


INTRODUCTION
Dengue is a leading cause of morbidity and mortality in tropical and subtropical regions and demands progressive efforts and investments by the countries in which it is endemic [Reference Guzman1]. In the Americas, about five million cases were reported between 2000 and 2007, and the four dengue virus (DENV) serotypes (DENV-1, -2, -3, -4) were reported to be in circulation [Reference San Martin2]. Brazil accounts for more than 50% of dengue cases in the American continent and about 60% of registered cases in the world [Reference Teixeira3].
Currently, there is a global consensus on the urgent need for the development of a safe dengue vaccine with the ability to stimulate a strong protective response of neutralizing antibodies against all four serotypes [Reference Swaminathan, Batra and Khanna4].
Dengue infection induces a long-lasting protective immunity to homologous serotypes and a short period of immune protection to heterologous serotypes [Reference Kyle and Harris5]. The co-circulation of different DENV serotypes is a risk for the emergence of severe cases because it increases the chance of secondary infections and also the emergence of more virulent genotypes [Reference Rico-Hesse6, Reference Halstead7].
The immune resistance and susceptibility of the population to different DENV serotypes is one of the factors that modulate the intensity of viral circulation and the occurrence of epidemics in the population [Reference Kuno8]. Studies investigating anti-dengue serotype-specific antibody status at the population level provide information about the dynamics of DENV serotype infection in a specific region and are useful for estimating the optimal age for implementation of future dengue vaccines [Reference Ferguson, Donnelly and Anderson9].
The plaque reduction neutralization test (PRNT) is considered to be the gold standard for detecting antibodies specific for different serotypes of DENV and has been widely used in studies evaluating the immunogenicity of dengue vaccines under development [Reference Simasathien10, Reference Capeding11] and in other studies [Reference Reiskind12–Reference Sanchez-Burgos14]. However, determining serotype-specific antibodies in population studies using PRNT has been difficult because it requires skilled technical staff and long periods of time to perform the tests [Reference Roehrig, Hombach and Barrett15]. Moreover, the cross-reactivity between different flaviviruses and DENV serotypes may result in difficult interpretations of the results in regions where different flaviviruses are circulating [Reference Roehrig, Hombach and Barrett15].
The northeastern region of Brazil, which is the country's second most populous region, contained about 20% of reported dengue cases in January–April 2011. Additionally, 34·2% of severe cases were reported in the state of Pernambuco [16]. Between 2005 and 2006, a population-based serological survey conducted in Recife, the capital of Pernambuco state, showed an overall anti-dengue IgG positivity of about 90%, indicating the intense viral transmission of dengue [Reference Braga17]. The estimated time-constant force of dengue infection in a subset of this study population (aged 5–20 years) yielded 5·2% cases of infection per year. However, this previous simulation lacked data on serotype-specific immune status by PRNT, which is necessary to accurately estimate the dynamics of viral circulation [Reference Ferguson, Donnelly and Anderson9]. In this paper, we report the dengue serotype-specific neutralizing antibodies results (PRNT50) of the participants of this survey. The potential risk factors for infection by one, two or three serotypes were assessed. We also estimated the distribution of susceptible individuals by the different DENV serotypes according to age using a simple catalytic model.
METHODS
Characteristics of the area and study population
The city of Recife is an area of 219 km2 divided into 94 neighbourhood districts with a population of 1 537 704 inhabitants in 2010 [18]. In Recife, which is the capital of the state and the major urban centre, the first reports of dengue fever occurred in 1987 with the circulation of DENV-1, which caused the first epidemic. In 1995, the introduction of DENV-2 led to a second epidemic, in which the first cases of dengue haemorrhagic fever (DHF) were reported [Reference Cordeiro19]. In 2002, DENV-3 was introduced and caused the largest and most severe epidemic in the city, with over 35 000 reported cases, 208 DHF cases and 14 deaths [Reference Montenegro20]. In 2005, during the period in which the population-based dengue survey was conducted, a total of 4796 dengue cases were reported by the surveillance system and DENV-3 was the only serotype isolated in the city (Health Department of Recife, unpublished data).
A major population-based survey (n=2819) was conducted in three selected areas, based on their distinct socioeconomic and physiographic characteristics, to represent a deprived, an intermediate and a high socioeconomic setting in the city of Recife in northeastern Brazil between 2005 and 2006. Concisely, dengue serostatus and individual- and household-level risk factors for infection were obtained from individuals aged between 5 and 64 years. Anti-dengue IgG antibodies were measured using commercial ELISA (Dengue-IgG ELISA, PanBio Ltd, Australia). The dengue seroprevalence was 91·1%, 87·4%, 74·3%, respectively, in the deprived, intermediate and high socioeconomic areas, respectively. Details on the sampling procedure, selection of the participants, data collection, and measurement of seroprevalence and risk factors have been described previously [Reference Braga17].
In the current study, we chose the intermediate socioeconomic setting (the neighbourhood of Engenho do Meio) to explore the serotype-specific immunity of the population. This setting was selected due its intermediate levels of endemicity (87·4%) and greater heterogeneity in its socioeconomic characteristics compared to the others [Reference Braga17]. Briefly, of 923 individuals investigated, 807 were dengue-IgG positive and a random sample was selected for PRNT evaluation.
Sample size calculation
Of 807 positive individuals, 323 stored samples were randomly selected to undergo PRNT. This sample size is large enough to estimate proportions of about 10% for the different serotypes in a single sample, assuming a maximum random error of about 2·5% [Reference Scheaffer, Mendenhall, Ott and Scheaffer21].
Laboratory procedures
The anti-dengue serotype-specific antibodies were determined by PRNT50, following a modified protocol by Morens et al. [Reference Morens22], and according to the World Health Organization guidelines [Reference Roehrig, Hombach and Barrett15]. The tests were performed at the Laboratory of Virology and Experimental Therapy (LaViTE), Centro de Pesquisas Aggeu Magalhães/FIOCRUZ in Recife, Pernambuco.
Dengue and yellow fever virus preparation
The virus strains DENV-1 (PE/97-42735), DENV-2 (PE/95-3808) and DENV-3 (PE/02-95016), which were isolated in Pernambuco state and donated by the Public Health Laboratory of Pernambuco (LACEN-PE), were used to prepare viral stock by cell inoculation. Since DENV-4 was not circulating in the region at the time of the survey and therefore no virus strain was isolated in the entire period from the start of dengue circulation in 1987 to 2006 [Reference Cordeiro19] this virus strain was not available for testing. The cross-reactivity was assessed using Yellow Fever virus human vaccine (YFV-17DD) obtained from the Oswaldo Cruz Foundation (Rio de Janeiro, Brazil). The vaccine was reconstituted with the distilled water provided, kept in an ice bath and used for cell inoculation. Vero (African green monkey kidney) cells were grown in minimal essential medium (MEM; Gibco BRL, USA) supplemented with 10% fetal bovine serum (FBS; Gibco BRL), and 1% penicillin/streptomycin solution (Gibco BRL) and kept at 37 °C in 5% CO2. Sub-confluent Vero cells grown in T175 flasks were infected with each DENV serotype at a multiplicity of infection of 0·1 for 5–6 days in MEM with 2% FBS and incubated at 37 °C in 5% CO2. After freeze-thawing, the cell suspensions were centrifuged at 931 g for 10 min at 4 °C. Supernatants containing each one of the DENV particles were collected and stored in vials at −80 °C.
PRNT
Briefly, assays were performed with Vero cells that had been seeded at a density of 300 000 cells/ml and grown in MEM with 10% FBS and 1% penicillin/streptomycin solution in 24-well plates (0·5 ml/well) for 24 h before the assay. Serum samples were inactivated for 30 min at 56 °C before diluting in MEM. The assay for screening DENV-specific neutralizing antibodies was performed after dilution of serum (1/20 and 1/80) into 96-well microtitre plates and the addition of 30 plaque-forming units (p.f.u.) of the challenge virus (DENV-1, -2, -3) to the wells. After incubation at 37 °C in a 5% CO2 atmosphere for 1 h, the medium of the 24-well microplates was discarded, and 50 μl of each dilution of the mixture serum/virus was inoculated in duplicate. The plates were then incubated at 37 °C in 5% CO2 for 1 h to allow virus adsorption. After incubation, the cells were covered with 500 μl of semi-solid medium [MEM 10×, 10% FBS, 10% carboxymethylcellulose (3%), 1% penicillin/streptomycin]. After incubation for 6–7 days at 37 °C in 5% CO2, the semi-solid medium was discarded and the cell monolayer was fixed with formalin solution (3·5 m) for 1 h and stained with Crystal Violet (0·5 ml/well). The plates were washed with water and subsequently counted after drying. The PRNT positivity was defined based on a ⩾50% reduction in plaque counts (PRNT50) at the lowest serum dilution used (1:20).
To ensure accuracy and to avoid intra- and inter-test variations, the same technician performed all the procedures. The entire sample was tested independently by investigators who were blinded with regard to the previous serological status of the individuals and other information such as age and sex. Positive and negative controls were included in each assay. Wells that contained uninfected cells were also used as controls. The following criteria were used to validate the test results: integrity of the monolayer of uninfected cells, the presence of little or no reduction in plate count of negative sera and appropriate plate counting of the positive control.
To assess cross-reactivity, all samples that were simultaneously positive for DENV-1, -2 and -3 in individuals aged <15 years (n=12) were tested for yellow fever virus (YFV-17DD) neutralizing antibodies. The neutralizing antibody titres for dengue serotypes were also determined in these samples at serum dilutions 1/20 to 1/1280, following the standard protocol of PRNT50.
Data analysis
The frequency distribution of the main characteristics of the study population was described. The neutralizing antibody titres (PRNT50) were determined by probit regression and transformed to the logarithmic scale (log10). The comparison of the means of the antibody titres of the three serotypes was performed using analysis of variance (ANOVA).
The analysis of the association between the numbers of DENV serotypes (one, two and three simultaneous serotype infections) and mean age was performed using ANOVA, whereas their association with gender and report of healthcare seeking behaviour during the acute disease was tested through χ2 test for trend. To produce the inferences of the serotype-specific susceptibility by age group in the general population, we first took the serotype-specific susceptibility and its 95% confidence interval (CI) in the positive subsample. Then, we incorporated the variability of the serotype-specific susceptibility in the overall susceptibility (not specific) measured in the serosurvey.
The force of infection (FOI) corresponds to the incidence and is used to explore the intensity of transmission of dengue infection in a population. Since age reflects duration of exposure, an age-stratified, strain-specific serological survey performed at one point in time can potentially provide information on the dynamics of infection [Reference Egger23, Reference Anderson and May24]. In this serosurvey, the FOI was estimated for the three serotypes (DENV-1, -2, -3) by a simple catalytic model using the age-specific distribution of the susceptible population. The assumptions of the model were absence of cross-protection among serotypes and absence of antibody-dependent enhancement response following primary infection [Reference Ferguson, Donnelly and Anderson9].
Statistical analysis was performed using Epi Info v. 6.04 (CDC, USA), GraphPad Prism v. 4.0 (GraphPad Software, USA), and SPSS v. 13.0 (SPSS Inc., USA).
Ethical considerations
Written consent to participate in the study was obtained from each person (or their guardian) after a full explanation of the study was provided. The data were treated confidentially and anonymously. The research was approved by the Ethics and Research Committee of the Centro de Pesquisas Aggeu Magalhães – FIOCRUZ (No. 8.19).
RESULTS
In total, 323 out of 324 selected dengue IgG-positive individuals had serotype-specific antibodies determined by PRNT.
Table 1 shows the main characteristics of the participants. The median age of participants was 23 years (range 5–64 years). In total, 58% were female and 55% had completed secondary school. About 60% of residents did not report previous dengue illness, suggesting a high frequency of unapparent infection. Of 125 residents who reported clinical disease, 56 (45·2%) sought medical assistance during the acute phase. Of 323 infected individuals, 174 (53·8%) had antibodies to DENV-1, 104 (32·2%) had antibodies to DENV-2 and 301 (93·2%) had antibodies to DENV-3. The frequencies of monotypic and multitypic infections were 124 (38·4%) and 199 (61·6%), respectively. Monotypic infections by DENV-3 were the most frequently found (35·6%), followed by multitypic infections by DENV-1 and DENV-3 (30·3%) and by DENV-1, -2 and -3 (17·7%). Of 109 individuals aged <15 years, 61·5% presented more than one serotype and thus had a multitypic dengue infection.
Table 1. Demographic and clinical characteristics of study subjects (n=323). Engenho do Meio, Recife, northeastern Brazil, 2005

* Previous dengue infection reported by the subject during the interview (four participants had missing information).
† Participants who reported seeking medical assistance in the acute phase of the disease (one participant was missing information).
Table 2 shows the association between the number of dengue serotype markers (one, two or three dengue serotypes) and age, sex, self-reported dengue, and healthcare-seeking behaviour during the acute disease. Individuals who were co-infected with three dengue serotypes were older compared to individuals infected by one or two serotypes (F test=4·152, P=0·016). There was no significant difference in the number of serotypes detected between men and women.
Table 2. Number of dengue serotypes according to demographic and clinical characteristics. Engenho do Meio, Recife, 2005
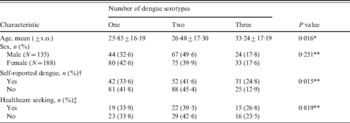
s.d., Standard deviation.
† Previous dengue infection reported by the subject during the interview.
‡ Participants who reported seeking medical assistance in the acute phase of the disease.
* ANOVA
** χ2 for trend.
There was a significant increased trend of being symptomatic according to exposure to one, two or three serotypes (χ2 for trend=5·90, d.f.=1, P=0·015). No association was found between self-reported healthcare seeking during the acute phase with the detection of one or more circulating serotypes.
Figure 1 shows the proportion of individuals susceptible to dengue infection by the different DENV serotypes according to age using a simple catalytic model. Individuals were most commonly susceptible to DENV-2, followed by DENV-1 and DENV-3. By the age of 5 years, about 70% of the children were immune to DENV-3 infection, whereas about 30% were immune to DENV-2 and about 40% were immune to DENV-1. With increasing age, fewer individuals were susceptible to all three DENV infections. Less than 10% of the population was susceptible to DENV-3 infection by the age of 60 years. The estimated FOI was 2·5% (95% CI 1·1–6·1) for DENV-3, 0·9% (95% CI 0·7–2·4) for DENV-1, and 0·4% (95% CI 0·1–0·6) for DENV-2.

Fig. 1. Estimated susceptible population for DENV-1, -2 and -3 according to age by a catalytic model. Recife, Brazil, 2005–2006.
Among children (<15 years) with simultaneous detection of DENV-1, -2 and -3, none had detectable levels of neutralizing antibodies to YFV (antibody titres <1/20). Higher titres of neutralizing antibodies were detected in individuals infected with DENV-3 (4·57±1·05) compared to DENV-1 (2·06±0·50) and DENV-2 (2·16±0·49) (P<0·001) (Fig. 2).

Fig. 2. Antibodies titres (log10) according to dengue serotypes between individuals aged <15 years who had serological markers to three dengue serotypes (P<0·001).
DISCUSSION
This study detected a high frequency of multitypic DENV infections in a population-based survey conducted in a major city in northeastern Brazil. Our study showed evidence of intense co-circulation of DENV in the area, with a predominance of DENV-3 and DENV-1 and a low frequency of DENV-2. DENV-3 had the highest time-constant incidence (2·5% per year) in the model, which was twice as high as the FOI for DENV-1. Moreover, the high proportion of children who were already immune to DENV-3 by the age of 5 years, as depicted by the catalytic curves, indicates the intense transmission of DENV-3 in early childhood. These findings are in accord with the epidemiological patterns of dengue in Brazil, where DENV-1, -2 and -3 have co-circulated since 2001, with DENV-3 predominating during the study period [Reference Cordeiro19, Reference Nogueira, de Araujo and Schatzmayr25]. Locally, the introduction of DENV-3 and its first outbreak occurred 3 years prior to the current survey, which took place in 2005; about 30 000 registered dengue cases with 14 deaths were observed during the outbreak [Reference Montenegro20].
To our knowledge this is the first study that tested a large number of DENV-infected individuals by PRNT in a region of hyperendemicity in northeastern Brazil; seroprevalence of about 90% was found at the population level [Reference Braga17]. In the same period, another survey was conducted in urban districts in the city of Belo Horizonte, in the southeast region of Brazil, which is a low endemic region. This survey found seroprevalence of 12% with serotypes varying from 0·85% (DENV-2) to 3·95% for the concomitant infection with of DENV-1, -2 and -3 [Reference Pessanha26]. Furthermore, a high proportion of individuals susceptible to the three serotypes were detected in the previous study, in contrast with the high levels of multiple serotype infections in our study in the northeast. However, the predominance of DENV-3 solely or in combination with other serotypes and a low frequency of DENV-2 was a common feature of both Brazilian surveys. It is of note that the distinct epidemiological scenarios, with a variability of co-circulation of multiple serotypes in regions in a continental country such as Brazil, are reported by the national surveillance system [Reference Siqueira27].
In the study setting, the co-positivity of DENV-1, -2 and -3 were more likely to be detected in adults. Similar results were found in a retrospective serological study that analysed the immunological status by age group in the city of Taiwan and showed an increased age-dependent rate of secondary infection from 0% (birth cohort 1990 and after) to 100% (birth cohort between 1931 and 1935) [Reference Chang28]. In South East Asia, a study of 166 volunteers found evidence that 58% of the adult population were infected with the four serotypes [Reference Wilder-Smith29]. Of note, dengue re-emerged in Brazil in the late 1980s, [Reference Siqueira27] whereas South East Asia has experienced dengue epidemics since the 18th century [Reference Gubler30].
One of the most marked findings of our study regarding the PRNT evaluation was that 11% of children and adolescents (<15 years) already had detectable antibodies against the three serotypes, showing an intense DENV co-circulation at an early age. In fact, surveillance data have noted a steady shift in dengue incidence towards younger age groups, combined with increased hospitalization, particularly in the northeast region where our study was conducted [Reference Siqueira27, Reference Cavalcanti31].
In our survey, about half of the infected individuals did not recall having the disease, suggesting a high frequency of unapparent infection in agreement with other epidemiological studies [Reference Siqueira27, Reference Endy32]. Interestingly, individuals who had serological markers for the three serotypes of the virus were more likely to report dengue disease. Under the assumption of long-term protection only for homologous serotypes [Reference Kyle and Harris5], it is likely that repeated viral exposure to the different serotypes, as detected in our study, would increase the chance of symptomatic disease [Reference Sangkawibha13, Reference Guzman33].
The catalytic model of infection for dengue, as we presented, is a simplified approach to age-distribution for the incidence of each DENV serotype individually. The study of the dynamic of dengue infection is complex because each of the four serotypes causes not only long-term protection for the homologous virus but also short-term cross-protective infection in a naive population. This model assumes a constant FOI in a susceptible population, and it does not take into account the time period of the introduction of the different serotypes, nor the heterogeneity of the population with respect to previous dengue exposure or the distribution of the vector population [Reference Kuno8].
Even with these caveats, this model using PRNT data showed regression curves with similar shapes. This pattern may reflect the cumulative acquisition of dengue infection for each serotype over time, similar to other viral infectious diseases [Reference Alencar Ximenes34]. However, the FOI of DENV-3 and DENV-1 was higher than DENV-2. Our data indicated the predominance of DENV-3 infection in the population as a whole and identified DENV-3 as probably the last circulating serotype. In fact, for young individuals with multitypic infections DENV-3 had the higher antibody titres, suggesting a more recent infection than the other viruses in the tested subsample. These findings are in accord with the large epidemics of DENV-3 in 2001 and the less frequent reporting of DENV-2 isolated in registered cases according to the official surveillance system. In our study, the attack rate for the three serotypes ranged from 1·9 to 9·1, which is the sum of the lower and higher 95% CI values. These incidence values were in line with the estimated variation found in a previous simulation model that also used the seroprevalence data from this survey conducted in the city of Recife [Reference Rodriguez-Barraquer35]. Several differences can be noted between both analyses. The current paper presents dengue serotype results to calculate distinct FOI, while the former publication applied mathematical modelling and assumed similar attack rates for the distinct serotypes to describe the evolution of the Brazilian dengue patterns [Reference Rodriguez-Barraquer35].
One of the limitations of the present study is that the analysis of the serotype-specific prevalence was performed in a subset of individuals since the PRNT is a very laborious technique and the study population may not be representative of the entire city. Although our results provide valuable data on previous immunity at population level they cannot be extrapolated for the population as whole. We also acknowledge that a comprehensive approach considering both the effect of ecological and immunological determinants would be valuable to the understanding of the dynamic of dengue transmission in the population. Nevertheless environmental factors were beyond the scope of the present study.
In summary, the current study showed evidence of intense exposure and multiple DENV-1, -2 and -3 infections at an early age. The epidemiological patterns presented here note the need for knowledge of dengue serotype infections in neonates and early childhood in representative samples of the Brazilian population. Furthermore, research efforts should be performed to study the vertical transmission of the virus and the consequences of antibody decay in infants in order to provide data for the optimal age of vaccination for the forthcoming vaccine era.
ACKNOWLEDGEMENTS
The authors acknowledge the partial support of the P. M. S. Castanha by Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco (Grant BFT-0190-4.06/10). C. M. T. Martelli and W. V. Souza received research scholarships (CNPq numbers 306489/2010-4, 305281/2010-0) and are research members from the National Institute of Science and Technology for Health Technology Assessment.
DECLARATION OF INTEREST
None.




