


Most countries recommend daily cow milk consumption for children to support growth and development(1–Reference Binns, Scott and Forbes4). These recommendations differ considerably on what age cow milk can first be introduced into the child’s diet. The American Academy of Pediatrics recommends that cow milk not be started until 1 year of age, which is consistent with recommendations from the United Kingdom and Australia(2,Reference Binns, Scott and Forbes4) . However, according to recommendations from Canada and Denmark, cow milk may be introduced as early as 9 months of age(1,5) . Childhood growth may be sensitive to the age that cow milk is first introduced into the diet. Cow milk consumption has been associated with small increases in children’s height, which suggests that earlier introduction of cow milk may result in greater height(Reference de Beer6–Reference Wiley8). However, excessive cow milk intake (≥3 cups per day) has been associated with early rapid weight gain, suggesting that delaying the introduction of cow milk may protect against child obesity(Reference DeBoer, Agard and Scharf7,Reference Berkey, Rockett and Willett9) .
Since the age that parents introduce cow milk into their child’s diet is modifiable, understanding how timing of cow milk introduction influences growth in later childhood may provide an intervention target to support linear growth, while minimising the risk of child obesity. We hypothesised that younger age of cow milk introduction would be associated with greater childhood height, while older age of cow milk introduction would be associated with lower childhood adiposity. The primary objective of the study was to evaluate the association between the age of cow milk introduction and height at 3–5 years of age among healthy Canadian children. Secondary objectives were to evaluate the association between the age of cow milk introduction and volume of cow milk consumed per day and adiposity at age 3–5 years.
Methods
Study design and participants
A secondary analysis of a prospective cohort study was conducted through The Applied Research Group for Kids (TARGet Kids!) practice-based research network (www.targetkids.ca)(Reference Carsley, Borkhoff and Maguire10). TARGet Kids! is a collaboration between child health researchers in the Faculty of Medicine at the University of Toronto and paediatric and family medicine practices in Toronto, Canada. Between 2008 and 2016, healthy children ≤2 years of age were recruited while attending a routine well-child visit at one of the participating TARGet Kids! clinics and followed until 3–5 years of age. Children were excluded from the study if they had a known health condition which might affect feeding or growth (e.g. cerebral palsy), chronic illness with the exception of asthma, severe developmental delay, born very preterm (before 32 weeks) and if the age of cow milk introduction was not reported or if the child did not consume cow milk.
Exposure and outcomes
Data were collected at the time of the clinic visit using a parent-completed standardised questionnaire adapted from the Canadian Community Health Survey(11). The primary exposure variable was the age of cow milk introduction. To maximise recall, this was measured at the first visit following introduction of cow milk (baseline visit) using the following question: ‘At what age did you introduce cow milk?’ Cow milk was defined as fresh, fluid commercial cow milk (any fat content) fortified with vitamins A and D. Since the age of cow milk introduction was the primary exposure, and this is infinite for children who were never introduced to cow milk, it was decided a priori to exclude them from the final analysis.
The primary outcome was height-for-age z-score. Secondary outcomes were volume of cow milk consumed per day and BMI z-score. Physical measurements were obtained by trained research assistants at each clinic. Height was measured without shoes using a calibrated stadiometer for children over 2 years and a length board for children under 2 years (SECA, Hamburg, Germany). Weight was measured using a precision digital scale (SECA). BMI was calculated as body weight (kg) divided by height (m2)(Reference Flegal and Ogden12). Height-for-age and BMI z-scores were calculated using the 2006 WHO child growth standards, which are believed to represent optimal growth in children(13,14) . All outcomes were measured at the last visit prior to 5 years of age (follow-up visit). Since height-for-age and BMI z-scores are age-standardised, minimal differences in child age at the follow-up visit were accounted for. Volume of cow milk consumed per day was obtained from the question: ‘How many 250 ml cups of cow milk does your child drink in a typical day?’
Other variables
Potential confounders known or suspected to influence the association between the age of cow milk introduction and childhood growth were generated a priori from a review of the literature. These included child age, sex, birth weight, self-reported household income, maternal ethnicity, maternal BMI or maternal height, BMI and length-for-age z-score prior to the introduction of cow milk, as well as sugar-sweetened beverage consumption and duration of breastfeeding measured at follow-up. Physical measurements prior to the introduction of cow milk were collected from a visit before cow milk was provided to the child. If more than one visit was available, the visit closest to when cow milk was introduced was chosen. Sugar-sweetened beverage consumption was defined as the daily number of 250 ml cups of 100 % juice, sweetened drinks and soda or pop. Breastfeeding duration was measured because children may have continued to receive breastmilk after being introduced to cow milk, which may have influenced growth either directly or indirectly by displacing cow milk in the diet. Total breastfeeding duration was determined from the following question: ‘For how long was your child breastfed?’ Children who had never been breastfed were classified as having a breastfeeding duration of 0 months and those currently breastfeeding were classified as having a breastfeeding duration equal to the child’s current age. Maternal ethnicity was categorised as European, Asian, African, Hispanic, mixed or other.
Statistical analysis
Descriptive characteristics including means ± sd for continuous variables and frequencies and percentages for categorical variables were used to describe the study population. For the primary analysis, univariate linear regression was used to test the unadjusted association between the age of cow milk introduction and height-for-age z-score. A multiple linear regression model was then developed to adjust for pre-specified covariates (see above) including maternal height. All potential confounders remained in the adjusted model regardless of statistical significance(Reference Harrell15). For the secondary analysis, a similar model was used to examine the unadjusted and adjusted association between the age of cow milk introduction and volume of cow milk consumed per day and BMI z-score. All covariates were the same as in the primary analysis adjusted model, except maternal BMI was included instead of maternal height.
Missing data for the outcomes and covariates were <10 %. All data were assumed to be missing at random. To reduce bias introduced from missing data, multiple imputation was performed to impute missing data for all covariate and outcome measures(Reference Harrell15). Five data sets were imputed, and the results were combined to obtain pooled estimates and standard errors(Reference Li, Stuart and Allison16,Reference Little and Rubin17) . All models were assessed for nonlinearity using linear splines(Reference Cleophas and Zwinderman18). A P-value of <0·05 was considered statistically significant, and all statistical analyses were carried out using R version 3.5.1 (www.R-project.org).
Results
A total of 3409 children met the inclusion criteria. By the follow-up visit, 445 children were younger than 3 years of age or older than 5 years of age, 184 children had not been introduced to cow milk, the age of cow milk introduction was not reported for 427 children and 372 children did not have a follow-up visit, leaving 1981 children available for the analysis (Fig. 1). Reasons for not consuming cow milk included an intolerance or allergy to cow milk (n 19), child disliked the taste of cow milk (n 1) or consumption of non-diary alternatives such as almond or soy beverages (n 83).

Fig. 1 Flow chart of participant selection
Baseline characteristics of the participants are shown in Table 1. The mean (±sd) age of children at baseline was 16·9 (±4·2) months and 46·9 (±7·5) months at follow-up, with a mean follow-up duration of 2·5 years. About half (53·8 %) of the participants were male. The average age of cow milk introduction was 11·7 (±2·1) months (min 4 months; max 30 months). Most children (99·4 %) had been introduced to cow milk by 2 years of age. Cow milk was introduced to 72 (3·6 %) children before 9 months, 562 (28·4 %) between 9 and 11·9 months, 1128 (56·9 %) between 12 and 12·9 months, 171 (8·6 %) between 13 and 17·9 months and 48 (2·4 %) at 18 months or later (Fig. 2). At follow-up, the mean height-for-age z-score was 0·04 (±0·96), children consumed an average of 1·7 (±1·0) cups of cow milk per day and the mean BMI z-score was 0·26 (±1·05).
Table 1 Baseline characteristics of children

* Table was stratified into cow milk introduction before v. at/after 12 months of age as per the current American Academy of Pediatrics Recommendation.

Fig. 2 Age of cow milk introduction distribution
In primary univariate and multivariate analyses, there was an association between younger age of cow milk introduction and greater childhood height. After adjusting for potential confounders, each month earlier that cow milk was introduced was associated with a 0·03 higher height-for-age z-score unit (95 % CI –0·05, –0·02) or 0·1 cm greater height (95 % CI –0·15, –0·12 cm) (Table 2). The height difference between a child aged 4 years who was introduced to cow milk at 9 months compared with 12 months was 0·1 height-for-age z-score units (95 % CI –0·15, –0·05) or 0·4 cm (95 CI –0·45, –0·36 cm) and compared with 18 months was 0·3 height-for-age z-score units (95 % CI –0·44, –0·14) or 1·2 cm (95 % CI –1·4, –1·1 cm). Exploration for nonlinearity revealed that the age of cow milk introduction was associated with childhood height after 9 months of age (P < 0·05) (Fig. 3).
Table 2 Association between the age of cow milk introduction and height, volume of cow milk consumed per day and adiposity adjusted for prespecified covariates (n 1981)
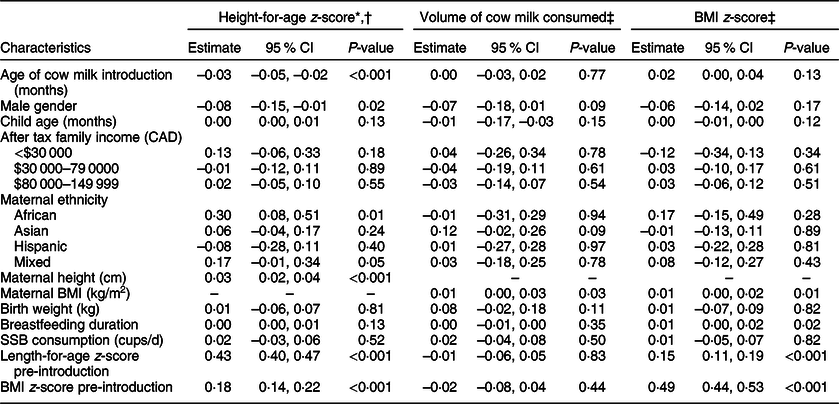
* Adjusted for age, sex, birth weight, breastfeeding duration, maternal ethnicity, household income, maternal height, sugar-sweetened beverage (SSB) consumption, BMI and length-for-age z-score prior to the introduction of cow milk.
† For a child aged 4 years, a height-for-age z-score of 0·3 is equivalent to approximately 0·1 cm.
‡ Adjusted for age, sex, birth weight, breastfeeding duration, maternal ethnicity, household income, maternal BMI, SSB consumption, BMI and length-for-age z-score prior to the introduction of cow milk.
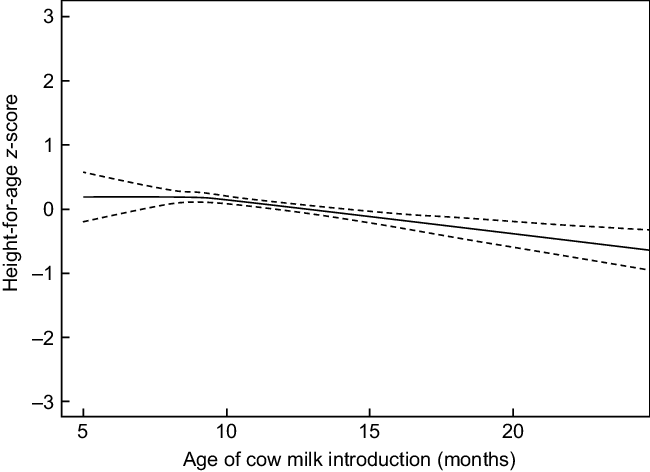
Fig. 3 Nonlinear relationship between the age of cow milk introduction and childhood height
In the univariate secondary analysis, there was no association between the age of cow milk introduction and the volume of cow milk consumed per day at follow-up (–0·005 z-score units; 95 % CI –0·03, 0·02; P = 0·64) or BMI z-score (0·01 z-score units; 95 % CI –0·01, 0·03; P = 0·48). These associations remained non-significant after adjusting for potential confounders (Table 2). Nonlinearity was not observed for the relationship between the age of cow milk introduction and child adiposity (P = 0·65).
Discussion
In this prospective cohort study of 1981 healthy children followed for an average of 2·5 years, children who started to consume cow milk at a younger age appeared to be taller by 3–5 years of age. For the average child, each month earlier that cow milk was introduced was associated with a 0·1 cm greater height. The height difference between a child aged 4 years introduced to cow milk at 9 v. 12 months was 0·4 cm and a child introduced at 9 v. 18 months was 1·2 cm. At 4 years of age, a height difference of 1·2 cm is about one-third of the distance between major percentile lines on the WHO child growth charts(13). The association with height was found only after 9 months suggesting little benefit on height for introducing cow milk prior to 9 months of age, which supports current recommendations from Canada and Denmark to delay introduction of cow milk until at least 9 months of age(1,5) . There was no association between the timing of cow milk introduction and volume cow milk consumed per day or adiposity at 3–5 years of age, suggesting that later introduction of cow milk is unlikely to protect against childhood obesity. Taken together, these findings suggest that introducing cow milk between 9 and 12 months is appropriate for supporting children’s linear growth, without adversely affecting child adiposity.
Previous research has consistently shown that children who consume cow milk attain higher height(Reference de Beer6,Reference DeBoer, Agard and Scharf7,Reference Hoppe, Udam and Lauritzen19,Reference Wiley20) . Data from the 1999 to 2002 NHANES survey found that cow milk consumption was associated with greater height in preschool children(Reference Wiley20). Also, a large prospective cohort study of American children found that higher cow milk intake was associated with greater height at 4–5 years of age. Children who consumed ≥4 v. <1 milk serving daily were 1 cm taller, which is similar to the height difference observed in the current study between children who started to consume cow milk at 9 v. 18 months of age (1·2 cm)(Reference DeBoer, Agard and Scharf7). Although childhood cow milk consumption has been previously associated with gains in height, few studies have examined how the timing of cow milk consumption may influence child growth. Our study adds to the literature by suggesting that children who start to consume cow milk earlier in life may attain greater height.
The biological mechanism by which cow milk promotes linear growth is unknown. Since cow milk is the main dietary source of Ca and vitamin D in children’s diets, nutrients essential for optimal growth, researchers have speculated that the nutrients present in cow milk may mediate the relationship between cow milk consumption and height(Reference Wiley20,Reference Black, Williams and Jones21) . In the 1999–2002 NHANES study, adjustment for Ca intake appeared to attenuate the magnitude of the association between cow milk intake and height, suggesting that Ca may play some role(Reference Wiley20). While meeting Ca and vitamin D requirements without cow milk is possible, it may be challenging and require careful planning particularly during the first few years of age as Ca-rich foods are not typically part of a toddler’s diet(1). Earlier consumption of cow milk may increase Ca and vitamin D intake during a time of rapid growth and increased nutritional needs, which may explain the observed association with height.
Other researchers have hypothesised that the energy and protein in cow milk may contribute to height in children(Reference Hoppe, Molgaard and Michaelsen22). However, Wiley(Reference Wiley20) found that the association between cow milk and height remained significant even after controlling for energy and protein intake, suggesting that there may be a component unique to cow milk that contributes to height such as insulin-like growth factor-1 (IGF-1) naturally present in cow milk. Studies have shown that children who drank more cow milk had higher circulating levels of IGF-1, and higher IGF-1 levels during childhood have been proposed to contribute to gains in height(Reference Hoppe, Molgaard and Michaelsen22). A longer duration of exposure to IGF-1 from earlier cow milk introduction may also explain the observed association with childhood height. The exact age at which IGF-1 exerts an influence on linear growth is not known; however, it has been proposed to begin sometime around 9 months of age(Reference Karlberg23). This is consistent with our findings where the association between the timing of cow milk introduction and height was apparent only after 9 months of age. However, it is possible that the present study lacked statistical power to detect a relationship with height prior to 9 months of age since only seventy-two children were introduced to cow milk before 9 months. Studies with a larger sample size are needed to confirm this finding.
There is some evidence that consuming too much cow milk (≥3 cups per day) may contribute excess energy to the diet and lead to unhealthy weight gain(Reference DeBoer, Agard and Scharf7,Reference Berkey, Rockett and Willett9) . In the current study, children introduced to cow milk at a younger age consumed a similar amount of cow milk and had similar adiposity at age 3–5 years. One explanation for these findings may be that children self-regulate energy intake following cow milk consumption, which is believed to promote satiety. Although there is little evidence for this in 3–5-year-old children, in a randomised trial of 10–12-year-old boys consumption of cow milk with breakfast, compared to juice, increased satiety and decreased energy intake at the following meal(Reference Mehrabani, Safavi and Mehrabani24). In another prospective cohort study of healthy weight preschool children, cow milk intake at age 2 years was not associated with BMI at age 3 years(Reference Huh, Rifas-Shiman and Rich-Edwards25), which is consistent with our findings.
Strengths of the study include the prospective design, which provided a means of assessing temporal relationships. Because the age of cow milk introduction was collected before the outcome measurement, child growth at follow-up was unlikely to have affected timing of cow milk introduction, minimising the possibility of reverse causality. Other strengths included a relatively large sample size of healthy, multicultural, preschool-aged Canadian children and detailed questionnaire data which allowed for the adjustment of numerous clinically relevant covariates. Lastly, although the degree of missing data was low, multiple imputation was performed to minimise the risk of bias introduced from missing data.
The study had several limitations. Causality cannot be inferred due to the observational nature of the study. The primary exposure measurement relied on parental report for the age of cow milk introduction, which may be subject to recall bias. Although, exposure data were collected at the first visit following introduction of cow milk (5 months after cow milk was introduced, on average) minimising the duration of recall. Another potential source of bias is that children’s height may have, in some way, affected the timing of cow milk introduction. However, physical measurements prior to the introduction of cow milk were included in the adjusted models to account for growth differences prior to cow milk introduction. Although adjustment included many potential confounders, residual confounding by unmeasured or unknown factors was possible. For example, because detailed dietary information was unavailable, we could not account for dietary factors such as energy and protein intake, which may have contributed to differences in height. Although sugar-sweetened beverage consumption was adjusted for, other data would have been helpful in evaluating whether total energy, protein or Ca intake was higher in children who started to consume cow milk at a younger age. Also, BMI cannot differentiate between body fat and muscle in children, and therefore, BMI z-score was used as a proxy for child adiposity and is a potential source of bias. However, BMI z-score is a widely used measure of adiposity in children and correlates well with direct measures of body fat(Reference Mei, Grummer-Strawn and Pietrobelli26). While the study population was ethnically diverse, it may not be representative of urban children in other settings. Finally, it is unclear whether childhood height is associated with final attained height in adulthood or whether the advantages of being taller outweigh potential disadvantages of earlier cow milk consumption not examined in the current study (e.g. Fe status)(Reference Green, Cairns and Casabonne27).
In this prospective cohort of healthy children, younger age of cow milk introduction was associated with greater height among 3–5-year-old children living in Toronto, Canada. Earlier cow milk introduction was neither associated with greater cow milk consumption nor was it associated with a higher BMI. Taken together, these findings suggest that one advantage of introducing cow milk earlier in life is a potential gain in height and that later introduction of cow milk is unlikely to decrease the risk of child obesity. Future studies that follow children throughout childhood and into adolescence are needed to understand how the timing of cow milk introduction may influence long-term growth and to understand the biological mechanisms underlying the relationships observed in the current study.
Acknowledgements
Acknowledgements: The authors thank all of the participating families for their time and involvement in TARGet Kids! and are grateful to all collaborators and practitioners who are currently involved in the TARGet Kids! practice-based research network. Financial support: No external funding received. Conflict of interest: Dr. Maguire received an unrestricted research grant for a completed investigator-initiated study from the Dairy Farmers of Canada (2011–2012), and Ddrops provided non-financial support (vitamin D supplements) for an investigator initiated study on vitamin D and respiratory tract infections (2011–2015). Dr. Birken received a research grant from the Centre for Addiction and Mental Health Foundation (CAMH 2017–2020). Authorship: Dr. Maguire and Ms. Soczynska: conceptualised and designed the study, drafted the manuscript and had primary responsibility for final content; Ms. Soczynska: performed statistical analysis and analysed data. All authors critically revised and reviewed the manuscript for important intellectual content and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the St. Michael’s Hospital and Sick Kids ethics committee. Written informed consent was obtained from all parents of subjects.





