associations with several domains in adulthood, including socio-economic outcomes and physical and mental health. However, it is unclear whether the magnitude of these associations is also changing across cohorts. Investigating this may help inform health policy and planning in relation to the consequences and burden associated with increasing trends in adolescent mental health problems. Studies of adulthood outcomes in relation to adolescent mental health have been conducted using the British birth cohorts (Colman et al., Reference Colman, Murray, Abbott, Maughan, Kuh, Croudace and Jones2009; Goodman et al., Reference Goodman, Joyce and Smith2011; Richards et al., Reference Richards, Collis, Hackett, Hotopf, Kuh, Jones and Parsonage2009), but with one recent exception examining alcohol outomes (Ning, Patalay, Maggs, & Ploubidis, Reference Ning, Patalay, Maggs and Ploubidis2021), to our knowledge no investigations of differences between cohorts has been undertaken to-date, possibly due to the requirement of a sequence of long running longitudinal studies to do so. A recent study investigated the association between childhood mental health difficulties at age 7 and adolescent outcomes (14–16 years) in three cohorts and their findings indicate that these associations are similar magnitude across cohorts and might be getting slightly stronger for some outcomes in recent generations (Sellers et al., Reference Sellers, Warne, Pickles, Maughan, Thapar and Collishaw2019).
In adolescent mental health, common difficulties are usually represented in two domains, internalising and externalising symptoms, which exhibit above chance levels of co-morbidity and have common antecedents (Patalay, Moulton, Goodman, & Ploubidis, Reference Patalay, Moulton, Goodman and Ploubidis2017). Internalising psychopathology is indicated by a liability to experience mood and anxiety related symptoms, whereas externalising psychopathology is indicated by a liability to experience antisocial behavioural related symptoms, substance use disorders, childhood oppositional defiance/conduct disorder, and adult antisocial personality (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Krueger et al., Reference Krueger, Hicks, Patrick, Carlson, Iacono and McGue2002). Regarding adult outcomes, there is some evidence that externalising difficulties might have stronger negative associations with educational and economic outcomes (Colman et al., Reference Colman, Murray, Abbott, Maughan, Kuh, Croudace and Jones2009; Richards et al., Reference Richards, Collis, Hackett, Hotopf, Kuh, Jones and Parsonage2009). However, it is unclear whether this is still the case when the shared variance with internalising symptoms is accounted for. In recent years, to account for their comorbidity and permit investigation of overall levels of mental health difficulties, mental health has been conceptualised as a general psychopathological construct that reflects shared variance between internalising and externalising symptoms (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Lahey et al., Reference Lahey, Applegate, Hakes, Zald, Hariri and Rathouz2012). In young people this general psychopathology factor explains between 70% and 80% of the variance in symptomology, and is highly predictive of future outcomes (McElroy, Belsky, Carragher, Fearon, & Patalay, Reference McElroy, Belsky, Carragher, Fearon and Patalay2018; Patalay et al., Reference Patalay, Fonagy, Deighton, Belsky, Vostanis and Wolpert2015).
The current study aimed to investigate whether cohort moderated the strength of associations between adolescent psychopathology (at age 16) and a wide range of health and wellbeing, social and economic outcomes in mid-life (at age 42) using simultaneous analysis of identically measured exposure, outcomes, and controls across the 1958 National Child Development Study and the 1970 British Cohort Study. In addition, adolescent mental health was conceptualised as traditional two-domains (internalising and externalising difficulties) and also using a more recent bi-factor general psychopathology approach. A range of health and wellbeing (mental health, general health, life satisfaction), social (cohabitation, voting behaviour) and economic (education and employment) outcomes were investigated to provide a comprehensive picture of the health and socioeconomic consequences related to adolescent mental health and whether these are changing across cohorts.
Methods
Participants
This study used data from 31 349 participants from two British birth cohort studies.
1958 NCDS
The 1958 National Child Development Study (1958 NCDS) follows the lives of 17 415 people born in England, Scotland and Wales in a single week of 1958 (Power & Elliott, Reference Power and Elliott2006). Since the birth survey in 1958, there have been 11 further surveys of the cohort members at ages 7, 11, 16, 23, 33, 42, 44, 46, 50, 55 and 62 years. In 2000 at age 42 years, 11 419 study members (50.7% female) participated in the survey. The analytic sample for this study consisted of 16 091 participants (92.39% of the original sample) having excluded those who had died or emigrated by age 42 years.
1970 BCS
The 1970 British Cohort Study (1970 BCS) follows the lives of 17 198 people born in England, Scotland and Wales in a single week of 1970 (Elliott & Shepherd, Reference Elliott and Shepherd2006). Since the birth survey in 1970, there have been ten surveys at ages 5, 10, 16, 26, 30, 34, 38, 42, 46 and 50 years. In 2012 at age 42 years 9841 study members (52.20% female) participated in the survey. The analytic sample for this study consisted of 15 258 participants (88.72% of the original sample) having excluded those who had died or emigrated by age 42 years.
Measures
Mental health at age 16
At age 16 one parent (usually the mother) of both 1958 NCDS and 1970 BCS cohort members completed the Rutter A scale (Rutter, Reference Rutter, Tizard and Whitmore1970), consisting of 18 symptoms for which the parent was asked to indicate whether each ‘does not apply’, ‘applies somewhat’ or ‘definitely applies’. Confirmatory 2-factor and bi-factor analyses were applied to derive latent factor scores, which were treated as continuous measures of internalising and externalising symptoms and general psychopathology.
Health and wellbeing outcomes at age 42
At age 42 psychological distress was measured in both cohorts using the nine item version of the Malaise Inventory (Rodgers, Pickles, Power, Collishaw, & Maughan, Reference Rodgers, Pickles, Power, Collishaw and Maughan1999), which includes items assessing presence of symptoms such as ‘feel miserable and depressed’, ‘get worried about things’ and ‘get easily upset or irritated’. On the sum score, a high score indicates greater psychological distress and there is an established cut-off of a score of above 3 indicating high psychological distress (Ploubidis, Sullivan, Brown, & Goodman, Reference Ploubidis, Sullivan, Brown and Goodman2017; Rutter, Tizard, Yule, Graham, & Whitmore, Reference Rutter, Tizard, Yule, Graham and Whitmore1976).
Life satisfaction was assessed by the question ‘How had life turned out so far’: on a scale of 0–10, where 0 is not at all satisfied and 10 is completely satisfied. General state of health was also measured in both cohorts at age 42. In the 1958 NCDS cohort members were asked to rate their general health using four categories (1 = Excellent, 2 = Good, 3 = Fair, 4 = Poor), and in the 1970 BCS cohort members were asked to rate their general health using five categories (1 = Excellent; 2 = Very good; 3 = Good; 4 = Fair; 5 = Poor). To harmonise this variable, the linear stretch method was applied to each general health measure (de Jonge, Veenhoven, & Arends, Reference de Jonge, Veenhoven and Arends2014).
Social and economic outcomes at age 42
Whether the cohort member lives with a spouse or partner, their highest academic qualification, their employment status (managerial/professional/non-managerial/professional/never worked/long-term unemployed), and whether the cohort member voted in the last general election was recorded in both cohorts at age 42. A binary variable was derived for highest academic qualification, which represented those who had a degree (coded 1) v. those who had no or other qualifications (coded 0). A binary variable was also derived for employment status which represented those in professional managerial positions (coded 1) v. those in any other employment status.
Covariates
Socio-economic and health covariates derived from birth and early childhood were included in the analysis. All covariates were measured identically between cohorts.
Covariates derived from birth and early childhood included birth weight, maternal smoking during pregnancy, whether cohort members were breastfed, childhood cognition and childhood body mass index. Covariates derived from parents included paternal social class at age 10/11 years (higher managerial, administrative and professional occupations, intermediate occupations, routine and manual occupations), housing tenure of parents at age 10, whether the mother of the participants was employed (birth to age 5 years), divorced (by age 10 or 16 years), and years of education of mother and father.
Statistical analysis
Latent variable measurement models
Measurement models were estimated with the age 16 mental health measure. Confirmatory factor analyses (CFA) were conducted to test two models. A 2-factor model was estimated which confirmed the factor structure for internalising and externalising psychopathology. Second, a bi-factor model where each symptom loads on to general psychopathology as well as internalising and externalising factors. CFA models were estimated using Mplus 8 (Muthén & Muthén, Reference Muthén and Muthén2013) and the weighted least square mean and variance estimator was used for categorical manifest variables (Beauducel & Herzberg, Reference Beauducel and Herzberg2009). We tested the measure for invariance between cohorts and found it to be invariant at the configural, metric and scalar levels, indicating between cohort comparisons could be made using this measure (see online Supplementary Table S1) (Gregorich, Reference Gregorich2006).
To compare the relative variance explained of both the general and specific factors, the explained common variance (ECV) for each factor was calculated for externalising, internalising and general psychopathology. ECV values range from 0 to 1, with values closer to 1 suggesting a greater share of variance explained. There are no established cut-offs in ECV values; it has been suggested that ECV values ranging from 0.60 to 0.85 indicate that a factor is the main source of shared variance (Reise, Scheines, Widaman, & Haviland, Reference Reise, Scheines, Widaman and Haviland2012).
Missing data
Multiple imputation using chained equations was implemented to impute missing data on all exposures, covariates and outcomes, with 50 imputations conducted separately in both cohorts (see online Supplementary Table S4 for counts and percentages of non-imputed data for each predictor and outcome). This multiple imputation approach includes a number of covariates and auxiliary variables in the models, which improves the plausibility of the missing at random (MAR) assumption (Little, Jorgensen, Lang, & Moore, Reference Little, Jorgensen, Lang and Moore2014; Mostafa et al., Reference Mostafa, Narayanan, Pongiglione, Dodgeon, Goodman, Silverwood and Ploubidis2021).
Regression analyses
Linear and logistic multivariable regression models were fitted to test associations between psychopathology at age 16 and health and socio-economic outcomes at ages 42, adjusting for a rich set of early life covariates. Data from both cohorts were combined in a single dataset post imputation and model comparison tests between models with and without cohort interactions were conducted. Where log-likelihood tests indicated that the models with cohort interactions had better fit, we present stratified models by cohort to help illustrate the direction and size of the coefficients in each cohort. Given significant improvements in model fit when including cohort × age 16 mental health interaction terms, stratified models are presented by cohort for all outcomes. We further illustrate the cohort differences in exposure–outcome associations across the distribution of the exposure using predictive margins from the regression models. We also investigated whether associations between adolescent mental health and midlife outcomes differed between sexes using sex*cohort*age 16 mental health interactions. An alpha level of 0.05 was used with adjustment made for rate of false discovery due to multiple outcomes testing using the Benjamini–Hochberg procedure (Benjamini & Hochberg, Reference Benjamini and Hochberg1995). To adjust individual p values using Benjamini-Hochberg procedure, critical values were calculated using the formula (i/m)Q [where ‘i’ is the individual p values rank, ‘m’ is the total number of tests and ‘Q’ is the false discovery rate (FDR)]. The FDR was 5% (i.e. Q = 0.05). Multiple imputation and subsequent analyses were conducted using Stata (V.15).
Results
Factor models
The first CFA estimated the 2-factor model using separate externalising and internalising latent factors. Factor loadings and model fit statistics for this model are displayed in online Supplementary Table S1. The second CFA estimated the bi-factor model with externalising, internalising specific and a general psychopathology bi-factor. Factor loadings and model fit for this model are displayed in online Supplementary Table S2. Estimating the ECV indicates that the general psychopathology factor accounted for 72.1% of the variance in symptoms, externalizing symptoms accounted for 14.8% of the variance and internalising symptoms accounted for 13% of the variance.
Descriptive statistics
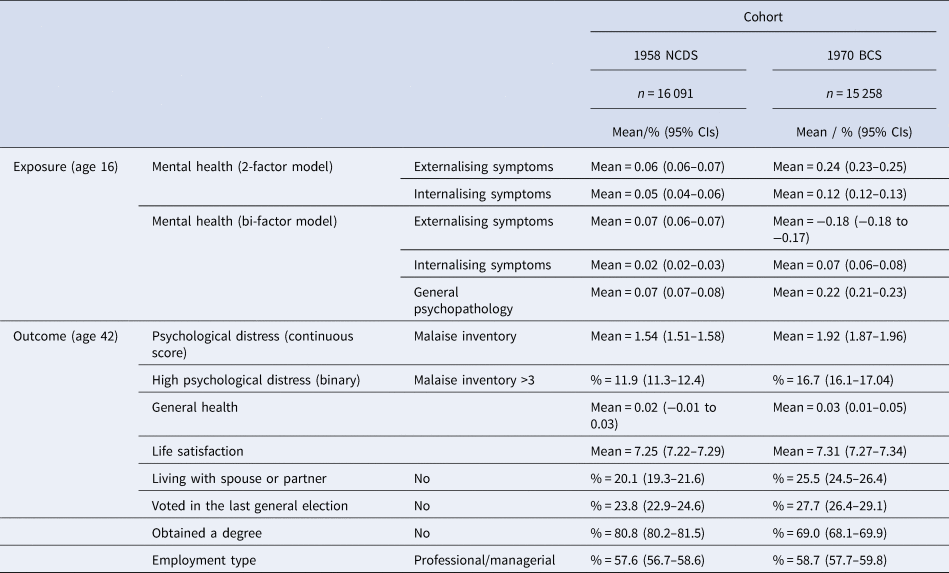
Table 1 displays the mean factor scores for adolescent mental health and the means/proportions for each harmonised outcome variable. Most mental health symptom scores at ages 16 were higher for in the 1970 cohort than for those 1958 cohort (with the exception of the externalising specific factor from the bi-factor model, tests of cohort differences are presented in online Supplementary Table S6). Online Supplementary Table S5 displays the correlations between adolescent mental health and age 42 health and social outcomes. Correlations are similar or of higher magnitude between each exposure-outcome pair for those born in the 1970 cohort than for those in the 1958 cohort.
Table 1. Means/proportions and 95% CIs for exposure and outcome variables
Associations between adolescent mental ill-health and health and social outcomes in adulthood
Model comparison tests of models with and without cohort interactions indicated that for all outcomes models with cohort interactions with age 16 mental health from the bi-factor model (and all except two from the 2-factor model) had an improved model fit than without the cohort interactions, supporting the presentation of cohort stratified estimates (log-likelihood tests for the model comparisons are presented in Table 2).
Table 2. Likelihood ratio tests comparing models with main effects only and cohort interactions to assess cohort differences in associations between age 16 mental health exposures and age 42 outcomes

Note: Results in bold are where log-likelihood difference test indicated differences in models being compared (p < 0.05).
All coefficients for the exposure-outcome associations stratified by cohort are displayed in Table 3. The coefficients describe the change in outcomes associated with one unit increase in the age 16 mental health scores. Histograms describing the distribution of age 16 mental health scores are presented in online Supplementary Figs. S5 and S6 to help illustrate what a unit increase in scores means relative to the population distribution of symptoms.
Table 3. Multivariable regressions estimating associations between adolescent psychopathology and age 42 health and social outcomes in NCDS 1958 and BCS 1970 cohorts
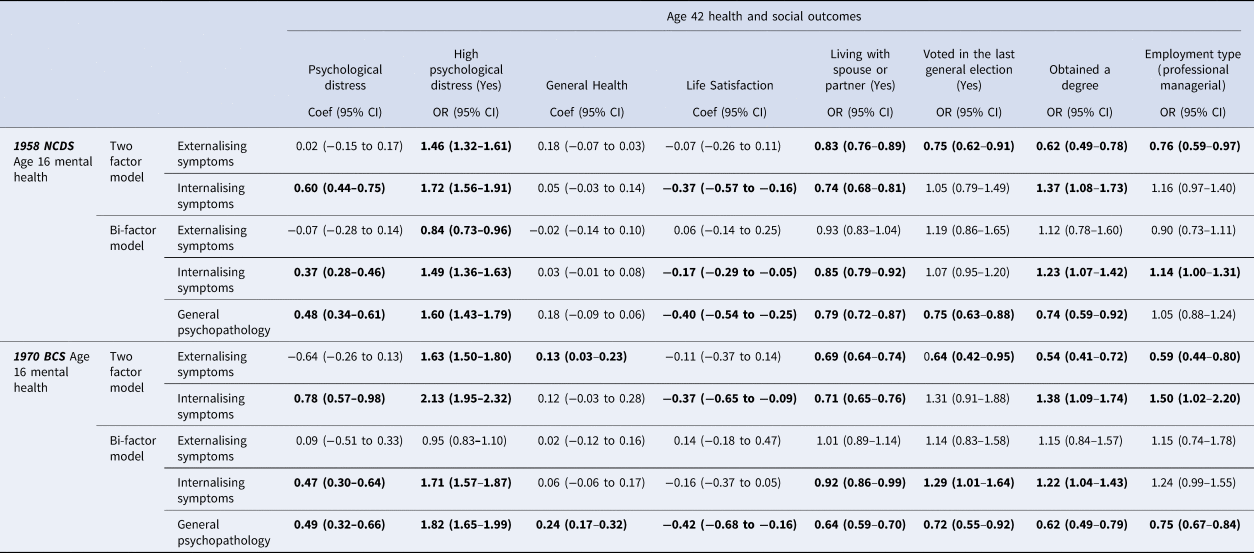
Note. NCDS 1958 (n = 16 091). BCS 1970 (n = 15 258). Models were adjusted using birth weight, maternal smoking during pregnancy, whether cohort members were ever breastfed, childhood cognition, housing tenure, body mass index at age 10/11 years, paternal social class at age 10/11 years, mothers employment status (birth to age 5 years), parental divorce (by age 10 or 16 years), and years of education of mother and father. Note: Coefficients in bold are where the 95% CIs do not cross the null and significant p values are retained after adjusting for multiple testing using the Benjamini-Hochberg procedure.
Externalising symptoms (from the 2-factor model) were associated with high psychological distress and lower likelihood of living with a partner, low education attainment and disadvantaged occupational class in both cohorts, with consistently weaker associations in BCS 1970. Internalising symptoms (from the 2-factor model) were associated similarly in both cohorts with life satisfaction, living with a spouse and obtaining a degree in both cohorts. However, a clear cohort effect is observed for age 42 psychological distress where higher internalising symptoms at age 16 is associated with 1.72 higher odds [95% confidence interval (CI) 1.56–1.91] in NCDS 1958 and 2.13 higher odds (95% CI 1.95–2.32) in BCS 1970 (online Supplementary Fig. S1 illustrates associations by cohort for each 2-factor exposure-outcome pair).
General psychopathology at age 16 was associated with poorer outcomes for most adult outcomes examined in both cohorts. Figure 1 illustrates the associations by cohort for general psychopathology and each outcome. We observe that at higher levels of adolescent difficulties, for several outcomes, including psychological distress, general health, higher education attainment, and employment, the associations with adverse adult outcomes are greater in the BCS 1970 cohort. For instance, age 16 mental health is not associated with lower likelihood of higher occupational class in the NCDS 1958: odds ratio (OR) 1.05 (0.88–1.24) whereas it is associated with substantially lower odds of higher occupational class in the BCS 1970 cohort: OR 0.75 (0.67–0.84).
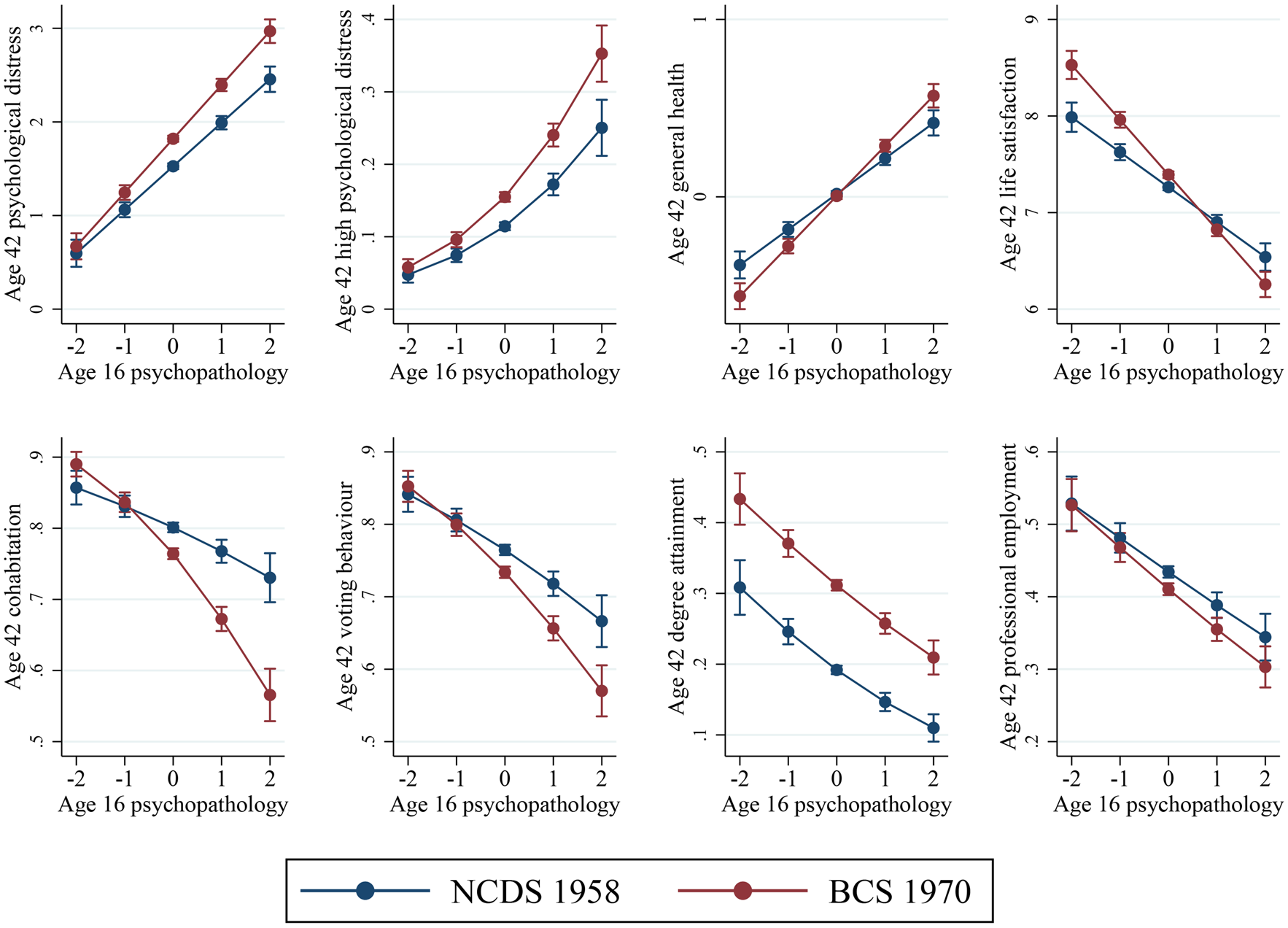
Fig. 1. Predicted probabilities or means of each outcome at age 42 (y-axis) demonstrating associations with mental health (from the bi-factor model) at age 16 (x-axis) in the two cohorts
After accounting for the shared variance associated with general psychopathology, there was one independent association between externalising symptoms and lower levels of psychological distress for the NCDS 1958. No associations between externalising symptoms (from the bi-factor model) and any of the other outcomes tested were significant in either cohort. Internalising symptoms (from the bi-factor model) were still independently associated with several adulthood outcomes including greater psychological distress, lower life satisfaction, and lower likelihood of cohabitation; however, the specific internalising symptoms were associated with attaining a higher degree. Online Supplementary Fig. S2 illustrates the associations by cohort for externalising and internalising bi-factor exposure-outcome pairs.
We also conducted log-likelihood tests with models including sex*cohort interactions to examine whether the exposure-outcome associations across cohorts were moderated by sex (Table 2). For most exposure-outcome associations, the models including sex interactions did not have better model fit, indicating that cohort differences observed are similar for males and females. A consistent exception was psychological distress at age 42 years, where we observe that the cohort effect is starker in males with either externalising and internalising mental health at age 16 (from 2-factor model) and the bi-factor (see Fig. 2 and online Supplementary Fig. S3). For likelihood of cohabitation we see that the lower likelihood by greater age 16 mental health difficulties are similar in males and females in the 1970 cohort, however, in the 1958 cohort this association was not observed in females and lower likelihood of cohabiting was only observed in males (see Fig. 2) and there is evidence of cohort effects being moderated by sex for professional occupations (see online Supplementary Fig. S4).
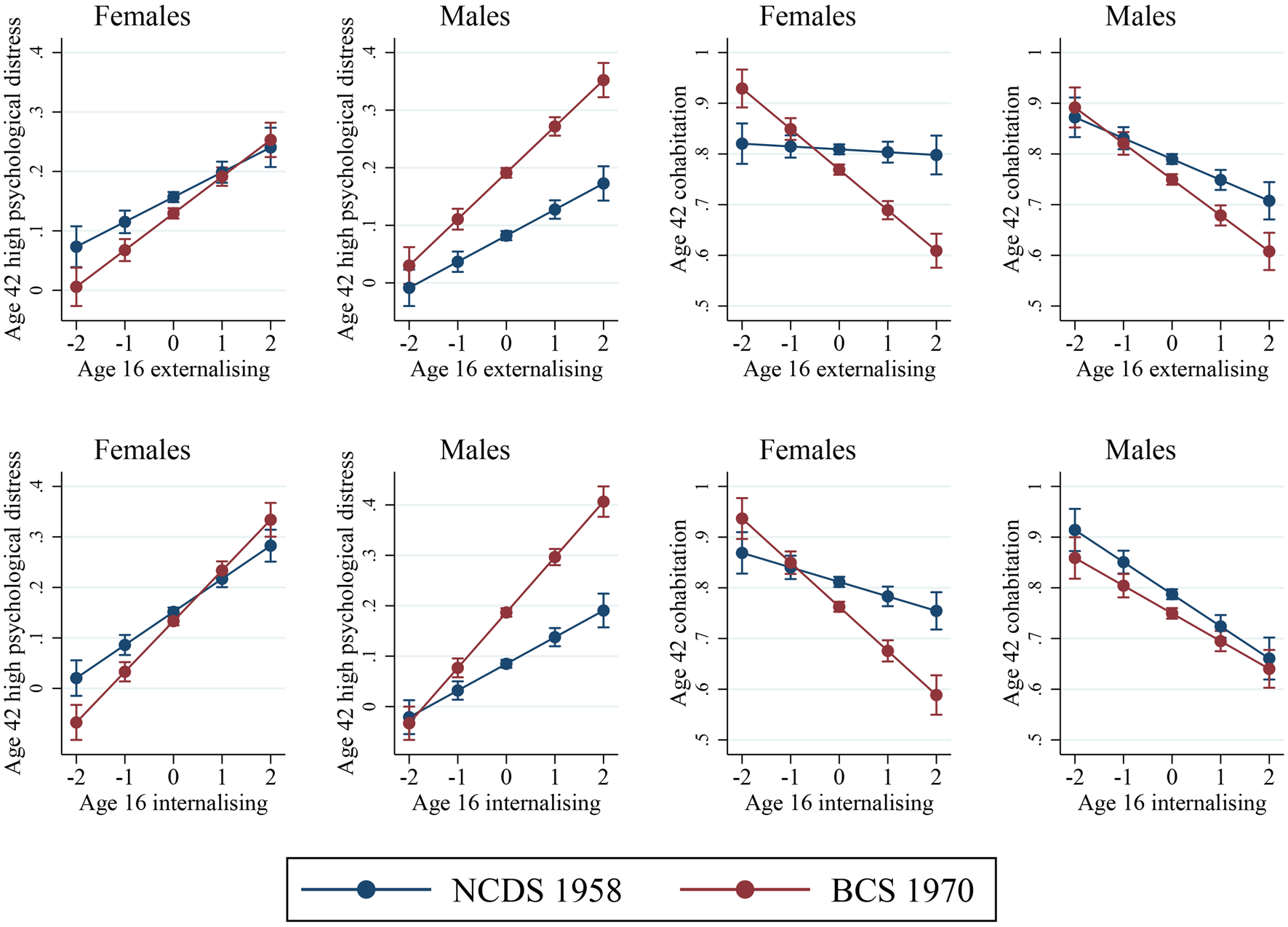
Fig. 2. Predicted probabilities or means in males and females for mental health at age 16 from the two-factor model (x-axis) association with high psychological distress and cohabitation at age 42 in the two cohorts.
Discussion
The findings of the paper highlight that the consequences of early life mental ill-health on a wide range of mid-life outcomes were stronger for many examined outcomes (or did not substantially change) in a cohort born in 1970 compared to a generation prior born in 1958. Alongside growing prevalence of adolescent mental health difficulties, which we also observe between these two cohorts, the larger mental health-based inequalities in life outcomes in the more recently born cohort call attention to the large and increasing public health and societal burden of mental ill-health through the life-course.
The associations between early life mental ill-health and mid-life social and economic outcomes followed a consistent general pattern of direction of effects in both cohorts, however, the magnitude of these associations became stronger in the younger generation for certain outcomes predicting greater mid-life mental health, lower likelihood of co-habitation with a partner, likelihood to vote and being in professional employment. For instance, greater general psychopathology at 16 was associated with a 60% increased risk of mid-life psychological distress in the 1958 cohort and 82% increased risk in the 1970 cohort. In another example, adolescents with higher symptoms were 21% less likely to be in cohabiting relationship at age 42 in the 1958 born cohort, whereas they were 36% less likely to be co-habiting in the 1970 born cohort. If sustained in the long term in more recently born cohorts (e.g. Millennium Cohort Study, born 2000–2001), a hypothesis we cannot currently test with the available data, this trend will likely have a considerable societal and public health impact.
Some cohort effects were also gendered, and we observe starker cohort differences in males in relation to their mid-life psychological distress and starker cohort differences in females in relation to their likelihood of being in a partnership in mid-life. Reasons for this gendered pattern need better understanding and in regard to mental health outcomes, might reflect greater stigma faced by males preventing them for help seeking despite a greater number experiencing mental health difficulties in recent cohorts (Patalay & Gage, Reference Patalay and Gage2019).
With respect to how adolescent mental health was conceptualised, internalising symptoms were associated with higher psychological distress, a higher likelihood obtaining a degree, and poorer life satisfaction at age 42 years. This also remains the case for most outcomes (excluding life satisfaction), when using a specific internalising factor accounting for covariance with externalising symptoms in the bi-factor model. Externalising difficulties were associated with poorer general health, voting behaviour and degree attainment, however, this was no longer the case when accounting for the covariance between internalising and externalising symptoms using the bi-factor model. The findings from the 2-factor model of internalising and externalising symptoms are in line with previous literature which shows both domains are associated with poorer outcomes (Clayborne et al., Reference Clayborne, Varin and Colman2019; Colman et al., Reference Colman, Murray, Abbott, Maughan, Kuh, Croudace and Jones2009; Erskine et al., Reference Erskine, Norman, Ferrari, Chan, Copeland, Whiteford and Scott2016; Richards et al., Reference Richards, Collis, Hackett, Hotopf, Kuh, Jones and Parsonage2009). Notably however, the bi-factor approach which allows us to account for the high levels of shared variance between these domains, highlights that most of the negative associations are predicted by the general psychopathology bi-factor. This finding contradicts previous evidence from a different longitudinal birth cohort study, which indicated externalising symptoms as an important factor in the prediction of mid-life socio-economic outcomes, while controlling for internalising difficulties (Colman et al., Reference Colman, Murray, Abbott, Maughan, Kuh, Croudace and Jones2009). However, the former study was based on data from the 1946 British birth cohort, where symptoms were reported by teachers and externalising and internalising have weak associations, whereas the findings from this study are based on parent report of symptoms, where internalising and externalising symptoms were highly correlated.
It is important to understand the reasons for the observed cohort differences in the associations between earlier mental health and later life outcomes. As mental health difficulties become more common in adolescence, it might be expected that their impacts are weakened due to the increased normality of any experienced difficulty; however, we do not find that this is the case. Possible explanations for observed cohort differences are described. First, changes in socio-economic inequalities in mental health, such that those with higher symptoms are more likely to be from socio-economically disadvantaged backgrounds and the greater likelihood of co-occurring adversities might be responsible for poorer later-life outcomes (Collishaw, Furzer, Thapar, & Sellers, Reference Collishaw, Furzer, Thapar and Sellers2019). However, in this study we controlled for socio-economic circumstances and the associations remain suggesting that the socio-economic changes are unlikely to be the sole explanation for the observed cohort differences. Second, increased co-occurrence of poor mental health with other health impacting behaviours such as substance use (Gage & Patalay, Reference Gage and Patalay2021; Jokela, García-Velázquez, Gluschkoff, Airaksinen, & Rosenström, Reference Jokela, García-Velázquez, Gluschkoff, Airaksinen and Rosenström2020). As smoking and alcohol use have become less common in the population, they have decreased at slower rates among those with poor mental health (Gage & Patalay, Reference Gage and Patalay2021; Jokela et al., Reference Jokela, García-Velázquez, Gluschkoff, Airaksinen and Rosenström2020), as a result these are more likely to cluster in those with poor mental health with potential consequences for later health outcomes. Third, the economy has been changing to a more hourglass shape (more people with lower skilled and professional jobs with middle-ranked jobs shrinking) with a larger focus on the knowledge-based jobs and skills (Holmes & Mayhew, Reference Holmes and Mayhew2012). In these changing contexts the impacts on those with poorer earlier life mental health might become greater due to an amplification of known negative impacts on education and other life chances (Goodman et al., Reference Goodman, Joyce and Smith2011), here are likely to also be other possible explanations for cohort differences in the associations between early life mental health and later life outcomes and now that these differences have been described in this paper, future research to understand and explain these will be beneficial. In addition, it is possible that poorer social and economic outcomes in mid-life are mediated by mental health in adulthood and that there are bi-directional associations between the health and socio-economic factors examined in this paper; whether these bi-directional cycles are stronger in the more recent cohorts would be important to understand.
Strengths and limitations
Successive national population-representative birth cohort studies with comparable measures of common mental health difficulties provide a unique opportunity to make robust comparisons across cohorts using aggregated analytical techniques. Previous cross-cohort research is limited by differences in how outcomes and exposures are assessed (Sellers et al., Reference Sellers, Warne, Pickles, Maughan, Thapar and Collishaw2019), resulting in uncertainty of whether observed cohort effects are method artefacts. By using completely harmonised exposure, outcome and control variables we can be confident that the cohort effects we observe are robust, especially since the mental health measures showed evidence of measurement invariance across cohorts. Another notable strength of this study was the range of outcomes across health and socio-economic domains. One limitation of the data was that rates of selective attrition across cohorts were not identical. To address the issue of missing data that is unavoidable in long running birth cohorts, multiple imputation was applied with a detailed set of early life auxiliary predictors to minimise the risk of observed effects being due to potential differences in those retained in the cohorts (Mostafa et al., Reference Mostafa, Narayanan, Pongiglione, Dodgeon, Goodman, Silverwood and Ploubidis2021).
Implications
Recent research highlights growing levels of adolescent internalising symptoms in more recently born cohorts (Patalay & Gage, Reference Patalay and Gage2019). This is also observed in the cohorts compared in our study, with those born in 1970 reporting greater levels of mental health difficulties in adolescence and midlife (Ploubidis et al., Reference Ploubidis, Sullivan, Brown and Goodman2017). One often suggested explanation for observed increases in adolescent mental health problems across cohorts is that it might be driven by differences in how these measures are completed due to less stigma and more awareness around mental health (Collishaw, Reference Collishaw2015). However, we establish that there is measurement invariance for the Rutter mental health scale at age 16 and others have established measurement invariance for the Malaise Inventory at age 42 across these two cohorts (Ploubidis et al., Reference Ploubidis, Sullivan, Brown and Goodman2017), implying that potential sources of bias such as age effects, survey design, period effects, or cohort specific effects do not influence the way participants in the two cohorts respond to the symptoms described. Moreover, our results indicate that consequences of poor mental health in adolescents are consistently observed between cohorts, and in some cases are more severe in the youngest cohort studied here (e.g. lower likelihood of living with a partner and poorer mental health in midlife). The widening of mental health based inequalities in life outcomes, further supports the need to recognise that secular increases in adolescent mental health symptoms is a public health challenge with measurable negative consequences through the life-course (Patalay & Gage, Reference Patalay and Gage2019; Sellers et al., Reference Sellers, Warne, Pickles, Maughan, Thapar and Collishaw2019).
In summary, as evidence from more recent generations indicate that common mental health difficulties are increasing further (Patalay & Gage, Reference Patalay and Gage2019), our findings indicate that negative consequences of these difficulties might persist or even increase in younger cohorts, with implications not only for social and economic outcomes but also potentially for morbidity and stalling life expectancies (Archer, Kuh, Hotopf, Stafford, & Richards, Reference Archer, Kuh, Hotopf, Stafford and Richards2018; Ploubidis et al., Reference Ploubidis, Batty, Patalay, Bann and Goodman2021).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721002506.
Data
The datasets used in this research are available for use to all researchers, free of charge, from the UK data service (https://ukdataservice.ac.uk/).
Acknowledgements
We are grateful for the co-operation and participation of the individuals who voluntarily participate in the 1958 and 1970 birth cohort studies. We thank the Economic and Social Research Council for funding these cohorts through the Centre for Longitudinal Studies (CLS) at the UCL Institute of Education, London. We further thank the Economic and Social Research Council for funding the Cross Cohort Research Programme (CCRP) (grant number: ES/M008584/1).We also thank the Medical Research Council (MRC) (grant numbers: MC_UU_12019/1 and MC_UU_12019//3) for funding Marcus Richards. Dr Praveetha Patalay is supported by a Wellcome Trust Institutional Strategic Support Fund (ISSF3/ H17RCO/NG1). We would also like to thank a large number of stakeholders from academic, policymakers and funder communities and colleagues at CLS involved in data collection and management. The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of this report. We also thank Prof Alissa Goodman (CLS) for her advice on the economic outcome measures used in this study.
Author contributions
PP conceptualised the study with input from all authors. EJT led on data preparation and analysis. EJT and PP drafted the manuscript and all authors contributed to drafting. All authors approved the final version for submission.
Financial support
This study was supported by UK Economic and Social Research Council.
Conflict of interest
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work, no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.







