



Introduction
Nutritious diets play a major role in the growth and development of children and prevention of future chronic diseases, such as obesity, which affects 19% of those aged 2–19 and 40% of adults in the US, and costs the US healthcare system $147 billion dollars annually.(1) Despite nutritional efforts such as the Federal Child Nutritional programmes (e.g. National School Lunch Program, School Breakfast Program), the US still faces a childhood obesity crisis.(2) Childhood obesity elevates risk of chronic health and worsening outcomes for affected children, including cardiovascular disease, asthma, and psychological disorders, with a linkage to the persistence of obesity into adulthood.(Reference Rajjo, Mohammed and Alsawas3,Reference Davis, Martinez and Spruijt-Metz4) Obesity rates among youth have been increasing steadily over the past decade, generating an increased burden of disease and negative health outcomes for affected populations.(Reference Rajjo, Mohammed and Alsawas3) Furthermore, these complications disproportionately increase risk in racially and economically marginalised children.(Reference Davis, Martinez and Spruijt-Metz4–Reference Hughes, Power and Beck8)
Nutrition also plays a major role in the management of chronic disease with those eating a healthy diet living longer and having a lower risk of chronic health conditions.(1,Reference Khaodhiar, McCowen and Blackburn5) According to the US Departments of Health and Human Services and Agriculture, a healthy diet includes a variety of plant- and animal-based proteins, fruits, vegetables, and whole grains and contains a minimum of added sugars, sodium, trans and saturated fats, and cholesterol.(9) Since 1999, there has been an upward trend in consumption of ultra-processed foods among US youth.(Reference Wang, Martínez Steele and Du10) Contrarily, studies have shown that when foods with high nutrient density are consumed, they can help break the intergenerational cycle of malnutrition and obesity.(Reference Troesch, Biesalski and Bos11) Nutrition education and cooking skills in the younger population can provide long-term benefits later in life.(Reference Utter, Larson and Laska12) Thus, one approach to combating childhood obesity has focused on providing nutrition education to children, particularly amongst at-risk populations. The approach is founded on the idea that increasing knowledge of food and eating habits can subsequently increase dietary consumption of healthier foods and decrease consumption of their unhealthy counterparts.(Reference Hughes, Power and Beck8,Reference Cunningham-Sabo, Lohse and Smith13,Reference Marshall and Albin14)
Educational interventions including general food knowledge, gardening lessons, and interactive culinary skills sessions have proven to increase participant knowledge and awareness of healthy food choices; however, anthropometric changes have been variable.(Reference Davis, Martinez and Spruijt-Metz4,Reference Cunningham-Sabo and Lohse6,Reference Cunningham-Sabo, Lohse and Smith13,Reference Davis, Pérez and Asigbee15,Reference Poelman, Delahunty and Broch16) Yet if initiated in the early stages of life, there is evidence that nutrition education coupled with cooking skills can be used to prevent and reduce diet-related disease and overall obesity.(Reference Lavelle, Spence and Hollywood17) Inconsistency in study findings suggests multifactorial influences on eating patterns in the paediatric population. Home food availability, parental diet, familial eating habits, and length and sustainability of intervention have been identified as factors that play an important role in the diet quality of children.(Reference Santiago-Torres, Adams and Carrel7,Reference Davis, Pérez and Asigbee15) Research shows that healthy eating leads to healthier weights and better long-term health outcomes.(Reference Rajjo, Mohammed and Alsawas3) Nonetheless, the benefits of integrating food and cooking skills (e.g. food safety, preparation) into nutrition education programmes have not been widely explored in urban paediatric populations, serving as the novel focus of this study. For example, while programmes such as SNAP-Ed and EFNEP have integrated skills-based aspects like food and cooking safety, there is limited research on their specific impact on paediatric populations, particularly in terms of longitudinal outcomes. We sought to fill that gap by exploring the benefits of integrating such skills-based components into nutrition education programmes.
In Philadelphia, approximately 41% of youth aged 6–17 are overweight or obese and more than a third (37%) live in poverty.(1,Reference Howell18) Vetri Community Partnership (VCP) is a nonprofit organisation in Philadelphia that strives to educate and empower students and families to lead healthier lives.(19) Using the kitchen as the classroom, Vetri Cooking Lab (VCL) — on of several VCP community engagement initiatives — teaches students from under-resourced communities how to cook while reinforcing STEAM (science, technology, engineering, art, and math) core concepts.(20) Culinary and education experts combine hands-on cooking experiences with nutrition education to foster the next generation of educated food consumers. Each lesson includes the creation of one to three recipes that complement a nutrition lesson, such as ‘Eating a Rainbow’, the ‘Importance of Breakfast’, and ‘Food Comes from the Earth’.
Previous research shows that nutrition education and cooking skills interventions can lead to improved food knowledge and confidence, which are positively correlated with healthier dietary behaviours.(Reference Cunningham-Sabo, Lohse and Smith13,Reference Marshall and Albin14) Our study builds on these findings by examining the correlation between increased cooking confidence and knowledge with changes in dietary consumption behaviours among children. Specifically, in the current study, we aimed to determine if children enrolled in a culinary skills programme promoting healthy food choices (i.e. VCL) experienced subsequent changes in: (1) knowledge and confidence; (2) vegetable preferences; and (3) dietary consumption behaviours.
Methods
Study design, setting, and participants
To assess the effectiveness of the VCL programme, we conducted a longitudinal observational study comparing students’ food knowledge and confidence, vegetable preferences, and dietary consumption behaviours student before and after VCL participation.
Eligible participants were enrollees in VCL during the 2018–19 academic year. Each VCL consisted of 8–10 sessions held weekly during both in-school and out-of-school time. Each class was conducted once a week, and the same cohort of students attended either in-school or out-of-school sessions, but not both, allowing for flexibility in implementation while maintaining consistent delivery of the programme’s curriculum. There were a total of 60 VCLs at 30 sites throughout Philadelphia and Camden, with semesters running in the fall and spring of each school year. At each site, one class of up to 15 students from grades three and up were selected by the school liaison or after-school programme liaison with any methods of their choosing — hand-selecting, nominating, or utilising an application process.
Ethical review
Analysis of de-identified data was performed according to International Review Board (IRB) protocol approved by the Thomas Jefferson University IRB. Consent was obtained from parents/guardians of participating students through a signed consent form approved by partner schools.
Educational cooking lab programme
The programme’s curriculum offered participants a sequence of lessons aimed to allow them to taste new foods in a positive setting and develop meal planning, food preparation, and cooking safety skills.(Reference Davis, Martinez and Spruijt-Metz4) VCL provided students with hands-on cooking lessons that complemented nutrition topics and highlighted the STEAM concepts learned in school. Participants received extracurricular programming with a goal of increased understanding of healthy eating and food preparation. Teachers and school liaisons were encouraged to observe classes and often received recipe samples and recipe books. As an opt-in programme, students were enrolled by school staff or partners and able to withdraw at any time. Appendix A presents an overview of 2018–2019 VCL curriculum.
Measurement
A 46-item survey questionnaire was developed to be administered at baseline and post-intervention (see Appendix B). Additional demographic items were also collected (e.g. age, race/ethnicity, gender). Survey items were adapted from previously validated research instruments including the Healthy Eating Index (HEI), Block Kids Questionnaire, and Home Environment Survey.(Reference Hanson, Neumark-Sztainer and Eisenberg21–Reference Gattshall, Shoup and Marshall26) The survey included 10 items to capture students’ culinary knowledge (e.g. ‘I can identify foods that are made of whole grains’.); 10 items to capture students’ culinary confidence (e.g. ‘I feel confident measuring ingredients correctly’); six items for consumption behaviours (e.g. ‘How often do you eat fruits?’); and 20 items for vegetable consumption preferences (e.g. ‘How do you feel about cabbage?’). To support comparison among the 20 vegetables included in the consumptive preferences measure, half were presented during VCL sessions and half were not presented (presented: cabbage, avocado, sweet potato, radish, cauliflower, kale, chickpeas, Swiss chard, mushroom, and turnips; not presented: eggplant, peas, Brussels sprouts, bell pepper, asparagus, cucumber, green beans, celery, butternut squash, carrots).
Knowledge and confidence items were responded to on a 3-point scale: ‘0 = not at all’, ‘1 = sometimes’, or ‘2 = often’. Frequency of food consumption behaviour items were presented with the options ‘0 = never’, ‘1 = 1–2 times a week’, ‘2 = 3–5 times a week’, and ‘3 = daily or almost daily’. Consumption preferences item response included ‘0 = I don’t like it’, ‘1 = I like it’, and ‘2 = I don’t know what it is’. Confidence and knowledge items scores were totalled, creating a scale ranging 0 (low confidence/knowledge) to 20 (high confidence/knowledge). The first scale measured student confidence in meal planning and preparation. The second measured knowledge of nutrition and safety. Consumption behaviour questions were totalled for maximum score of 18. We assessed scale reliability of the included measures using Cronbach’s alpha,(Reference Tavakol and Dennick27) concluding that each exhibited high reliability scores (confidence = 0.77; knowledge = 0.73; consumption behaviours = 0.75).
Data collection
Programme instructors and volunteers administered baseline and post-intervention surveys in the first and last classes, respectively. If students were absent in the first class, the baseline assessment was administered during the first class attended by the student. If any student was absent on the last day, a post-intervention survey was not administered or collected, and their baseline survey was not included in our matched analysis. To address varied reading and comprehension skill levels, instructions for administering the surveys were provided for all VCL instructors and volunteers. In particular, instructors and volunteers were available to read survey questions orally. Assistance was provided for students who had questions about answering the surveys.
Statistical analysis
Following data collection, survey responses were compared at baseline and post-intervention to identify changes in cooking confidence, nutritional knowledge, consumption preferences (i.e. vegetable likes), and consumption behaviours. Students who skipped more than a quarter of questions in either survey were omitted from analysis. Median imputation was used to account for missing responses to individual items (percent missing: mean = 3.8; maximum = 7.6).
We used paired t-tests (alpha = 0.05) to identify pre-post changes in knowledge, confidence, consumption preferences, and consumption behaviours. Pearson’s correlation coefficients (r) and Cohen’s d, a standardised measure of effect size,(Reference Fritz, Morris and Richler28) were also generated among each of the aggregate measures. For consumption preference questions, we calculated percentages of vegetables liked, not liked, and hadn’t tried, stratified by whether or not vegetables were presented during VCL classes.
Using multivariable logistic regression, we modelled how consumption behaviours were associated whether changes in knowledge and confidence while adjusting for participants’ age, race, ethnicity, gender, and language, as well as VCL site. An indicator variable was created if students had positive changes in consumption behaviours (0 = no change, 1 = change). To account for correlation between change in knowledge and confidence, we included an interaction variable in the final regression model to explore their potentially synergistic effect.(Reference Cortina29,Reference Jaccard, Wan and Turrisi30) Student grade was not included because of collinearity with age.
Results
Sample characteristics
A total of 904 students enrolled in VCL in the 2018–19 school year. Of enrollees, 171 completed pre- and post-surveys and were eligible for our analysis (response rate = 18.9%; see Table 1). Among the 171 respondents, more than half identified as Black (51.5%) and female (60.1%). Nearly four in ten also identified as Hispanic or Latino (39.1%). Student ages ranged from 8 to 16 (mean = 10.6; SD = 1.5; median = 10) and grade levels from 4 to 11. More than half were in grades four or five, 26.9% and 31.0%, respectively.
Table 1. Sample characteristics (n = 171). Frequency and proportion are presented for characteristics of the study participants including gender, grade, race, ethnicity, and language

Confidence, knowledge, and consumption behaviours
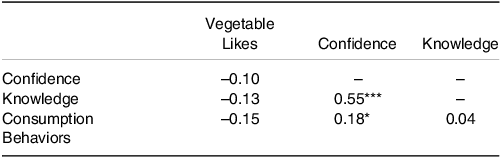
On average, students scored higher on post-survey confidence (P < 0.001; d = 0.45) and knowledge (P < 0.001; d = 0.43) scales (see Table 2). Half of students reported at least some changes in individual consumption behaviours (n = 85, 49.7%). As shown in Table 3, knowledge and confidence were positively correlated (r = 0.55; P < 0.001). Increased confidence was also positively correlated with consumption behaviour change (r = 0.18; P = 0.022). Cohen’s d scores and t-tests revealed small to medium effects on students’ food confidence and knowledge that were significant at the alpha = 0.05 level (see Table 2).
Table 2. Pre-post score and scale descriptive statistics (total n = 171). Summary of pre- and post-intervention scores for confidence, knowledge, and consumption behaviours among participants. Table columns includes mean scores, standard deviations, Cohen’s d effect sizes, and P-values for paired t-tests comparing baseline and post-intervention results. Alpha level is set at 0.05 for significance. Alpha = 0.05
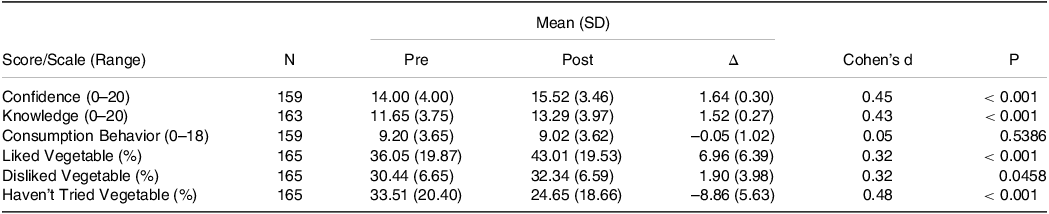
Table 3. Pearson’s correlation coefficient (r) for survey components. Correlation coefficients are presented for selected components of the survey, including confidence, knowledge, consumption behaviours, and vegetable likes. Significance levels are indicated: ***P < 0.001, *P < 0.05. Alpha = 0.05
When accounting for differences in student demographics and VCL site, we identified several predictors of changes in consumption behaviours (see Table 4). Increased knowledge was independently associated with behaviour changes (OR = 1.46; P = 0.026). Confidence was positively associated with consumption changes in both our adjusted (OR = 1.81; P < 0.001) and unadjusted models (aOR = 1.88; P = 0.013). Students who gained confidence in their ability to add vegetables to every meal had nearly three times higher odds of reporting consumption behaviour changes, an association that increased in strength in the adjusted model (aOR = 2.65; P = 0.030). Similarly, students who gained confidence in understanding the positive benefits of fruits and vegetables also had nearly three times higher odds (aOR = 2.88; P = 0.045).
Table 4. Logistic regression models. Results of logistic regression models analysing the association between changes in consumption behaviours and various predictors, including knowledge change, confidence change, age, race, gender, ethnicity, and language. An interaction term between knowledge and confidence is also included to explore their combined effect. Unadjusted and adjusted odds ratios (i.e. OR, aOR), 95% confidence intervals, and P-values presented at right (Alpha = 0.05).
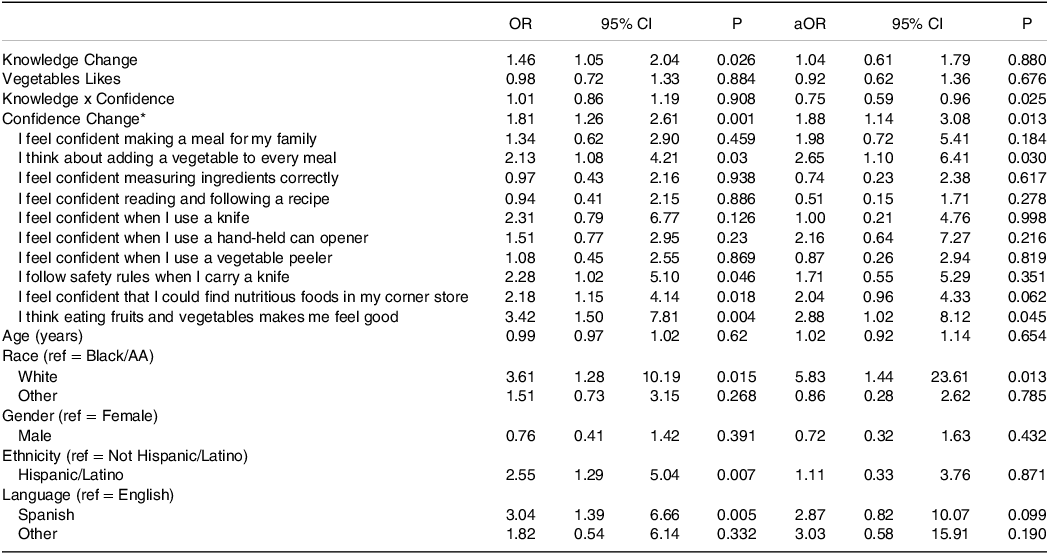
* Excluded from model with individual items.
Compared to Black students, White students were more likely to report consumption changes (aOR = 5.83; P = 0.013). In unadjusted modelling, Hispanic/Latino participants and participants who spoke Spanish had nearly three times higher odds of consumption behaviour changes (Hispanic/Latino OR = 2.55; P = 0.007; Spanish OR = 3.04; P = 0.005). Student age and gender were not associated with behaviour changes.
Vegetable preference changes
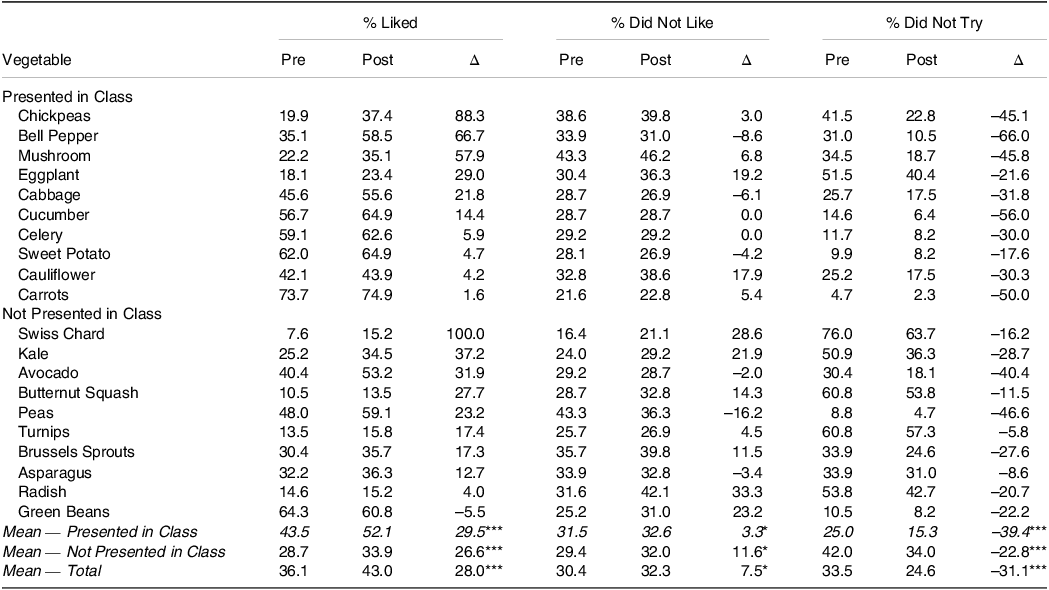
Table 5 presents changes in vegetable preferences from pre- to post-class as well as between vegetables presented in class versus those not presented. Among vegetables presented during class, bell peppers, chickpeas, and mushrooms exhibited the greatest changes in percentage liked, 88%, 67%, and 58%, respectively. On average, vegetables presented during class had higher percentage increase in students who liked them (P < 0.001) and decreases in students who hadn’t tried them (P < 0.001).
Table 5. Vegetable preferences pre- versus post-programme. Comparison of participants’ preferences for various vegetables before and after the intervention. The table includes percentages of vegetables liked, disliked, and not tried, stratified by whether the vegetables were presented during the VCL sessions. Paired t-tests were used to evaluate pre-post differences, with significance levels indicated: ***P < 0.001, *P < 0.05. Alpha = 0.05
Discussion
Students who participated in VCL showed noticeable improvements in cooking confidence and knowledge, indicating the programme’s potential benefits and impact on their dietary habits. Most students also reported individual changes in their consumption behaviours and preferences for certain vegetables. There was a strong positive correlation between students’ knowledge and confidence levels, suggesting that as students gained more knowledge, their confidence also increased. Our analysis identified several predictors of student behaviour changes highlighting potential demographic disparities. Taken together, our findings help to close a gap in understanding the impact of nutritional education in paediatric populations, pointing to multiple opportunities for improving VCL programming and future research and evaluation.
Exposure to healthy foods and culinary skills education can have a positive impact on confidence in meal planning and preparation and knowledge of nutrition and safety.(Reference Garcia, Reardon and McDonald31) Our study highlights the importance of integrating cooking lessons and kitchen skills into educational programmes as a means to improve food preferences, cooking attitudes, self-efficacy, nutrition knowledge, and long-term healthy eating habits in paediatric populations. It emphasises the practical and tangible benefits that can be derived from hands-on cooking experiences and underscores the potential of such interventions in promoting positive dietary behaviours in childhood.
Constraints to behavioural dietary changes are usually multifactorial and are influenced by socioeconomic status, access to food resources, cultural effects, home food availability, and overall food preferences.(Reference Santiago-Torres, Adams and Carrel7,Reference Kris-Etherton, Petersen and Velarde32,Reference Farahmand, Tehrani and Amiri33) For example, children are limited to the types of food their parents provide them which can be impacted by parental nutrition education, cooking skills, familial eating habits, and time and availability to prepare meals. And a child’s larger nutrition environment — for example, school cafeteria, grocery stores, restaurants — determines food choices and quality of foods consumed and this entails areas of food deserts, food swamps, and overall food insecurity.(Reference Kris-Etherton, Petersen and Velarde32) Given VCL was conducted in the surrounding regions of Philadelphia with an unfavourable nutrition environment,(Reference Hirsch and Hillier34–Reference Cannuscio, Weiss and Asch36) the lack of an effect among students who didn’t report behaviour changes could be explained by how much control children actually have over their dietary intake outside of school.
Showing vegetables during lessons was important for exposing students to previously untried items, and could also serve as an opportunity to change negative perceptions and preferences. Prior research shows that incorporating cooking lessons and the teaching of kitchen skills as a component improves participants’ preference for vegetables, positively impacts food and cooking attitudes, and increases self-efficacy and enthusiasm towards assisting with food preparation at home.(Reference Khaodhiar, McCowen and Blackburn5,Reference Cunningham-Sabo and Lohse6,Reference Lavelle, Spence and Hollywood17) Additionally, studies amongst college students have found that incorporating hands-on components such as cooking safety to these sessions is effective in increasing nutrition knowledge, cooking confidence, and ability even further and may promote long-term healthy eating habits.(Reference Howell18)
Cooking skills interventions like VCL that improve cooking confidence and increased fruit and vegetable consumption can promote healthy dietary behaviours, an effect particularly beneficial for economically marginalised populations.(Reference Garcia, Reardon and McDonald31) Although we stratified our results by age, we found no differences across age groups in terms of improvements in cooking confidence, knowledge, or dietary behaviours, contrasting with findings from other studies. For example, Lavelle and colleagues(Reference Lavelle, Spence and Hollywood17) noted that children under 12 years old and teens 13–18 years old had greater confidence in their cooking and food skills, cooking practices, cooking attitudes, diet quality, and health. The authors underscored the ‘importance of learning cooking skills at an early age for skill retention, confidence, cooking practices, cooking attitude and diet quality’.(Reference Lavelle, Spence and Hollywood17) Based on our evaluation of VCL participants, the benefits of cooking skills interventions may be experienced consistently across a wide age range, supporting the inclusion of such programmes at various developmental stages.
Our findings suggest several potential follow-up studies to further understand and improve food confidence and consumption behaviours. Firstly, a long-term follow-up study to track the sustained effects of VCL on students’ food confidence, knowledge, and consumption behaviours over time. Secondly, an intervention modification study that tailors VCL for specific subgroups that showed lower engagement or less demonstrable behaviour changes, aiming to optimise the intervention’s effectiveness and address disparities. Lastly, we propose a qualitative study to explore students’ experiences, perceptions, and barriers, providing valuable insights into the factors influencing confidence, knowledge, and behaviour changes.
The current study is not without limitations. First, as our dataset included only self-reported response from VCL participants, we could not confirm behaviour changes otherwise. Furthermore, our findings may not be generalisable beyond students who participated in VCL in Philadelphia, although they may be transferrable to similar populations in other diverse urban settings, and it is possible that the findings are not generalisable to students who participated in VCL but didn’t complete evaluation surveys. Second, our sample was comprised of VCL participants who completed both baseline and end line surveys, less than 20% of the total participants in the programme. In the absence of information about those who participated in VCL but didn’t complete the surveys, it is possible that there were differences between our sample and the larger pool of VCL students both demographically and as it relates to changes in knowledge, confidence, and consumption behaviours. Third, although HEI has been rigorously evaluated for validity and reliability as a scoring metric that utilises dietary intake data collected from other instruments (e.g. 24-hour recalls, food records or food frequency questionnaires) to determine overall diet quality as well as quality of various dietary components, it does not collect dietary intake data in and of itself as we adapted it for in the current study. Finally, we lacked a control group with which to draw comparisons about the impact of VCL. The lack of a control group limits our ability to establish causality and draws attention to the need for more robust study designs in future research endeavours.
Conclusion
Although family members are usually the primary source of culinary skills for the younger generation, there is great variability with regard to access and knowledge of culinary skills within families. Extracurricular cooking lessons and kitchen skills teaching can supplement and enhance participants’ self-efficacy and enthusiasm towards assisting with food preparation at home. When individuals gain confidence in their ability to cook and prepare meals, they are more likely to engage in these activities independently, leading to a greater sense of empowerment and autonomy in making healthy food choices. As VCL is done as a peer-educational model, it could ultimately be part of larger normative restructuring efforts of food and food preparation culture.
Here we demonstrated that programmes integrating practical cooking skills education along with nutrition can improve confidence and knowledge about healthy food choices amongst children. With this improved confidence and knowledge of healthy foods, we hope to improve attitudes towards healthier foods and in the long term inspire healthier food behaviours. We encourage larger studies to be done in the paediatric setting to see how we can improve and expose children to healthier foods to create long term healthier lifestyles. This has the long-term goal of preventing adolescent and adult obesity.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2024.31
Acknowledgements
The authors thank Vetri Community Partnership for their role in providing Vetri Cooking Lab throughout Greater Philadelphia. We also thank students who participated both in the programme as well as contributed responses to the surveys analysed here.
Financial support
The authors conducted this research as part of their work as employees at their respective institutions without any outside funding. From 2018 to 2019, GlaxoSmithKline provided financial support for Vetri Cooking Lab.
Conflict of interest
None.
Authorship
MB, AN, and SA conceived of and conducted the intervention. AM and MB collected and prepared data for analysis. MK, PC, and SA conducted data analysis. AM, MB, AN, and SA developed the first version of the manuscript draft, and MK, PC, and SA completed the final version of the manuscript draft. All authors reviewed, commented on, and approved of the final draft of the manuscript.








 Open access
Open access