



Introduction
The frontal sinuses generally appear by the age of 1 year, and their growth is almost complete at the age of 20 years.Reference Peynegre, Rouvier, Gershwin and Incaudo1 The embryological development of the frontal sinus is thought to originate from the frontal recessReference Stammberger and Kennedy2 – a complex space within an inverted funnel-like area in which the apex is at the frontal ostium on a sagittal view.Reference Lee, Kuhn and Citardi3 This recess is an embryological continuation of first (agger nasi and uncinate process) and second (bulla ethmoidalis) ethmoturbinalles.Reference Stammberger and Kennedy2 The sinus is thought to be a superior extension of anterior ethmoid cells between anterior and posterior tables of frontal bone.Reference Duque, Casiano, Kountakis, Senior and Draf4
Frontal sinus pneumatisation is highly variable, even between monozygotic twins and indeed even within the same individual, ranging from aplasia to hyperplasia.Reference Kjær, Pallisgaard and Brock-Jacobsen5 Its patterns have been traditionally classified as aplasia, hypoplasia, of medium size and hyperplasia, according to computed tomography (CT) measurements.Reference Guerram, Minor, Renger and Bierry6,Reference Aslier, Karabay, Zeybek and Keskinoğlu7 The extent of frontal sinus pneumatisation is determined in relation to fixed landmarks, including, the supra-orbital line, initially introduced by Libersa and Faber in 1958.Reference Libersa and Faber8 Another component was subsequently introduced as a landmark – a vertical line at the midpoint of both orbits parallel to midsagittal line (mid-orbital line).Reference Guerram, Minor, Renger and Bierry6,Reference Ozcan, Hizli, Sarisoy, Ulusoy and Yildirim9 The superomedial angle of the orbital cavity has also been used as a landmark.Reference Rouviere and Delmas10
Some authors found size categorisation of frontal sinus pneumatisation to be difficult, as it often has an asymmetrical configuration in each subject. They proposed a system of classification by calculating area size and measuring the degree of bilateral asymmetry, the form of scalloping, and the number of septa and complete cells. Each parameter was given a class according to its variation.Reference Szilvassy11,Reference Yoshino, Miyasaka, Sato and Seta12 Some authors used the term ‘frontal sinus hyperaeration’; however, this is a separate and rare entity, of uncertain aetiology, which defines pneumatisation beyond physiological borders.Reference Caylakli, Cagici, Yilmazer, Ozer and Ozluoglu13 A brief literature review of previous relevant studies showed that the majority were concerned with the morphology of frontal sinuses, within the context of forensic medicine, focusing on the identification of unknown people.Reference Yoshino, Miyasaka, Sato and Seta12,Reference Kim, Lee, Park, Kwak and Han14
The degree of frontal sinus pneumatisation may indicate concomitant anatomical variations in adjacent sinuses and be of paramount importance in the interpretation of sinus anatomy pre-operatively.Reference Kim, Lee, Park, Kwak and Han14,Reference Yazici15 This association, however, was limited to patients with the same type of frontal sinus pneumatisation on both sides, and the laterality of concomitant variations was not specified.Reference Yazici15
In order to address issues of asymmetry and laterality, we introduce a unique model to determine more accurately the association between frontal sinus pneumatisation and anatomical variations, by analysing CT scans of the sinus for each side of the head separately and focusing on ipsilateral associations.
Materials and methods
Our institutional review board appraised and approved the study protocol. We reviewed the scans of patients who underwent sinus CT (using the picture archiving and communication system by Multivox, Seoul, Korea) at our hospital between February 2018 and February 2020. All subjects underwent sinus CT examination in a supine position. A 16-slice CT scanner (MX16 Evo2 CT scanner; Philips India, Mumbai, India) was used. All scans were analysed on coronal sections (3 mm slices, as per hospital protocol) and were evaluated by an experienced rhinologist (KHB).
Subjects
A total of 403 individuals who underwent sinus imaging were recruited from the radiological database. Their mean age was 40 years (range, 18–77 years). There were 211 males (52 per cent) and 192 females (48 per cent), with a male-to-female ratio of 1.1:1. Males and females were of a similar age (40.7 vs 38.8 years). Inclusion criteria consisted of patients aged over 18 years who underwent sinus imaging for suspected chronic sinusitis. Patients with frontal sinus aplasia, or a previous history of sinus surgery, sinonasal tumours or trauma to the face, were excluded from the study.
Because of restraints imposed by sinus asymmetry and the laterality of concomitant variation, frontal sinus evaluation was conducted separately for each side of the head (n = 806). We then related it to prevalence of sinus variation on the ipsilateral side. We compared our findings with the literature.
The degree of frontal sinus pneumatisation on paranasal sinus CT scans was determined in relation to two anatomical lines observed on coronal sections, as previously described:Reference Guerram, Minor, Renger and Bierry6,Reference Ozcan, Hizli, Sarisoy, Ulusoy and Yildirim9 specifically, a horizontal line tangent to the superior edges of both orbits (supra-orbital line), and a vertical line across the midpoint of both orbits, parallel to midsagittal line (mid-orbital line). Accordingly, we categorised patients into three frontal sinus pneumatisation groups: type 1 – frontal sinus pneumatisation stays below the supra-orbital line; type 2 – frontal sinus pneumatisation continues beyond the supra-orbital line, but stays medial to the mid-orbital line; and type 3 – frontal sinus pneumatisation continues beyond the supra-orbital line and crosses lateral to the mid-orbital line (Fig. 1).

Figure 1. Paranasal computed tomography image of type 3 frontal sinus pneumatisation on coronal plane, demonstrating a horizontal supra-orbital line and two vertical mid-orbital lines. Frontal sinus pneumatisation in this type continues beyond the supra-orbital line and crosses lateral to the mid-orbital line.
The following anatomical variations were related to frontal sinus pneumatisation, as previously described:Reference Yazici15,Reference Kalavagunta and Reddy16 gender; presence and direction of the nasal septal deviation; extensive maxillary pneumatisation (categorised into three types (I–III) according to the horizontal and vertical dimensions of the maxillary sinus); presence of middle concha pneumatisation; presence of ethmoidal air cell variations (namely, agger nasi, Haller and Onodi cells); pneumatisation of sphenoid bone; and Vidian canal type.
Sphenoid bone pneumatisation, as measured on CT scans in the coronal plane (Fig. 2), includes pneumatisation of the anterior clinoid process, lateral sphenoid recess, pterygoid process and greater wing of the sphenoid. Lateral sphenoid recess pneumatisation has three types:Reference Vaezi, Cardenas, Pinheiro-Neto, Paluzzi, Branstetter and Gardner17 type I – pre-Vidian, absent pneumatisation in the pterygoid recess; type II – intercanal, partially pneumatised pterygoid recess; and type III – post-rotundum, extensively pneumatised pterygoid recess. The Vidian canal has three types:Reference Lee, Kao, Hsu and Lin18 type 1 – canal is completely inside the sphenoid sinus; type 2 – canal is partially protruding into the sphenoid sinus; and type 3 – canal is completely embedded in the sphenoid corpus.

Figure 2. Left sphenoid sinus: area 1 shows the sphenoid sinus proper and area 2 shows sphenoid lateral recess (pterygoid and greater sphenoid) pneumatisation. Arrowhead indicates a type 1 Vidian canal, protruding in the sinus lumen. Larger arrow (bottom) indicates the foramen rotundum. Smaller arrow (top) demonstrates anterior clinoid process pneumatisation.
Analysis
Statistical analysis was performed using SPSS software, version 12.0 (SPSS, Chicago, Illinois, USA). Categorical and ordinal variables were summarised as frequencies and percentages. The associations of demographics and pneumatisation patterns with the prevalence of anatomical variations were assessed for statistical significance: univariate analysis was performed using the Pearson's chi-square test for categorical and ordinal variables. Where p ≤ 0.05, the finding was considered statistically significant.
Results
Imaging scans for each side of the participants’ heads were divided into three groups according to frontal sinus pneumatisation type, and prevalence of ipsilateral anatomical variants for each type was evaluated separately, as demonstrated in Table 1.
Table 1. Prevalence of ipsilateral paranasal sinus CT variations according to frontal sinus pneumatisation type*
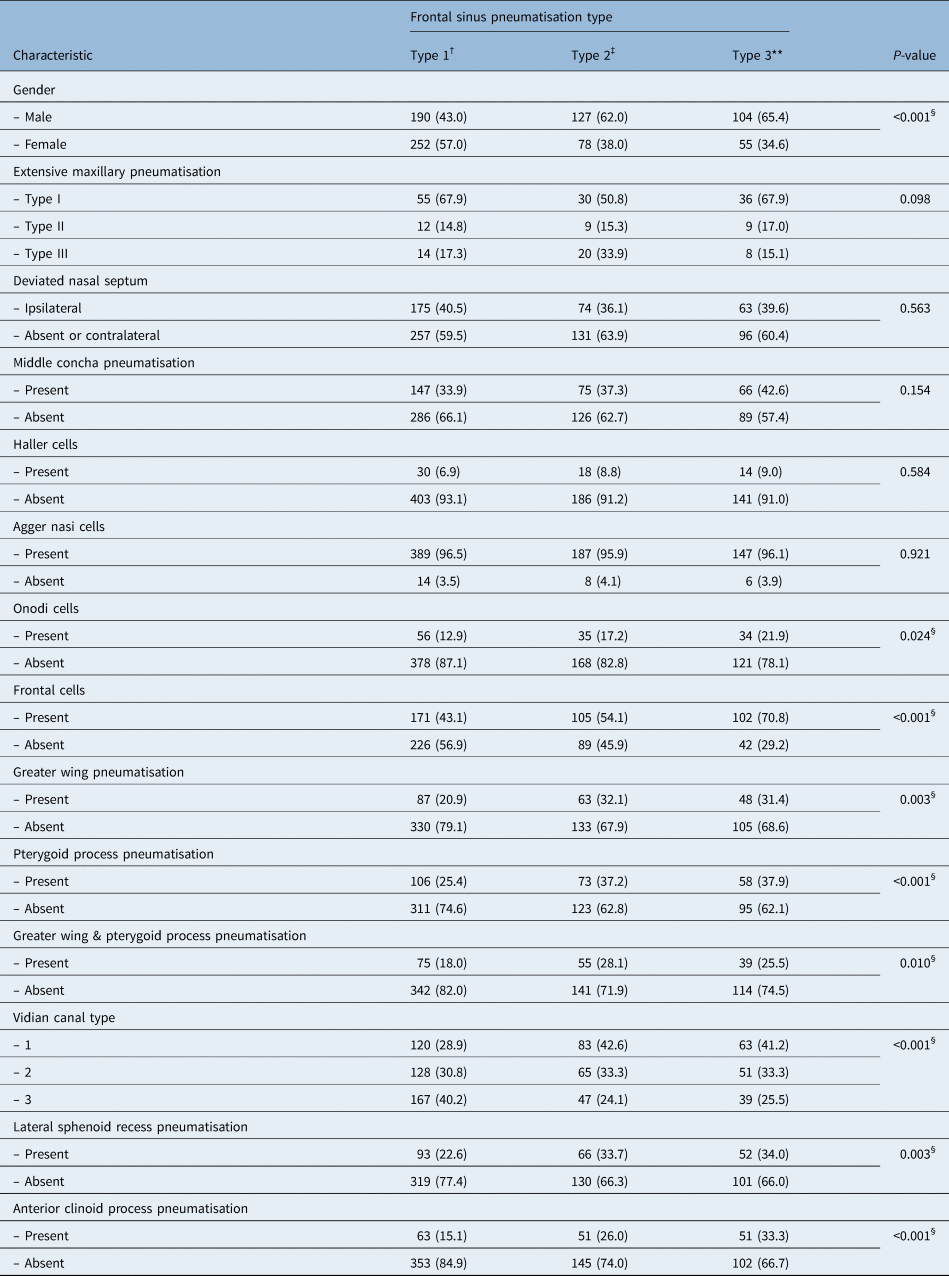
Data represent numbers (and percentages) of cases, unless indicated otherwise. *Total n = 806; †n = 442; ‡n = 205; **n = 159. §Indicates statistical significance. CT = computed tomography
There was significantly more type 2 and 3 frontal sinus pneumatisation in males (p < 0.001), as well as a positive association with anterior clinoid process pneumatisation (p < 0.001). There was a significant association between frontal sinus pneumatisation and variations of pneumatisation in the sphenoid sinus (lateral sphenoid recess, greater wing, pterygoid process and Vidian canal), as well as frontal and Onodi cells. Frontal sinus pneumatisation was not associated with a deviated nasal septum, middle concha pneumatisation or extensive maxillary pneumatisation.
Discussion
The true prevalence of degrees of frontal sinus pneumatisation remains unknown as there has not been a proven objective classification system. The overall prevalence of hyperplasia (type 3) of sinus sides in our series was 19.6 per cent (n = 159). This was lower than the reported rate of 44.5 per cent.Reference Aslier, Karabay, Zeybek and Keskinoğlu7 However, 54.8 per cent of sinus sides (n = 442) were hypoplastic, which is substantially higher than previously reported rates of 14.2 per centReference Aslier, Karabay, Zeybek and Keskinoğlu7 and 15 per cent.Reference Zeifer19 This might be related to ethnic differences. Measured variables that were shown to affect frontal sinus pneumatisation included dimensions of the frontal sinus peak, and the presence of supra-orbital and frontal cells.Reference Yüksel Aslier, Karabay, Zeybek, Keskinoğlu, Kiray and Sütay20,Reference Meyer, Kocak, Smith and Smith21 We noted that the presence of frontal cells was positively associated with frontal sinus pneumatisation (p < 0.001) (Table 1).
Variability of frontal sinus pneumatisation can even be seen within the same individual.Reference Kjær, Pallisgaard and Brock-Jacobsen5,Reference Aslier, Karabay, Zeybek and Keskinoğlu7 Right and left frontal sinuses develop independently from each other as a result of bone resorption and septations.Reference Duque, Casiano, Kountakis, Senior and Draf4 This was noted in 21.5 per cent of our subjects where the degree of frontal sinus pneumatisation on the two sides was asymmetric. Hyperplasia was more frequently observed on the left side.Reference Duque, Casiano, Kountakis, Senior and Draf4,Reference Aslier, Karabay, Zeybek and Keskinoğlu7,Reference Pondé, Andrade, Via, Metzger and Teles22,Reference Tatlisumak, Ovali, Asirdizer, Aslan, Ozyurt and Bayindir23 This may be due to the asymmetric predominance of chewing stress on the left side, or the conventional trend of lying on the right side, which determines the direction of pneumatisation through the frontal bone for ethmoidally derived frontal sinuses.Reference Prossinger24 In our series, hyperplasia was evenly distributed on either side (19.2 per cent on the right and 20.3 per cent on the left), but not necessarily within the same individual, as 19.6 per cent of subjects showed asymmetry.
When we analysed gender differences between the three groups, we observed that more females had type 1 frontal sinus pneumatisation, and more males had type 2 and type 3 frontal sinus pneumatisation (Table 1). The difference was statistically significant (p < 0.001). This is in concordance with the findings of Yazici, who observed more females with type 1 frontal sinus pneumatisation and more males with type 3 frontal sinus pneumatisation, a difference which was also statistically significant (p = 0.012).Reference Yazici15 The larger size of the frontal sinus in males is implied in many studies, and this feature is even used to determine gender identity in forensic medicine.Reference Tatlisumak, Ovali, Asirdizer, Aslan, Ozyurt and Bayindir23,Reference Lee, Sakai and Spiegel25,Reference Hamed, El-Badrawy and Fattah26
Regarding the presence and direction of a deviated nasal septum, there was no statistically significant difference amongst the three frontal sinus pneumatisation types (p = 0.563). This is in concordance with the findings of Yazici, who also found no statistically significant difference (p = 0.785).Reference Yazici15
When we addressed prevalence of ethmoidal complex variations, the type 3 group had the highest middle concha pneumatisation (42.6 per cent), but the difference was not significant (p = 0.154). When we examined agger nasi, Hallar and Onodi (sphenoethmoid) cells, the prevalence of the latter was significantly higher (21.9 per cent) in type 3 frontal sinus pneumatisation (p = 0.024). These cells pneumatise laterally and somewhat superiorly to the sphenoid sinus, and were identified by a horizontal bony plate dividing the sphenoid sinus.Reference Meyer, Kocak, Smith and Smith21 In comparison, Yazici reported the type 3 group to have the highest middle concha pneumatisation and highest prevalence of Haller cells, with significant associations (p = 0.011 and p = 0.010).Reference Yazici15
Regarding the maxillary sinus, we found no association between frontal sinus pneumatisation and extensive maxillary pneumatisation (p = 0.098). We were unable to compare this association with previous findings in the literature as these data were unavailable.
Regarding variations in sphenoid bone, the prevalence of pterygoid process pneumatisation in our series was 37.6 per cent, which is higher than reported in other studies (18.3 per cent,Reference Yazici15 29 per cent,Reference Hewaidi and Omami27 22 per centReference Lu, Pan, Qi, Shi, Zhang and Wu28 and 9.3 per centReference Tawfik, El-Fattah, Nour and Tawfik29). The prevalence of greater wing pneumatisation was 32.6 per cent; this was equivalent to the results of some studies (e.g. 29.2 per centReference Yazici15 and 31.8 per centReference Tawfik, El-Fattah, Nour and Tawfik29) and higher than reported in others (e.g. 20 per centReference Lu, Pan, Qi, Shi, Zhang and Wu28 and 21.2 per centReference Lu, Pan, Qi, Shi, Zhang and Wu28). In contrast, the prevalence of co-existence of pterygoid process and greater wing pneumatisation was 37.3 per cent, more than double the reported rate of 15.8 per cent.Reference Yazici15
We found that type 2 and 3 frontal sinus pneumatisation groups had the highest prevalence of pterygoid process and greater wing pneumatisation, as well as both combined, and the difference was significant (p = 0.001, p = 0.003 and p = 0.010 respectively) (Table 1). Yazici reported similar observations and, likewise, the associations were highly significant (p = 0.006, p < 0.001 and p = 0.003 respectively).Reference Yazici15
Another variation in sphenoid bone is the anterior clinoid process pneumatisation, the posteromedial projection of the lesser sphenoid wing surrounded by vital structures.Reference da Costa, de Oliveira Santos, de Araujo Paz, Rodrigues, Abdala and Centeno30 The prevalence of anterior clinoid process pneumatisation reported in the literature varied from 6 to 35.5 per cent,Reference Burulday, Muluk, Akgül, Kaya and Öğden31,Reference Arslan, Aydınlıoğlu, Bozkurt and Egeli32 and the rate reported in our series and in Yazici's study were within this range (28.5 per cent and 29.2 per cent respectively).Reference Yazici15 The prevalence of anterior clinoid process pneumatisation in both our study and Yazici's study was higher for the type 3 frontal sinus pneumatisation group (41.2 per cent), compared to type 1 and 2 groups, with significant differences (p = 0.012 and p < 0.001 respectively). Additionally, both studies noted a significant association between bilateral anterior clinoid process pneumatisation and type 3 frontal sinus pneumatisation (p < 0.001).Reference Yazici15
• Frontal sinus pneumatisation is highly variable, classified as aplasia, hypoplasia, medium size or hyperplasia
• Hyperplasia is more common in men, and on the left side of the body
• Frontal sinus hyperplasia may indicate concomitant anatomical variations in adjacent sinuses, emphasising the importance of interpreting sinus anatomy pre-operatively
• The association, however, was limited to patients with same frontal sinus pneumatisation type on both sides, and did not indicate laterality of concomitant variations
• A unique model is introduced to establish the association between frontal sinus pneumatisation and anatomical variations
• There were significant associations of frontal sinus hyperplasia with sphenoid sinus pneumatisation, frontal and Onodi cell presence, and Vidian canal exposure
We also established the likelihood of encountering an exposed Vidian canal in the sphenoid sinus in patients with frontal sinus hyperplasia. A type 1 Vidian canal (canal is completely inside the sphenoid sinus) occurred in 33 per cent of sinus sides, and its prevalence was significantly higher in the type 2 and 3 frontal sinus pneumatisation groups, compared to the type 1 frontal sinus pneumatisation group (42.6 per cent, 41.2 per cent and 28.9 per cent respectively) (p < 0.001). Our finding is concordant with the literature; indeed, many authors have warned about the risk of encountering the vulnerable Vidian canal when approaching the skull base in patients with frontal sinus hyperplasia.Reference Yazici15,Reference Lee, Kao, Hsu and Lin18,Reference DeLano, Fun and Zinreich33,Reference Itagi34
Conclusion
We introduced a unique model to determine more accurately the association between frontal sinus pneumatisation and ipsilateral anatomical variations by analysing CT scans of sinuses on each side of individuals’ heads. We found significant associations between type 3 frontal sinus pneumatisation (hyperplasia) and pneumatisations of the anterior clinoid process, lateral sphenoid recess, pterygoid process and greater wing, as well as exposure of the Vidian canal. The type 3 frontal sinus pneumatisation group also showed significant associations with male gender and the presence of frontal and Onodi cells. Direct attention to ipsilateral variation when interpreting CT scans pre-operatively can be informative in endoscopic sinus and skull base surgery, particularly in patients with frontal sinus hyperplasia.
Acknowledgement
We acknowledge Mrs Oraib Faraheed for performing the statistical analysis.
Competing interests
None declared



