



Introduction
In 2019, more than 3.5 million children were the subject of an investigation by child protective services (CPS) in the United States (U.S. Department of Health and Human Services [USDHHS] et al., 2019). Previous research has illustrated that the highest risk of maltreatment is during the first few years of life (Wildeman & Waldfogel, Reference Wildeman and Waldfogel2014). Young children are disproportionately more likely to be involved with CPS, with children under 2 years old making up more than one quarter (28.1%) of all victims (USDHSS et al., 2019). This is especially concerning because early childhood is an important period that sets the foundation for long-term development across the lifespan (Heckman, Reference Heckman2008). Previous research has found that children with a history of maltreatment are more likely to experience worse outcomes across multiple developmental domains and across the lifespan (Brown et al., Reference Brown, Anda, Edwards, Felitti, Dube and Giles2007; Chapman et al., Reference Chapman, Wheaton, Anda, Croft, Edwards, Liu, Sturgis and Perry2011; Clarkson Freeman, Reference Clarkson Freeman2014; Dong et al., Reference Dong, Anda, Felitti, Dube, Williamson, Thompson and Giles2004; Huang et al., Reference Huang, Yan, Shan, Chen, Li, Luo, Gao, Hao and Liu2015; Reiser et al., Reference Reiser, McMillan, Wright and Asmundson2014; Yoon, Reference Yoon2017). Additionally, children who experience maltreatment are at-risk for maladaptive outcomes, regardless of substantiation status (English et al., Reference English, Bangdiwala and Runyan2005; Hussey et al., Reference Hussey, Marshall, English, Knight, Lau, Dubowitz and Kotch2005; Widom, Reference Widom2014).Yet not all children display poor outcomes after experiencing maltreatment, and instead illustrate resilience. Resilience is a complex construct and currently, there is limited empirical evidence on the multidimensional, longitudinal nature of resilience among young children who experience maltreatment. Therefore, the current study seeks to focus on identifying patterns of resilience trajectories among children who experience maltreatment very early in life.
Young children’s development after experiencing maltreatment
Experiencing maltreatment in the first 2 years of life might be particularly detrimental because it could undermine foundational skills and contribute to long-term maladaptive outcomes (Heckman, Reference Heckman2008). Additionally, children who experience maltreatment during very young ages are at risk of chronic maltreatment across developmental periods (Russotti et al., Reference Russotti, Warmingham, Duprey, Handley, Manly, Rogosch and Cicchetti2021). Previous research focusing on young children who experience maltreatment demonstrated increased risk of worse outcomes, including impaired cognition, language, and behavioral functioning. For example, studies have shown that 20%–36% of children younger than 5 years old in the CPS system have a documented developmental delay or disability (Lightfoot et al., Reference Lightfoot, Hill and LaLiberte2011). Child maltreatment during early childhood is especially harmful because it impairs the development of the prefrontal cortex, a brain region involved in complex behaviors such as executive functioning (Lupien et al., Reference Lupien, McEwen, Gunnar and Heim2009). Previous work has found that, compared to non-maltreated children, children who experience maltreatment performed significantly lower on a memory task which suggested impaired executive functioning (Augusti & Melinder, Reference Augusti and Melinder2013).
In regard to language development, children who experienced maltreatment early in life have shown less optimal language skills across multiple domains (i.e., receptive, expressive, and pragmatics) when compared to children who did not experience maltreatment (Eigsti & Cicchetti, Reference Eigsti and Cicchetti2004; Sylvestre et al., Reference Sylvestre, Bussières and Bouchard2016). Among maltreated infants, children’s auditory and expressive communication scores decreased significantly from intake to the infants’ first birthday regardless of removal status (i.e., remaining in home or placement with kin or nonkin caregivers; Stacks et al., Reference Stacks, Beeghly, Partridge and Dexter2011).
Similarly, studies have found a significant association between early child maltreatment and maladaptive behaviors, such as poor social adaption and behavior problems (Font & Berger, Reference Font and Berger2015). For example, the Minnesota Mother-Child Project identified four maltreatment groups from home observations 7 and 10 days postpartum and when infant were 3,6, and 12 months. Results demonstrated that children who experienced physical neglect had the least effective coping strategies and showed more signs of tantrums, stealing, and self-punishing behaviors compared to other maltreatment groups (Egeland & Sroufe, Reference Egeland, Sroufe, Cicchetti and Rizley1981; Egeland et al., Reference Egeland, Sroufe and Erickson1983). Physical abuse has also been positively associated with early childhood aggression (Yoon et al., Reference Yoon2017) and chronic exposure to child maltreatment is linked to lower IQ scores and more externalizing and internalizing problems (Jaffee & Maikovich-Fong, Reference Jaffee and Maikovich-Fong2011). Taken together, these studies demonstrate that the consequences of maltreatment are complex, and detrimental to children’s development.
Resilience after child maltreatment
Despite all the risks associated with experiencing abuse and neglect, some children can display positive development and exhibit resilience (Luthar et al., Reference Luthar, Cicchetti and Becker2000; Masten & Coatsworth, Reference Masten and Coatsworth1998). Although resilience has been studied for several decades, there is still not a universal definition (Yoon et al., Reference Yoon, Howell, Dillard, McCarthy, Napier and Pei2019). Generally, resilience is considered a process of positive adaptation in the context of risk rather than a personality trait (Masten, Reference Masten2001). However, there is heterogeneity in whether positive adaptation is conceptualized as performing better compared to others who experience similar risks (Rutter, Reference Rutter2006) or performing as well as others who do not experience similar risks (Luthar et al., Reference Luthar, Cicchetti and Becker2000; Sattler & Gershoff, Reference Sattler and Gershoff2019). Although there is no consensus on which conceptualization of resilience should be used or whether children need to demonstrate resilience across multiple developmental domains at a given time, research studies should be clear in their operationalization of resilience (Popham et al., Reference Popham, McEwen, Pluess and Ungar2021; Ungar, Reference Ungar2021). The current study draws upon a multisystems perspective, and thus, resilience is defined as “the capacity of a dynamic system to adapt successfully through multisystem processes to challenges that threaten the function, survival, or development of the system” (Masten et al., Reference Masten, Lucke, Nelson and Stallworthy2021, p. 524). Specifically, we assessed whether a child demonstrates positive adaptation across three developmental domains (i.e., cognitive, language, and behavioral) following the exposure to child maltreatment. Positive adaptation is characterized by demonstrating similar levels of adaptation in a specific developmental domain as a non-maltreated sample.
In addition to variations in the definitions of resilience, there are also wide ranges in the rates of resilience across studies based on how and when resilience was measured. In some studies resilience is assessed based on a single developmental domain. For example, in a study of 5- to 9-year-olds living in foster care, between 27.5% to 70.9% of children demonstrated behavioral resilience depending on the type and number of indicators (e.g., emotional problems, conduct problems, or prosocial behaviors; Bell et al., Reference Bell, Romano and Flynn2013). Further, Jaffee and Gallop (Reference Jaffee and Gallop2007) cited approximately a third of children demonstrated resilience in one developmental domain at one time point following maltreatment, but only 14%–22% of children demonstrated resilience in a given domain across multiple time points.
In contrast, other studies have classified resilience as a multidimensional construct and therefore measured multiple developmental domains (Dubowitz et al., Reference Dubowitz, Thompson, Arria, English, Metzger and Kotch2016; Kinard, Reference Kinard1998; Sattler & Font, Reference Sattler and Font2018; Yoon et al., Reference Yoon, Pei, Logan, Helsabeck, Hamby and Slesnick2022). For example, in a study of 2–6-year-old children who experienced maltreatment, resilience was defined as a child performing adequately (i.e., better than 1 SD below the mean) for all 3 domains of resilience (behavioral, social, and developmental). In this study, 46% of children exhibited resilience (Dubowitz et al., Reference Dubowitz, Thompson, Arria, English, Metzger and Kotch2016). Yet another study investigated resilience as a multidimensional construct in children involved in the child welfare system prior to the age of one, but defined resilience as reaching normal developmental standards despite experiencing maltreatment. This study found that 38% of the sample exhibited social resilience, 25% cognitive resilience, and 11% multi-domain resilience (both social and cognitive; Sattler & Font, Reference Sattler and Font2018). Similarly, a recent study conceptualized resilience as a multifaceted construct and identified three distinct profiles of resilience among young children (3–5 years old) involved in the child welfare system (Yoon et al., Reference Yoon, Pei, Logan, Helsabeck, Hamby and Slesnick2022). This study found that a little over half of the sample showed multi-domain resilience, 24% low cognitive resilience, and 20% low emotional and behavioral resilience. Further, in a study of children aged 8 to 10 years who experienced maltreatment, rates of resilience varied between 45% to 94% depending on whether resilience was based on academic, behavioral, or social indicators (Walsh et al., Reference Walsh, Dawson and Mattingly2010). Although each of these studies incorporated a multidimensional perspective of resilience, these estimates did not capture the mutable nature of resilience since it was only assessed once.
Developmental trajectories of resilience remain understudied since the majority of resilience research to date has focused on resilience as an outcome at a single time point. Based on longitudinal studies investigating developmental trajectories after experiencing a variety of adversities (e.g., community violence or terrorist attacks), there is evidence that resilience increases across the life course (Eisman et al., Reference Eisman, Stoddard, Heinze, Caldwell and Zimmerman2015; Norris et al., Reference Norris, Tracy and Galea2009; Werner, Reference Werner1989). Among adolescents who experienced maltreatment, Oshri et al. (Reference Oshri, Topple and Carlson2017) examined growth trajectories of social resilience across three waves and found significant positive growth of prosocial behavior (e.g., cooperation, assertion, responsibility, and self-control) over time. Results demonstrated a 4-class solution, with 17.10% of the sample in the breakdown group (high intercept and large, negative slope), 17.40% in the stress-resistant group (high intercept and small, positive slope), 10.10% in the emergent resilience group (low intercept and large, positive slope), and 55.40% in the unresponsive-maladaptive group (low intercept and small, negative slope). Similarly, Proctor et al. (Reference Proctor, Skriner, Roesch and Litrownik2010) examined behavioral resilience in 6- to 14-year-olds placed in early foster care. Using growth mixture modeling, they classified three internalizing trajectories: stable adjustment (66.7%), mixed/decreasing adjustment (25.4%), and increasing adjustment (7.9%). When it came to externalizing trajectories, they identified four: stable adjustment (46.6%), mixed adjustment (28.7%), increasing adjustment (8.2%), and stable maladjustment (16.5%). In another study, Holmes and colleagues (2018) examined language/academic functioning in 0- to 5-year-olds who have been reported to CPS. Using growth mixture modeling they determined five language/academic trajectories: high stable (21.5%), low increasing (20.1%), low stable (19.9%), high decreasing group (21.4%), and decrease/recover/decrease (17.1%).
One study conceptualized resilience based on a multidimensional, longitudinal construct. In this study, resilience was based on a count of positive adjustment across different developmental domains and results demonstrated that resilience increased among adolescents involved in CPS (Yoon et al., Reference Yoon, Sattler, Knox and Xin2021). A similar trend of increasing resilience over time was observed in a study that focused on resilience during early childhood (Dubowitz et al., Reference Dubowitz, Thompson, Arria, English, Metzger and Kotch2016). Specifically, resilience was operationalized as competencies across behavioral, social, and developmental domains following exposure to maltreatment and other adversities and results indicated that only 29% of the children showed resilience at age 4 but the number increased to 52% at age 6 years. Even though these studies examined various trajectories of resilience, the samples either focused on adolescents or these studies only focused on a single domain of resilience. Given the wide variation in developmental periods and conceptualizations of resilience (e.g., multidimensional vs. single-domain) in previous research it is challenging to compare or synthesize findings across the studies. Additionally, there is gap in the literature on resilience trajectories among very young children involved in CPS despite representing the greatest risk of CPS involvement. The current study builds upon prior work by using a multidimensional, longitudinal construct of resilience among young children involved in CPS.
Initial placement setting, caregiver behaviors, and resilience
The extent to which children demonstrate resilience may vary based on whether children remain in-home following contact with CPS or if they are placed in out-of-home care (Berger et al., Reference Berger, Bruch, Johnson, James and Rubin2009). Children who are placed in out-of-home care likely experienced more severe maltreatment compared to children who remained in home (U.S. Department of Health and Human Services, 2005), and it is difficult to disentangle the effects of maltreatment and removal (Dozier & Rutter, Reference Dozier, Rutter, Cassidy and Shaver2016). Attachment theory can provide a framework for understanding children’s ability to display resilience based on their initial placement type. According to attachment theory, when caregivers are responsive and sensitive during periods of distress children develop secure attachment (Main & Solomon, Reference Main, Solomon, Greenberg, Cicchetti and Cummings1990); which is essential for long-term positive development (Sroufe, Reference Sroufe2005). Conversely, children form insecure and disorganized attachments when their caregiver is unavailable, unresponsive, or engages in abusive and neglectful behavior. Particularly among young children, experiencing maltreatment may impede children’s ability to form secure attachment relationships (Cicchetti et al., Reference Cicchetti, Rogosch and Toth2006; Cyr et al., Reference Cyr, Euser, Bakermans-Kranenburg and Van Ijzendoorn2010), and this could lead to maladaptive development. Placement in foster care provides an immediate respite from severe maltreatment and could also provide the opportunity to establish new attachment relationships or modify negative internal working models (Ponciano, Reference Ponciano2010; Stovall-McClough & Dozier, Reference Stovall-McClough and Dozier2004). Yet, experiencing removal may be detrimental by itself (Folman, Reference Folman1998) and children enter foster care for a variety of reasons (e.g., parental death, parental incarceration) that may be differentially associated with resilience. Therefore, it might be important to remain in-home to provide the least disruption and to maintain closeness and connection to birth parents in certain situations. The evidence regarding placement setting on children’s development is mixed (Berger et al., Reference Berger, Bruch, Johnson, James and Rubin2009) and, therefore, warrants an investigation on the association between placement setting and children’s trajectories of resilience.
Although the potential benefits of placement setting might not be straight forward, positive caregiving behaviors are one of the strongest, most frequently cited protective factors in the literature (Afifi & Macmillan, Reference Afifi and MacMillan2011; Masten, Reference Masten2018). In particular, emotionally responsive and cognitively stimulating caregiving behaviors might be beneficial for children who experience maltreatment (Harden & Whittaker, Reference Harden and Whittaker2011). Emotionally supportive behaviors are characteristic of nurturing, warm, responsive interactions between caregivers and children, whereas cognitive stimulating behaviors encompass behaviors such as book reading, practicing the alphabet, and encouraging language development (Bradley & Corwyn, Reference Bradley and Corwyn2005). Prior research has illustrated that nurturing behavior from the non-offending parent is especially beneficial for children who experience maltreatment (Rosenthal et al., Reference Rosenthal, Feiring and Taska2003). Jaffee (Reference Jaffee2007) found that sensitive and stimulating caregiving was linked to better behavioral and cognitive outcomes among children involved in CPS who had increased neurodevelopmental risk. In a sample of children involved in CPS before age one, Sattler and Font (Reference Sattler and Font2018) found that cognitively stimulating behavior was associated with social, cognitive, and multidomain resilience, whereas emotional support was associated with cognitive resilience only. However, these associations differed by whether children were in in-home or out-of-home care. To our knowledge there has yet to be a study examining whether emotionally responsive and cognitively stimulating parenting behaviors are associated with trajectories of resilience among young children involved in CPS.
The current study
Child maltreatment is a serious risk factor for children’s development; however, some children are able to display resilience in spite of experiencing abuse and neglect. Much of the prior research on resilience has either focused on a single domain of resilience, focused on resilience at a single point in time, or focused on adolescents involved in CPS. The current study expands upon prior literature by modeling resilience as a multidimensional, longitudinal construct of resilience among very young children (i.e., less than 2 years old) involved in CPS. Given the exploratory nature of person-centered trajectory analyses, we do not have a hypothesis on the expected number or pattern of resilience trajectories. In addition, the current study investigates whether placement setting, and caregiving behaviors are associated with patterns of resilience trajectories. Given the conflicting literature regarding placement type, we do not have an expected direction of how this would influence resilience trajectories, but we expect higher levels cognitive stimulation and emotional support to be positively associated with increasing resilience based on the broader literature.
Method
Data and sample
The current study used data from the National Survey of Child and Adolescent Well-Being (NSCAW I). NSCAW I is nationally representative and longitudinal sample of 5,501 children involved in CPS who are between 0 to 14 years old. The first wave of data collection began in 1999 and there are three additional complete waves of data that occurred approximately 18 months apart (Waves 1, 3, 4, and 5; Dowd et al., Reference Dowd, Kinsey, Wheeless, Thissen, Richardson, Suresh and Smith2008). Specifically, data collection was based on when CPS investigation was closed and wave 1 occurred soon after. Data collection occurred 18 months since investigation for wave 3 and occurred 36 months after the investigation for wave 4, which creates 18-month intervals between waves of data collection. Wave 2 was not a full interview and therefore not included in analyses. Data were collected using questionnaires and direct observations from children, caregivers, and child welfare caseworkers. The current study focused on children who were involved in CPS in the first 2 years of life. Therefore, the sample was limited to children who were less than 2 years old at wave 1 (n = 1,699). The average age of children was approximately 13 months at wave 1, 29 months at wave 3, and 45 months at wave 4 (SD was 6 months at all waves). Descriptive statistics of the sample can be found in Table 1. The data are restricted access and not available for distribution by the authors. This study was not preregistered. This study was found exempt by the institutional review board at the University of North Carolina at Greensboro because it was solely secondary data analysis of deidentified data.
Table 1. Descriptive statistics of sample (n = 1,699)
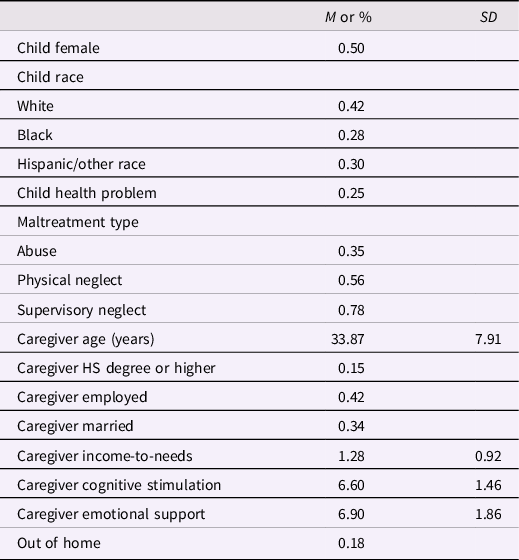
Note. HS = high school. All measures from wave 1.
Measures
Resilience
In recognition of resilience as a multi-domain construct, resilience was measured using a composite score of adaptive functioning in several developmental domains (i.e., behavioral, language, and cognitive), which are detailed below. Each assessment selected included standardized assessments with scores normed on a not-at-risk sample. Thus, resilience could range from 0 to 3 domains. Resilience scores were measured at Waves 1, 3, and 4 because these are when the outcome measures are available.
Behavioral resilience was measured based on the daily living skills from the Vineland Adaptive Behavior Scale Screener (Sparrow et al., Reference Sparrow, Carter and Cicchetti1993). For children 0–2 years of age, the daily living skills assessed from caregiver report on behaviors such as eating, dressing, toileting, general safety, and household tasks. Internal consistency was good for all waves, α = .91 for 0- to 2-year-old children and α = .77 for 3-to-5-year-old children. Standard scores were computed for the daily living skills domain within different age groups. Behavioral resilience was considered demonstrating the average or higher score (i.e., 100 or higher on the Vineland scale).
Resilience in language was assessed using the Preschool Language Scale-3 (PLS-3; Zimmerman et al., Reference Zimmerman, Steiner and Pond1992). The PLS-3 measured auditory comprehension and expressive communication among children from birth to 5 years old. The PLS-3 was administered by trained interviewers and the Total Language score had good internal consistency (α = .87, range from .74 to .94). Standard scores were computed for the total language scale. Language resilience was considered demonstrating the average or higher score (i.e., 100 or higher on the PLS-3).
Cognitive resilience was measured based on the Battelle Developmental Inventory & Screening Test, which is a standardized assessment of cognitive development for children up to age 8 (BDI; Newborg et al., Reference Newborg, Stock, Wnek, Guidubaldi and Svinicki1984). The BDI was administered by trained interviewers to children through age 4 and to children over age 4 if their Kaufman Brief Intelligence Test score was zero. According to the user manual, internal consistency was not reported for this measure but has demonstrated high validity and good test–retest reliability (Newborg et al., Reference Newborg, Stock and Wnek1988). The cognitive scale assessed conceptual development, memory, perceptual discrimination, and reasoning and academic skills. A cognitive development quotient (CDQ) was created for the cognitive scale based on the publisher’s scoring (Newborg et al., Reference Newborg, Stock and Wnek2005). Cognitive resilience was considered average or higher CDQ (i.e., 100 or higher on the BDI).
Out-of-home care
Overall placement type was based on caregiver, child, and caseworker reports. Out-of-home setting was based on derived variables at Wave 1 provided in the dataset. In-home settings were based on whether or not the child was currently in an out-of-home setting and the child’s relationship to the primary caregiver. If no discrepancies existed between reported placement setting, then placement type was based on a non-missing value from the interviews. If there were discrepancies, then caregiver reported setting took priority, followed by youth report and caseworker report. A dichotomous indicator was created with 1 = “Out-of-home placement” and 0 = “In-home placement.”
Caregiver parenting behaviors
Caregiving behaviors were measured using the Home Observation for Measurement of the Environment (HOME; Bradley, Reference Bradley and Reese1994; Bradley et al., Reference Bradley, Corwyn, Burchinal, McAdoo and García Coll2001) at Wave 1. The HOME scales included both caregiver reports and interviewer observations of caregivers’ behaviors and the physical environment. The HOME included age-specific items for the age groups of 0–2 years, 3–5 years, and 6–10 years. Caregiver cognitive stimulation and emotional support were assessed using the Cognitive Stimulation subscale and the Emotional Support subscale. Both Cognitive Stimulation and Emotional Support are continuous scales based on the summation of relative indicators, with higher scores indicating more positive behaviors.
Covariates
All analyses included child and caregiver covariates drawn from the wave 1 assessment. Child-level covariates included sex (0 = male; 1= female), race (White, Black, Hispanic/other race), child chronic health problem (0 = no; 1 = yes). Caregiver covariates included age, education level (0 = less than high school degree; 1 = high school degree or more), employment status (0 = no employment; 1 = any employment), marital status (0 = not married; 1 = married), and income-to-needs ratio (based on household income and household size). Analyses also controlled for maltreatment type, which was based on the caseworkers’ risk assessment and allegation type. Maltreatment type included non-mutually exclusive dichotomous indicators of abuse (physical or sexual), physical neglect, and supervisory neglect.
Analytic approach
All analyses were conducted in Mplus version 8.5 (Muthén & Muthén, 2017), and missing data were accounted for using full information maximum likelihood (FIML) for dependent variables. According to the Stata command (mcartest), the results of this test suggest that data were consistent with a pattern of missing at random based on the covariate-dependent missing assumption extension of Little’s Missing Completely at Random (MCAR) test (Li, Reference Li2013). Repeated measures latent class analysis (RMLCA; Collins & Lanza, Reference Collins and Lanza2010) was used to investigate the number and pattern of trajectories of resilience. RMLCA is one approach to capture patterns of growth using dichotomous or categorical variables (Collins & Lanza, Reference Collins and Lanza2010). RMLCA is a longitudinal application of latent class analysis, in which a limited number of indicators are assessed across at least three time points. Although not a traditional growth mixture model, RMLCA is still considered to be one way of modeling trajectories (Collins & Lanza, Reference Collins and Lanza2010; Wright & Hallquist, Reference Wright and Hallquist2014). RMLCA can model nonparametric change and is able to accommodate indicators with irregular change across time (Killian et al., Reference Killian, Cimino, Weller and Hyun Seo2019; Wright & Hallquist, Reference Wright and Hallquist2014). Another unique advantage of RMLCA, is it clearly illustrates how each indicator changes across different trajectories. Similar to latent class analysis, RMLCA involves a class enumeration process in which each model was compared to consecutively more complex models using the Bayesian Information Criterion (BIC) and adjusted BIC (ABIC) to determine the number of classes that best fit of the model to the data. Smaller BIC/ABIC values indicate a better model fit, such that a model of k classes fits better than the k-1 class model (Nylund et al., Reference Nylund, Asparouhov and Muthén2007). The data were weighted with analytic sample weights, which is not compatible with Lo-Mendell-Rubin Adjusted or Bootstrapped Likelihood Ratio Tests (Muthén, Reference Muthén2016). Classes also needed to contain a minimum of 50 cases (Weller et al., Reference Weller, Bowen and Faubert2020). In conjunction with comparing these fit statistics, model fit was also based on examination of a line graph of the BIC and ABIC values to determine where the values leveled off. We also considered entropy, interpretability, and parsimony of the latent classes in model selection. We estimated between a one and seven class solution.
Next, we examined the predictors of resilience trajectories. Based on the best fitting model of three trajectories, we included a regression equation where the categorical latent variable of trajectory class membership was regressed on out-of-home placement status, caregiver behaviors, and all covariates using the R3STEP command (Asparouhov & Muthén, Reference Asparouhov and Muthén2014). This analysis is similar to multinomial logistic regression and the preferred method for including covariates while simultaneously not allowing covariates to influence class formation (Asparouhov & Muthén, Reference Asparouhov and Muthén2014). For each indicator, the estimated odds ratios (ORs) provide the probability of being in a specific class relative to the reference class.
Results
Trajectories of resilience
First, we estimated the trajectories of resilience among young children involved in CPS. Using several indicators of model fit, interpretability, and parsimony, the 3-class model fit the data best (see Table 2). The BIC and ABIC declined across all models (i.e., from the 1- to 2-class model, from the 2- to 3-class model, etc.); however, the 7-class solution demonstrated convergence issues. Both the 5-class and 6-class models included classes with fewer than 50 cases and thus were not selected as the optimal solution. In comparing the 3-class and 4-class solution, the entropy decreased and there was reduced interpretability and parsimony. Specifically, the fourth class did not seem qualitatively different from existing class solutions in the 3-class model. The four-class solution appeared to reduce the patterns of the previous three classes and created a fourth class that blended the patterns of the other classes. Class membership and item response probability parameter estimates can be found in Table 3. The three developmental trajectories were plotted and labeled according to their change over time (see Figure 1). Approximately 17.4% of young children demonstrated average initial levels of resilience that greatly increased over time, and this group was labeled “increasing resilience.” Specifically, children in the increasing resilience trajectory demonstrated higher levels of resilience across all three developmental domains (i.e., behavioral, language, and cognitive) and across time. A second group was labeled “decreasing resilience” and included 51.5% of young children who demonstrated average levels of resilience initially that declined over time; however, this group of children did demonstrate rebounding levels of behavioral resilience at wave 3. In the decreasing resilience trajectory, children exhibited successively lower levels of language and cognitive resilience and somewhat lowering levels of behavioral resilience across time. The last group of young children initially had low levels of resilience that remained consistently low over time; this group included approximately 31.1% of young children and was labeled “stable, low resilience.” For example, this last trajectory included children who exhibit no behavioral resilience at the latter two waves.
Table 2. Repeated measures latent class analysis fit statistics for trajectories of resilience

Note. The 7-class model had convergence issues.
Table 3. Three-class model of resilience trajectories (n = 1,699)
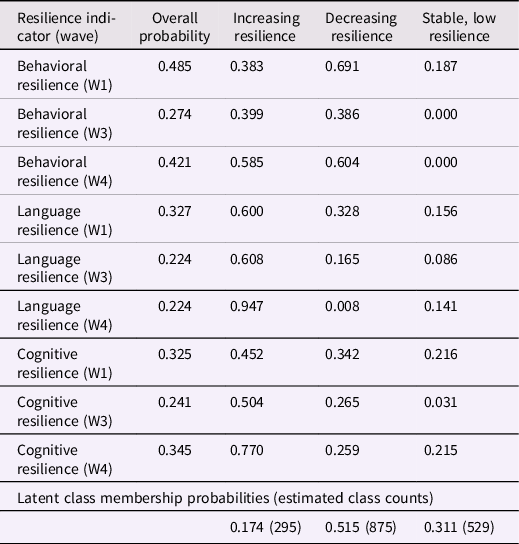
Note. All analyses were weighted with longitudinal sample weights. Item response probabilities are the probabilities of each domain of resilience for the overall sample and within each latent class.

Figure 1. Repeated measures latent class analysis results for young children involved in CPS.
Predictors of resilience trajectories
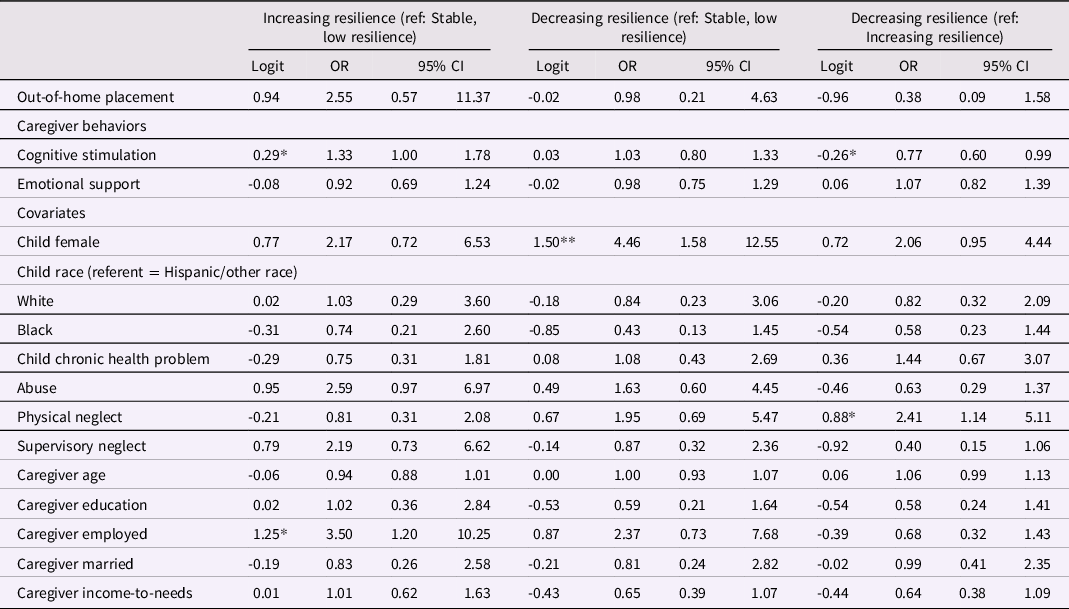
Next, we examined whether out-of-home placement, caregiver behaviors, and covariates were associated with class membership. Table 4 contains all unstandardized logits, ORs, and 95% confidence intervals for the ORs (95% CI). Out-of-home placement at wave 1 was not significantly associated with class membership regardless of the reference trajectory. Similarly, emotional support at wave 1 was not significantly associated with class membership. Higher levels of cognitive stimulation were associated with lower odds of being in the decreasing resilience compared to the increasing resilience class and associated with higher odds of being in the increasing resilience class compared to the stable, low resilience group. In other words, higher levels of cognitive stimulation were related to higher odds of being in the increasing resilience trajectory.
Table 4. Multinomial logistic regression odds ratios (OR) and confidence intervals (CI) for out-of-home placement, caregiver behaviors, and covariates (n = 1,468)
Note.
* p < .05;
** p < .01
Ref = reference group. Caregiver education is high school diploma and higher or not. All predictors are from wave 1.
Turning to the covariates, females were more likely to be in the decreasing resilience class compared to the stable, low resilience class (as seen in Table 4). Children with employed caregivers were more likely to be in the increasing resilience class compared to the stable, low resilience class. Compared to the increasing resilience class, children who experience physical neglect were more likely to be in the decreasing resilience trajectory.
Discussion
Over the past few decades, there has been a notable growth in the number of studies focusing on resilience among children who have experienced child maltreatment (Dubowitz et al., Reference Dubowitz, Thompson, Arria, English, Metzger and Kotch2016; Sattler & Font, Reference Sattler and Font2018; Yoon et al., Reference Yoon, Sattler, Knox and Xin2021). Yet, several important limitations and gaps in prior studies have hindered the field’s ability to advance our scientific understanding of resilience in the context of child maltreatment. That is, most previous studies on resilience either focused on a single domain of resilience, assessed resilience at a single point in time, or focused on adolescents. Thus, little is known about heterogeneity in developmental trajectories of resilience among young children in CPS. This study fills the research gaps by assessing resilience as a multidimensional construct, modeling resilience longitudinally using a person-centered analytic approach (i.e., RMLCA), and focusing on very young children involved with the child welfare system. Furthermore, we examined placement setting as a predictor of resilience trajectories and caregiving behaviors —cognitive stimulation and emotional support— as important protective factors for resilience trajectory group membership.
Using RMLCA, we found three distinct resilience trajectories: the increasing resilience group (17.4%); the stable, low resilience group (31.1%); and the decreasing resilience group (51.5%). The three unique resilience trajectory patterns identified in the study support the idea that resilience is not a fixed trait but rather a mutable, multifaceted construct that changes over time. Interestingly, two groups (i.e., increasing and decreasing resilience) started out with a similar initial score at baseline (Wave 1) but diverged over time. The similarity in resilience at baseline may be attributed to children’s shared recent experience of CPS involvement, which may have influenced their (resilient) functioning that was assessed shortly after exposure to maltreatment. It may also be that there is generally less variation in resilience at younger age and the heterogeneity in resilience becomes more salient as children get older and are exposed to diverse environments and relationships outside their family/home context. However, more research is needed to further clarify and understand these findings.
Our findings are broadly in line with previous studies that used other trajectory approaches (i.e., Growth Mixture Modeling) to investigate social (Oshri et al., Reference Oshri, Topple and Carlson2017), behavioral (Proctor et al., Reference Proctor, Skriner, Roesch and Litrownik2010), or academic (Holmes et al., Reference Holmes, Yoon, Berg, Cage and Perzynski2018) resilience among maltreated children in that similar trajectory patterns (i.e., stable and low, increasing, decreasing) were also observed in these other studies. What is different from previous studies is that the largest portion of our sample showed the decreasing resilience trajectory pattern over time, which contradicts empirical evidence from prior work that resilience increases over time across the life course (Eisman et al., Reference Eisman, Stoddard, Heinze, Caldwell and Zimmerman2015; Norris et al., Reference Norris, Tracy and Galea2009; Werner, Reference Werner1989). The discrepancy in findings may be due to the shorter observation time of resilience (i.e., 36 months) in our study compared to the longer observation period in other studies (i.e., 10 years in Holmes et al., Reference Holmes, Yoon, Berg, Cage and Perzynski2018; 8 years in Proctor et al., Reference Proctor, Skriner, Roesch and Litrownik2010). Alternatively, it may be that our findings point to the extreme vulnerability of young children affected by maltreatment during the first few years of life and suggest that, without proper support systems and intervention, young children in CPS are at risk of decreasing resilience over time.
Among children who demonstrated varying levels and trajectories of resilience across time, more were in the stable, low resilience group (31.1%) than the increasing resilience group (17.4%). One possible explanation for a smaller portion of children demonstrating increasing resilience in our study is that we operationalized resilience as showing competence across multiple domains of development (i.e., behavioral, language, and cognitive functioning). It may be that multi-domain resilience is less common than resilience in a single domain (Dubowitz et al., Reference Dubowitz, Thompson, Arria, English, Metzger and Kotch2016; Sattler & Font, Reference Sattler and Font2018). Put differently, one may show competence and resilience in one area, but experience challenges in other areas of development.
In terms of the predictors of resilience trajectories, we found no evidence that placement setting predicted membership in resilience trajectory groups. The null relationship between placement setting and resilience trajectories falls in line with prior work yielding mixed or null findings of placement setting on children’s long-term development (Berger et al., Reference Berger, Bruch, Johnson, James and Rubin2009). One potential explanation could be that initial placement setting is not most influential but rather what happens after the initial placement (e.g., safety, placement stability, permanency) has more direct impact on children’s outcomes, including resilience development (Brown et al., Reference Brown, Leveille, Gough, Flynn, Dudding and Barber2006; Rubin et al., Reference Rubin, Alessandrini, Feudtner, Mandell, Localio and Hadley2004). Similarly, it might be that the placement setting is not as important as other factors such as the types of caregiving behaviors shown by the primary caregivers. For example, a study that examined adolescent resilience in the context of child maltreatment revealed that the type of placement (e.g., foster care, residential care, community care) was not associated with youth resilience whereas other demographic and family factors, such as being a girl, older, and accepted by the father, contributed to resilience (Davidson-Arad & Navaro-Bitton, Reference Davidson-Arad and Navaro-Bitton2015).
With regard to caregiving behaviors, we found that cognitive stimulation, but not parental emotional support, was predictive of resilience trajectories. Emotional support and emotional responsiveness have been linked to positive social behavioral outcomes among maltreated children in prior studies (Harden & Whittaker, Reference Harden and Whittaker2011; Saitadze, 2021) and positive cognitive outcomes in maltreated infants (Sattler & Font, Reference Sattler and Font2018), yet the same positive effects were not observed in our study. Given the other studies that reported positive effects of emotional support assessed resilience among older children (i.e., kindergarten or later), it may be that emotional support has more salient influences at later developmental periods than during the infancy and toddlerhood period. It is noteworthy that the majority of our sample experienced child neglect (i.e., 65% experienced physical neglect, 79% experienced supervisory neglect). Children who experience child neglect are at a higher risk of not receiving adequate level of cognitive stimulation that is necessary to meet their developmental needs (Skuse, Reference Skuse1989). Further, ample evidence suggests that child neglect, as well as the lack of cognitive stimulation, can have particularly detrimental impact on child growth and development during infancy and toddlerhood (Cates et al., Reference Cates, Dreyer, Berkule, White, Arevalo and Mendelsohn2012; English et al., Reference English, Thompson, Graham and Briggs2005b; Strathearn et al., Reference Strathearn, Gray, O’Callaghan and Wood2001). Therefore, cognitive stimulation might have played an especially salient role in this sample of very young children, many of whom experienced child neglect. Another possibility is that our sample included both parental and non-parental caregivers, whereas other studies mostly focused on parents. It may be that the influence of emotional support varies across caregivers (Sattler & Font, Reference Sattler and Font2018). However, further research is needed to understand the role of emotional support/responsiveness in resilience during early childhood.
In contrast to the null findings of emotional support on resilience trajectories, we found that higher levels of cognitive stimulation predicted membership in the increasing resilience group compared to the stable, low resilience, and decreasing resilience groups. This finding is consistent with a robust body of research indicating caregivers’ cognitively stimulating behavior as an important factor related to resilience development among children with a history of child maltreatment (Holmes et al., Reference Holmes, Yoon, Berg, Cage and Perzynski2018; Jaffee, Reference Jaffee2007; Sattler & Font, Reference Sattler and Font2018). Similar to previous work, our findings demonstrate that the benefit of cognitive stimulation starts even at a very early developmental stage (i.e., infancy, toddlerhood) and that it has enduring and lagged effects on resilience development over time. One potential alternative explanation is our resilience construct was based on two more cognitive domains and one social domain. Therefore, cognitive stimulation may be more influential when assessing resilience this way. Future research should expand on the current study to consider how specific parenting behaviors differentially impact domains of resilience.
Of the covariates, physical neglect was found to be significant predictors of resilience trajectories. Specifically, children who experienced physical neglect were more likely to be in the decreasing resilience, compared to the increasing resilience class. Drawing from Belsky’s differential susceptibility hypothesis (Belsky et al., Reference Belsky, Bakermans-Kranenburg and Van IJzendoorn2007) which posits that children are differently affected (“both for better and for worse”) by their environments and experiences, early childhood neglect may have had varying levels and different patterns of influence on the development of resilience for children. Relatedly, studies suggest that childhood trauma can contribute to both risk and resilience (Oldehinkel et al., Reference Oldehinkel, Ormel, Verhulst and Nederhof2014; Samuels & Pryce, Reference Samuels and Pryce2008). Nevertheless, it remains unclear how different maltreatment types are linked to different resilience trajectories and why maltreatment is associated with increased resilience for some children and decreased resilience for others, warranting further investigation.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, despite the use of longitudinal data, the nonexperimental study design limits our ability to make any causal inferences between study variables. Second, given that our study sample included children involved in CPS due to child maltreatment, the study results may not be generalizable to children who have not been involved with the child welfare system or children with other risk experiences. Third, we were only able to measure resilience at three time points over a 36-month period, with an interval of approximately 18 months. Resilience is a dynamic process, and its fluctuation across time may have been better captured in shorter intervals between assessment time points. Future research may benefit from assessing the changes in resilience for a longer period of time, with shorter time intervals.
Conclusions and implications
Despite these limitations, the current study has multiple strengths and offer significant implications for research, practice, and policy. First, this study makes several research contributions. This study is among the first to longitudinally examine heterogeneity in resilience while also accounting for the multidimensional nature of resilience among young children involved in CPS. The study’s focus on very young children involved in CPS, with a resilience lens, is another unique strength, given that most prior resilience studies focused on school-aged children or adolescents. The RMLCA approach applied in the current study successfully identified three distinct resilience trajectory groups, demonstrating the appropriateness and utility of longitudinal person-centered analytical approaches in studying resilience among CPS-involved children. However, in using this approach we were not able to model how resilience in one domain enables resilience in another across time. This is in part due to methodological limitations. Future research should continue to consider utilizing longitudinal, person-centered modeling as well as multidimensional measures to explore various forms and developmental patterns of resilience in this population. At the practice level, our finding of caregivers’ cognitively stimulating behavior predicting membership in the increasing resilience group informs the development of intervention strategies for young children in the CPS system. Practitioners working with young children with a history of maltreatment should understand the role of early cognitive stimulation in children’s resilience development over time. Interventions that teach parents to create a cognitively stimulating environment for their children may maintain or enhance resilience among children. At the policy level, more funding should be allocated to support programs and services targeting the well-being of very young children involved in CPS, considering that over a quarter of maltreatment victims involve children under 2 years old and that over a half of these children are at risk of experiencing decreasing resilience over time. More targeted and intensive interventions are needed to ensure the sustained well-being and resilience development of young children involved in the child welfare system.
Acknowledgments
This document includes data from the National Survey on Child and Adolescent Well-Being, which was developed under contract with the Administration on Children, Youth, and Families, U.S. Department of Health and Human Services (ACYF/DHHS). The data were provided by the National Data Archive on Child Abuse and Neglect (NDACAN).
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
None.






 Open access
Open access