Introduction
Selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), 5-HT1A receptor modulators, mixed dopamine serotonin receptor antagonists, and medications such as pregabalin/gabapentin are used to reduce anxiety in adults with anxiety disorders,Reference Strawn, Geracioti, Rajdev, Clemenza and Levine 1 although some patients may not fully respond to these treatments. As such, benzodiazepines—once the first-line psychopharmacologic intervention for adults with anxiety disorders—continue to have a role in treating anxiety, particularly in patients with partial response to other medications.Reference Goddard, Brouette, Almai, Jetty, Woods and Charney 2 While they are used more selectively in current practice, benzodiazepines remain one of the most commonly prescribed classes of medication in the United States. Benzodiazepine prescribing has increased, primarily among nonpsychiatric clinicians.Reference Agarwal and Landon 3 Moreover, while benzodiazepines are no longer the first-line treatment for anxiety disorders, they remain a viable option for patients with treatment refractory anxiety and as adjunctive agents,Reference Pollack, Van Ameringen and Simon 4 , Reference Pollack, Simon and Worthington 5 and continue to be used for insomnia, muscle relaxation, neuromotor spasticity, and sedation.
Previous meta-analyses reveal that benzodiazepines are more effective than placebo for patients with anxiety disorders, including generalized and social anxiety disorders as well as panic disorder.Reference Kong, Deng and Wan 6 , Reference Slee, Nazareth, Bondaronek, Liu, Cheng and Freemantle 7 However, most prior meta-analyses have examined only endpoint response and were unable to address heterogeneity in design and treatment response. Two Cochrane Reviews of benzodiazepines in adults with panic disorder found benzodiazepines were superior to placeboReference Breilmann, Girlanda and Guaiana 8 and observed similar response rates for benzodiazepines and antidepressants.Reference Bighelli, Trespidi and Castellazzi 9 In the first of these meta-analyses, which compared benzodiazepines to placebo, the risk ratio for improvement was 1.65 (95% Confidence Interval [CI]: 1.39-1.96) corresponding to a number needed to treat of 4 (95% CI: 3-7). However, these meta-analyses were unable to address variation in dosing or the time course of response, which may produce differences in response and tolerability in addition to altering response trajectory.
The last three decades saw an accumulation of knowledge regarding the pharmacokinetics and pharmacodynamics of benzodiazepines, which have shed light on their differential tolerability and efficacy. Benzodiazepines are positive allosteric modulators at the
 $ \gamma $
-amino butyric acid (GABAA) receptor,Reference Griffin, Kaye, Rivera Bueno and Kaye
10 a ligand-gated chloride-selective ion channel,Reference Nelson and Chouinard
11 although, they differ in their affinity for GABAA. All benzodiazepines (except clorazepate) are absorbed completely, and all have high lipid-water distribution coefficients in their nonionized form. Patterns of plasma benzodiazepine concentrations are consistent with two-compartment models, although some studies suggest that three-compartment models more appropriately describe the most lipophilic benzodiazepines. As lipophilicity determines redistribution, it is one of the most important determinants of the duration of benzodiazepine effect.Reference Dettli
12 Thus, while differences in the duration of effect can relate to the presence of active metabolites, lipophilicity is likely more important given that benzodiazepine activity is terminated by redistribution.
$ \gamma $
-amino butyric acid (GABAA) receptor,Reference Griffin, Kaye, Rivera Bueno and Kaye
10 a ligand-gated chloride-selective ion channel,Reference Nelson and Chouinard
11 although, they differ in their affinity for GABAA. All benzodiazepines (except clorazepate) are absorbed completely, and all have high lipid-water distribution coefficients in their nonionized form. Patterns of plasma benzodiazepine concentrations are consistent with two-compartment models, although some studies suggest that three-compartment models more appropriately describe the most lipophilic benzodiazepines. As lipophilicity determines redistribution, it is one of the most important determinants of the duration of benzodiazepine effect.Reference Dettli
12 Thus, while differences in the duration of effect can relate to the presence of active metabolites, lipophilicity is likely more important given that benzodiazepine activity is terminated by redistribution.
Pharmacologic differences in benzodiazepines are hypothesized to produce different clinical profiles and may predict differences in efficacy, tolerability, and abuse potentialReference Griffin, Kaye, Rivera Bueno and Kaye 10; however, explorations of the relationship between pharmacologic characteristics and clinical efficacy are rare. In one prior meta-analysis, dose (in diazepam equivalents) or type of benzodiazepine were not significantly associated with endpoint response, although these analyses did not address the heterogeneity of treatment response or the trajectory of response.
Benzodiazepines effectively reduce anxiety in adults with anxiety disorders; however, the corpus of randomized controlled trials is heterogeneous. Medication, medication dosage, duration, and placebo response vary considerably across studies. Additionally, the few meta-analyses of benzodiazepines in anxiety disorders have focused on endpoint response and have been unable to meta-analytically examine the trajectory of treatment response.Reference Gale, Glue, Guaiana, Coverdale, McMurdo and Wilkinson 13 , Reference Gupta, Bhattacharya and Fartieen 14
Aggregating time course and symptom severity data from trials of benzodiazepines in adults with anxiety disorders allows the overall time course of treatment and placebo response and the impact of selected medication-specific variables to be evaluated with greater statistical power than can be accomplished in individual trials. With these considerations in mind, we conducted a Bayesian hierarchical modeling (BHM) meta-analysis of benzodiazepine and placebo response in randomized, placebo-controlled trials for the short-term treatment of generalized, social and/or separation anxiety disorders as well as panic disorder in adults. Specifically, we sought to: (1) examine the temporal course of benzodiazepine and placebo response; (2) compare the trajectory and magnitude of response as a function of pharmacologic characteristics; (3) determine if standardized dose predicts treatment response; and (4) compare the trajectory of response across benzodiazepines. We hypothesized that treatment response would be logarithmic as is the case for pharmacologic interventions (eg, SSRIs and SNRIs) in anxiety disorders and major depressive disorder and that higher doses and greater lipophilicity and greater potency would be associated with faster and greater improvement.
Methods
Search strategy
All meta-analytic methods and sensitivity analyses were specified before conducting the meta-analysis proper. The studies included were obtained through an electronic search of English language articles in PubMed (1966 through January 2021) in addition to the Cochrane Database as well as the government clinical trials registry, www.clinicaltrials.gov using the search strategy: (Benzo* OR alprazolam OR clonazepam OR clobazam OR lorazepam OR diazepam OR bromazepam OR chlordiazepoxide OR chlorazepate OR clorazepam OR estazolam OR flurazepam OR quazepam OR temazepam OR triazolam OR oxazepam) AND (anxiety OR anxious OR anxiolytic OR panic* OR panic disorder OR generalized anxiety OR generalized anxiety disorder OR GAD OR social anxiety disorder OR social phobia OR SoP) AND (placebo) NOT (“systemic review” OR “systematic review” OR review OR meta-analysis OR meta-analysis OR editorial OR case report OR letter OR mice OR zebrafish OR rat OR dog OR insomnia OR sleep OR dental OR delirium OR memory OR seizure OR withdrawal). The results of the search were then manually limited to randomized, placebo-controlled trials. The references of all eligible trials were searched for additional clinical trials.
Criteria for inclusion of studies
Studies were included if they were prospective, randomized, parallel group, placebo-controlled trials that evaluated the efficacy of a benzodiazepine in the treatment of social, generalized and/or separation anxiety disorder or panic disorder or a DSM-IV or DSM-III-R forerunner of these disorders in adults, and used the Hamilton Anxiety Rating Scale,Reference Hamilton 15 a validated rating scale to measure the severity of the anxiety symptoms. Clinical trials were excluded if they met any of the following criteria: included children and adolescents (age < 18 years); utilized a cross-over design; did not study a benzodiazepine; were not randomized; were not placebo-controlled; provided adjunctive psychotherapy or adjunctive benzodiazepine to active or control group; or included <10 patients per treatment group.
Data extraction
Data were extracted into an Excel (Microsoft, Redmond, WA) spreadsheet by two physician authors (J.N.S. and J.R.S.). Additional data related to the methods, demographics, dosing, duration of the trial, and other relevant aspects and results of the studies were collected. Consistent with a prior meta-analysis of the efficacy and tolerability of SSRIs and SNRIs,Reference Strawn, Welge, Wehry, Keeshin and Rynn 16 the outcome measurements selected from each included clinical trial was the mean improvement in the benzodiazepine-treated and placebo-treated groups. This mean improvement was determined for the clinical rating scale measuring anxiety symptom severity at each reported time point for the Hamilton Anxiety Rating Scale.
Statistical methods
The primary outcome for these analyses was the change in HAM-A total score from baseline to endpoint. A set of treatment response models (linear, exponential, logarithmic, and quadratic) was developed in which the relative treatment effects were modeled using a Bayesian inferential approach with parameters estimated using Markov chain Monte Carlo (MCMC) simulation. The best fitting model was selected based on posterior predictive trajectories, Akaike and Bayesian Information Criteria (AIC and BIC), as previously described.Reference Mills and Prasad 17
For individual studies, the endpoint was typically week 4, 6, or 8, except in four studies with 10 and 12-week duration (Figure 1A). The benzodiazepine dose was converted (or imputed and converted) to lorazepam equivalents. Based on lorazepam equivalents,Reference Chouinard, Lefko-Singh and Teboul
18 dose was categorized as low (
 $ < $
3 lorazepam equivalents/day), medium (3 to <6 lorazepam equivalents/day) or high (
$ < $
3 lorazepam equivalents/day), medium (3 to <6 lorazepam equivalents/day) or high (
 $ \ge $
6 lorazepam equivalents/day). The difference in change scores between each medication and its corresponding placebo arm was computed, and treatment response was modeled for the standardized change in HAM-A. Specifically, the ratio of anxiety symptom severity score at each week to the initial anxiety symptom score was employed with the standard deviation in weekly anxiety score normalized using the initial anxiety score to allow for heterogeneity in variance across studies, as previously described.Reference Strawn, Mills, Sauley and Welge
19
$ \ge $
6 lorazepam equivalents/day). The difference in change scores between each medication and its corresponding placebo arm was computed, and treatment response was modeled for the standardized change in HAM-A. Specifically, the ratio of anxiety symptom severity score at each week to the initial anxiety symptom score was employed with the standard deviation in weekly anxiety score normalized using the initial anxiety score to allow for heterogeneity in variance across studies, as previously described.Reference Strawn, Mills, Sauley and Welge
19

Figure 1. Response in adults with anxiety disorders treated with benzodiazepines and placebo. The number of studies reporting data at each week is shown in (A). The change in anxiety symptom severity for patients who received benzodiazepine (blue) and those who received placebo (red) is each study is shown in (B). Change in anxiety symptoms was logarithmic in the best fitting model for both active medication and placebo (C) and this change in anxiety symptoms was similar in an unrestricted response model (D) as was the standardized benzodiazepine-placebo difference (E). Standardized medication-placebo difference differed by dose (F) and was superior for clonazepam compared to other benzodiazepines (G). Dotted lines reflect the 95% credible interval.
Change in anxiety symptom severity was evaluated as a function of time, standardized dose, and lipophilicity, using a BHM with individual (patient level) logarithmic trajectories to capture unobserved heterogeneity. Posterior estimates were obtained from MCMC simulations as previously described.Reference Strawn, Mills and Cornwall 20 , Reference Suresh, Mills, Croarkin and Strawn 21 For comparison of benzodiazepine and placebo response by week, posterior distributions of the weekly difference in means were obtained from a time indicator “random effects” BHM. Differences in means, credible intervals, and so forth were determined from the posterior MCMC samples. The logarithmic trajectory BHM was specified as,
 $$ \begin{array}{c}\Delta {h}_{it} = \hskip1.5pt {\delta}_i\log {t}_i+{\beta}_1\mathrm{low}\_\mathrm{dos}{\mathrm{e}}_{it}+{\beta}_2\mathrm{high}\_\mathrm{dos}{\mathrm{e}}_{it}\\ {}\hskip-3.2pc + {\beta}_3\mathrm{lipophilicit}{\mathrm{y}}_{it}+{\varepsilon}_{it},\end{array} $$
$$ \begin{array}{c}\Delta {h}_{it} = \hskip1.5pt {\delta}_i\log {t}_i+{\beta}_1\mathrm{low}\_\mathrm{dos}{\mathrm{e}}_{it}+{\beta}_2\mathrm{high}\_\mathrm{dos}{\mathrm{e}}_{it}\\ {}\hskip-3.2pc + {\beta}_3\mathrm{lipophilicit}{\mathrm{y}}_{it}+{\varepsilon}_{it},\end{array} $$
where
 $ \Delta {h}_{it}\hskip1.5pt = $
change in HAM-A score from baseline for study
$ \Delta {h}_{it}\hskip1.5pt = $
change in HAM-A score from baseline for study
 $ i $
at time period,
$ i $
at time period,
 $ {t}_i $
(week),
$ {t}_i $
(week),
 $ \mathrm{low}\_\mathrm{dos}{\mathrm{e}}_{it}\hskip1.5pt =\hskip1.5pt 1\;\mathrm{if}\ \mathrm{dose}\hskip1.5pt \le 3,0 $
otherwise,
$ \mathrm{low}\_\mathrm{dos}{\mathrm{e}}_{it}\hskip1.5pt =\hskip1.5pt 1\;\mathrm{if}\ \mathrm{dose}\hskip1.5pt \le 3,0 $
otherwise,
 $ \mathrm{high}\_\mathrm{dos}{\mathrm{e}}_{it}\hskip1.5pt =\hskip1.5pt 1\;\mathrm{if}\ \mathrm{dose}>6,0 $
otherwise,
$ \mathrm{high}\_\mathrm{dos}{\mathrm{e}}_{it}\hskip1.5pt =\hskip1.5pt 1\;\mathrm{if}\ \mathrm{dose}>6,0 $
otherwise,
 $ {\varepsilon}_{it}\sim N\left(0,{\sigma}_i^2\right) $
. Two specifications were considered for the hierarchical prior distributions, each with
$ {\varepsilon}_{it}\sim N\left(0,{\sigma}_i^2\right) $
. Two specifications were considered for the hierarchical prior distributions, each with
 $ {\delta}_i\sim N\left(\delta, \tau \right),\delta \sim U\left(-\mathrm{2.0,1.0}\right),\tau \sim U\left(0.001,5.0\right),\beta \sim N\left(0,1\right), $
where
$ {\delta}_i\sim N\left(\delta, \tau \right),\delta \sim U\left(-\mathrm{2.0,1.0}\right),\tau \sim U\left(0.001,5.0\right),\beta \sim N\left(0,1\right), $
where
 $ N $
represents the normal distribution and
$ N $
represents the normal distribution and
 $ U $
the uniform. For the homoskedastic specification, with
$ U $
the uniform. For the homoskedastic specification, with
 $ {\sigma}_i\hskip1.5pt =\hskip1.5pt \sigma, \sigma \sim U\left(0.001,5.0\right) $
, and for the heteroskedastic specification,
$ {\sigma}_i\hskip1.5pt =\hskip1.5pt \sigma, \sigma \sim U\left(0.001,5.0\right) $
, and for the heteroskedastic specification,
 $ {\sigma}_i^2\sim IG\left(\left({n}_i-1\right)/2,s\left({n}_i-1\right)/2\right),s\sim U\left(0.001,12.0\right), $
with
$ {\sigma}_i^2\sim IG\left(\left({n}_i-1\right)/2,s\left({n}_i-1\right)/2\right),s\sim U\left(0.001,12.0\right), $
with
 $ {n}_i\hskip1.5pt =\hskip1.5pt $
number of observations (time periods) for study
$ {n}_i\hskip1.5pt =\hskip1.5pt $
number of observations (time periods) for study
 $ i $
, and
$ i $
, and
 $ IG $
represents the inverted-gamma distribution. All prior parameter values were validated to ensure the resulting priors were uninformative (ie, relatively flat over the support of the likelihood with nonnegligible probability). The time indicator BHM was specified as,
$ IG $
represents the inverted-gamma distribution. All prior parameter values were validated to ensure the resulting priors were uninformative (ie, relatively flat over the support of the likelihood with nonnegligible probability). The time indicator BHM was specified as,
 $$ \begin{array}{c}\Delta {h}_{it}\hskip2.50pt =\hskip3.50pt \alpha +{\delta}_t{I}_{it}+{\beta}_1\mathrm{low}\_\mathrm{dos}{\mathrm{e}}_{it}+{\beta}_2\mathrm{high}\_\mathrm{dos}{\mathrm{e}}_{it}\\ {}\hskip-3.5pc + {\beta}_3\mathrm{lipophilicit}{\mathrm{y}}_{it}+{\varepsilon}_{it},\end{array} $$
$$ \begin{array}{c}\Delta {h}_{it}\hskip2.50pt =\hskip3.50pt \alpha +{\delta}_t{I}_{it}+{\beta}_1\mathrm{low}\_\mathrm{dos}{\mathrm{e}}_{it}+{\beta}_2\mathrm{high}\_\mathrm{dos}{\mathrm{e}}_{it}\\ {}\hskip-3.5pc + {\beta}_3\mathrm{lipophilicit}{\mathrm{y}}_{it}+{\varepsilon}_{it},\end{array} $$
where
 $ {I}_{it} $
is a vector of time indicators,
$ {I}_{it} $
is a vector of time indicators,
 $ {I}_{it}\hskip1.5pt =\hskip1.5pt \Big[{I}_{i1t}{I}_{i2t} $
…
$ {I}_{it}\hskip1.5pt =\hskip1.5pt \Big[{I}_{i1t}{I}_{i2t} $
…
 $ {I}_{i8t}\Big] $
with
$ {I}_{i8t}\Big] $
with
 $ {I}_{ikt}\hskip1.5pt =\hskip1.5pt 1 $
if
$ {I}_{ikt}\hskip1.5pt =\hskip1.5pt 1 $
if
 $ t\hskip1.5pt =\hskip1.5pt k,0 $
otherwise (ie, time fixed effects),
$ t\hskip1.5pt =\hskip1.5pt k,0 $
otherwise (ie, time fixed effects),
 $ {\varepsilon}_{it}\sim N\left(0,{\sigma}^2\right) $
, and priors
$ {\varepsilon}_{it}\sim N\left(0,{\sigma}^2\right) $
, and priors
 $ {\delta}_i\sim N\left(\mu, 1\right),\mu \sim TN\left(0,2,-3.0,2.0\right),\alpha \sim N\left(0,2\right),\beta \sim N\left(0,1\right),{\sigma}^2\sim U\left(0.001,10.0\right), $
where
$ {\delta}_i\sim N\left(\mu, 1\right),\mu \sim TN\left(0,2,-3.0,2.0\right),\alpha \sim N\left(0,2\right),\beta \sim N\left(0,1\right),{\sigma}^2\sim U\left(0.001,10.0\right), $
where
 $ TN $
is a truncated normal distribution with bounds −3 and 2 (imposed solely to improve computational stability and performance of the MCMC algorithm). A post hoc examination of dose and dropout, a crude proxy for tolerability, was also conducted. From the BHM posterior simulation samples, we determined the relative risk for dropout in benzodiazepine-treated patients with regard to dose (reported as relative risk with the 95% credible interval [CrI]).
$ TN $
is a truncated normal distribution with bounds −3 and 2 (imposed solely to improve computational stability and performance of the MCMC algorithm). A post hoc examination of dose and dropout, a crude proxy for tolerability, was also conducted. From the BHM posterior simulation samples, we determined the relative risk for dropout in benzodiazepine-treated patients with regard to dose (reported as relative risk with the 95% credible interval [CrI]).
Statistical heterogeneity was quantified with standard measures: the Q statistic (ie, weighted sum of squared differences between individual study effects and the pooled effect across trials) and
 $ {I}^2 $
(ie, heterogeneity-related variance rather than variance attributed to sampling error).Reference Suresh, Mills, Croarkin and Strawn
22 To further and more comprehensively assess heterogeneity, we examined: (1) individual trend models, (2) heteroskedastic error models, (3) time indicator random effects specification, and (4) the robustness of each response model to alternate functional forms.
$ {I}^2 $
(ie, heterogeneity-related variance rather than variance attributed to sampling error).Reference Suresh, Mills, Croarkin and Strawn
22 To further and more comprehensively assess heterogeneity, we examined: (1) individual trend models, (2) heteroskedastic error models, (3) time indicator random effects specification, and (4) the robustness of each response model to alternate functional forms.
Analyses were conducted in Julia (version: 1.6.1).Reference Higgins, Thompson, Deeks and Altman 23 The BHMs were each estimated using 5000 iterations of the “No U-Turn” Hamiltonian Monte Carlo sampler in Turing.jl.Reference Bezanson, Edelman, Karpinski and Shah 24 For all analyses, Bayesian posterior tail-area equivalents of a frequentist P-value for evidence against the null hypothesis (H 0) were determined and considered statistically significant at the P < .05 level. Means are represented ± their standard deviations (SD) and precision is expressed as 95% CrIs.
Results
Selection of studies and study characteristics
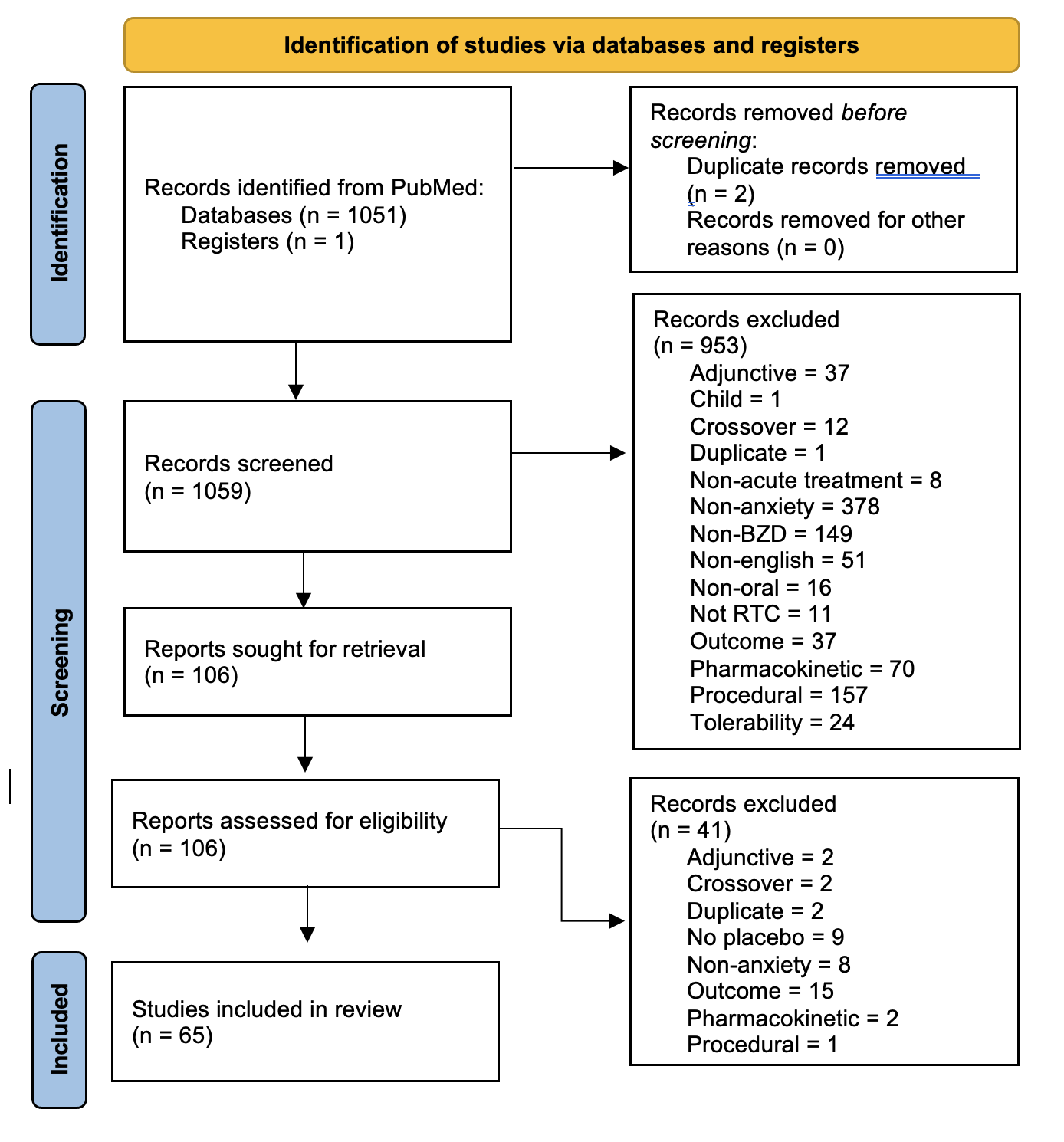
A total of 1060 reports were identified that were potentially eligible for inclusion in this meta-analysis of which 106 were retrieved in full text. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagramReference Ge, Xu and Ghahramani
25 illustrating the selection procedure—which yielded 69 studies (65 after those with missing data were excluded)—is shown in Figure 1B Supplemental Figure 1. Seven different benzodiazepines were evaluated in these randomized controlled trials which included 73 arms (Table 1) with a mean duration of 5.3
 $ \pm $
1.9 weeks. In total, 3692 patients were treated with a benzodiazepine and 3418 received placebo and all studies were conducted in the outpatient setting. Sixteen trials focused on patients with panic disorder and 47 trials included GAD while six trials included patients with social anxiety disorder/social phobia, overanxious disorder/anxiety neurosis. Additional trial characteristics are shown in Table 1 and several trials included multiple arms.
$ \pm $
1.9 weeks. In total, 3692 patients were treated with a benzodiazepine and 3418 received placebo and all studies were conducted in the outpatient setting. Sixteen trials focused on patients with panic disorder and 47 trials included GAD while six trials included patients with social anxiety disorder/social phobia, overanxious disorder/anxiety neurosis. Additional trial characteristics are shown in Table 1 and several trials included multiple arms.
Table 1. Study, Patient, and Treatment Characteristics of Included Randomized Controlled Trials of Selective Benzodiazepines in Adults with Panic Disorder, Generalized/Social Anxiety Disorders

Note:
 $ \overline{X} $
, mean.
$ \overline{X} $
, mean.
Time course of benzodiazepine response compared to placebo
Based on AIC, BIC, and posterior predictive accuracy, the best models for benzodiazepine treatment response were linear-logarithmic model for trajectory of improvement (Figure 1C,E) and a time indicator random effects model to evaluate week by week comparisons of improvement (Figure 1D). These models both indicated that benzodiazepine-related improvement in anxiety compared to placebo was greatest initially; this rate of improvement decreased over successive weeks. Statistically significant standardized benzodiazepine-placebo differences (δ) emerged early during treatment (δ week 1 = −0.218, 95% credible interval [CrI]: −0.263 to −0.173, P < .001, Figure 1C,D and Table 2) within 1 week of beginning treatment and persisted through week 8 (δ week 8 = −0.158, 95% CrI: −0.232 to −0.086, P < .001, Figure 1E and Table 2). More than 80% of the expected improvement by week 8 emerged by week 4 (Figure 1C,D).
Table 2. Benzodiazepine and Placebo Response in Adults with Anxiety Disorders

Note: Negative values reflect improvement.
Pharmacologic predictors of response trajectory
Lipophilicity was significantly associated with benzodiazepine response (trend interaction coefficient
 $ \beta $
= 0.029
$ \beta $
= 0.029
 $ \pm $
0.013, CrI: 0.004-0.053, P = .023) suggesting that when correcting for dose and potency, benzodiazepines with greater lipophilicity produce smaller improvement and slower improvement. Additionally, potency—when correcting for dose—was not significantly associated with response trajectory.
$ \pm $
0.013, CrI: 0.004-0.053, P = .023) suggesting that when correcting for dose and potency, benzodiazepines with greater lipophilicity produce smaller improvement and slower improvement. Additionally, potency—when correcting for dose—was not significantly associated with response trajectory.
Time course of placebo response
In these studies, placebo response—like benzodiazepine response—emerged early in the course of treatment (δ week 1 = −0.139, 95% credible interval [CrI]: −0.179 to −0.097, P < .001, Figure 1C and Table 2). Additionally, by week 4, placebo response plateaued. Approximately 75% of the expected improvement by week 8 emerged by week 4 (Figure 1C,D). Placebo response plateaued at week 4 at significantly less improvement than BZD response (Figure 1).
Effect of benzodiazepine dose on treatment response and dropout
Response, over time, was superior for low dose (<3 mg/day in lorazepam equivalents) compared to medium dose (
 $ \beta \hskip1.5pt =\hskip1.5pt $
−0.054
$ \beta \hskip1.5pt =\hskip1.5pt $
−0.054
 $ \pm $
0.026, CrI: 0.108 to −0.003; P = .042) and patients who received high dose benzodiazepines (>6 mg/day) had less improvement compared to patients who received medium doses of benzodiazepines (
$ \pm $
0.026, CrI: 0.108 to −0.003; P = .042) and patients who received high dose benzodiazepines (>6 mg/day) had less improvement compared to patients who received medium doses of benzodiazepines (
 $ \beta $
= 0.094
$ \beta $
= 0.094
 $ \pm $
0.032, CrI: 0.031-0.158, P = .001) (Figure 1F). Additionally, dropout rates at 4 weeks (modal endpoint), were 14.07% for all benzodiazepine-treated patients, 18.35% for those receiving low dose, 10.04% in those receiving medium dose, and 7.00% in those receiving high doses. The probability of dropout was significantly greater for low dose treatment compared to high dose (mean difference in risk 0.11, P < .001) and was significantly greater for low dose compared to medium dose (mean difference in risk 0.08, P < .001) and did not differ between medium and high dose (mean difference in risk 0.03, P = .10).
$ \pm $
0.032, CrI: 0.031-0.158, P = .001) (Figure 1F). Additionally, dropout rates at 4 weeks (modal endpoint), were 14.07% for all benzodiazepine-treated patients, 18.35% for those receiving low dose, 10.04% in those receiving medium dose, and 7.00% in those receiving high doses. The probability of dropout was significantly greater for low dose treatment compared to high dose (mean difference in risk 0.11, P < .001) and was significantly greater for low dose compared to medium dose (mean difference in risk 0.08, P < .001) and did not differ between medium and high dose (mean difference in risk 0.03, P = .10).
Comparisons among benzodiazepines
Relative to the reference benzodiazepine (lorazepam), clonazepam (
 $ \beta \hskip1.5pt =\hskip1.5pt $
−0.217
$ \beta \hskip1.5pt =\hskip1.5pt $
−0.217
 $ \pm $
0.95, P = .021) had a greater trajectory/magnitude of response (other specific benzodiazepines did not statistically differ from lorazepam) (Figure 1G and Table 3).
$ \pm $
0.95, P = .021) had a greater trajectory/magnitude of response (other specific benzodiazepines did not statistically differ from lorazepam) (Figure 1G and Table 3).
Table 3. Differences in Benzodiazepine Response Relative to Lorazepam

Note: Negative values reflect improvement. δ, standardized medication-placebo trajectory difference. Bold refers to findings that are statistically significant at the p<0.05.
Heterogeneity
Heterogeneity measures for response in benzodiazepine studies were as follows: Q = 26.52 (P = .696), I 2 = 0.0. For panic disorder studies of benzodiazepines, Q = 20.20 (P = .027), I 2 = 50.5, while for GAD studies of benzodiazepines, Q = 5.43 (P = .996), I 2 = 0.
Single trend and heteroskedastic error models produced qualitatively similar results to the individual trends model used for the primary analyses. Considering the one trend, individual trends and heteroskedastic error models, the mean trend coefficient estimate ranged from −0.11 to −0.10. The low dose coefficient was approximately −0.05 in all three models and the high dose coefficient ranged from 0.07 to 0.09, while the coefficient for lipophilicity ranged from 0.02 to 0.03. The R 2 for all three models was approximately 0.22. The model that included a time indicator random effects specification (Figure 1D) produced similar results for both placebo and benzodiazepines compared to the individual trend model (Figure 1C). Based on AIC, BIC, and posterior predictive trajectories, alternate functional forms (linear, log-linear, and quadratic) of benzodiazepine response were less robust in terms of predictive performance compared to the individual trends, linear-log model used in the analysis.
Discussion
This meta-analysis of randomized, double-blind, placebo-controlled trials of benzodiazepines in adults with anxiety disorders: (1) reveals a logarithmic response model; (2) highlights early treatment-related improvement in anxiety; (3) describes a greater trajectory and magnitude of response for low dose vs high dose; and (4) suggests that less lipophilic benzodiazepines produce greater and faster improvement. The implications of these findings in terms of the role benzodiazepines in treating anxiety disorders as well as the selection and dosing of benzodiazepines warrant additional discussion.
This meta-analysis is the first to demonstrate that benzodiazepines decrease anxiety very early in the course of treatment, although this is certainly consistent with clinical experience. This rapid reduction in anxiety symptoms described herein has important treatment implications. Traditional psychotherapeutic and SSRI/SNRI-based treatments often take weeks to produce improvement which results in a protracted period of persistent symptoms for many patients. That benzodiazepines may have a role in the initial management of anxiety as other treatments are initiated is consistent with several studies of adults with anxiety disorders in which faster improvement has been observed when adjunctive benzodiazepines are added to SSRIs.Reference Pollack, Van Ameringen and Simon 4 , Reference Pollack, Simon and Worthington 5 Additionally, this meta-analysis replicates and extends findings from prior meta-analyses of benzodiazepines in anxiety disorders.Reference Breilmann, Girlanda and Guaiana 8 , Reference Page, McKenzie and Bossuyt 26 , Reference Gale, Herbison, Glue, Coverdale and Guaiana 27 This reminder of the efficacy of benzodiazepines is important considering recent commentaries suggesting that “the risks of benzodiazepines have been overestimated while the benefits minimized”Reference Tibrewal, Looi, Allison and Bastiampillai 28 which could result in undertreating, particularly in those patients who do not have contraindications or those with anxiety disorders that are only partially responsive to traditional treatments. That said, while benzodiazepines act rapidly and are efficacious, they—like any other medication—should be used only after considering the relative benefit to risk ratio and considering the patient’s history of substance use, age, fall, and fracture risk.Reference Hirschtritt, Olfson and Kroenke 29
Dose is an important determinant of benzodiazepine response; however, the relationship between dose and response is nuanced. Lower benzodiazepine doses produce the fastest improvement compared to doses >3 mg of lorazepam per day (P = .042). Dose–response relationships have been reported in prior studies, particularly in patients with panic disorder and pharmacokinetic studies reveal relationships between exposure (eg, plasma concentrations), response, and tolerability.Reference Ciraulo, Barnhill, Boxenbaum, Greenblatt and Smith 30 , Reference Greenblatt and Wright 31 In one study of adults with panic disorder, the greatest response occurred when alprazolam plasma concentrations were 20 to 40 ng/mL and this was superior to concentrations <20 ng/mL with no additional benefit at levels >40 ng/mL. Additionally, as plasma concentrations increase, side effects, including drowsiness and sedation, increase.Reference Ciraulo, Barnhill, Boxenbaum, Greenblatt and Smith 32 This suggests that the loss of a dose–response relationship at higher doses (or plasma concentrations) may be confounded by side effects and tolerability concerns. This is consistent with insurance claims data suggesting that higher doses of benzodiazepines are associated with greater depressive symptoms.Reference Greenblatt and Wright 33 As such it remains possible that the low doses, which in our analyses, provided the best response, represent the optimal balance between efficacy and tolerability. However, regardless of the mechanism, for clinicians, low and medium doses are preferable to high dose treatment.
Pharmacologic properties of the specific benzodiazepines were associated with treatment response. Specifically, less lipophilic benzodiazepines produced a greater response and, when compared to lorazepam (reference response), clonazepam was superior. Importantly clonazepam—like lorazepam and alprazolam—is a high potency benzodiazepine,Reference Griffin, Kaye, Rivera Bueno and Kaye 10 but has additional pharmacologic properties that may relate to its greater efficacy. Like other benzodiazepines, clonazepam is an agonist at the GABAA receptor but has weaker GABAA binding compared to other high potency benzodiazepines (eg, alprazolam) which may relate to less amnestic effects and improved tolerability.Reference Griffin, Kaye, Rivera Bueno and Kaye 10 Beyond this, clonazepam affects serotonergic transmission. In preclinical models, acute and chronic clonazepam decreases hippocampal 5-HT turnover (reflected by reduced 5-HT to 5-hydroxyindoleacetic acid ratios) and appears to agonize 5-HT1A receptors, which may contribute to its anxiolytic effects.Reference Greenblatt, Von Moltke and Harmatz 34 This may also accelerate response as in studies of adjunctive clonazepam in panic disorder and social anxiety.
In our analyses, less lipophilic benzodiazepines—including clonazepam—produced greater and more rapid improvement. This may relate to clearance and redistribution as well as tolerability. Less lipophilic agents are absorbed slowly and have a slower onset of action compared to more lipophilic benzodiazepines. Less lipophilic benzodiazepines have a longer duration of action because of their slower redistribution which culminates in a shorter half-life. In essence, this means that other things being equal, a less lipophilic benzodiazepine would produce a more sustained anxiolytic effect. Additionally, lipophilicity may subtend tolerability effect (eg, more lipophilic benzodiazepines are associated with less amnestic effects) which could relate to the greater efficacy of less lipophilic benzodiazepines in the present analysis.
While this is one of only a few meta-analyses of benzodiazepines in anxiety disorders and the first to examine the trajectory of benzodiazepine-related improvement and its pharmacologic predictors and placebo response, there are several limitations. First, despite the general similarity of studies and our use of BHMs to address the influence of heterogeneity assumptions, unobserved factors may still affect the response and response trajectory. These factors—which may be pharmacologic, clinical, or related to study design—are difficult, if not impossible to measure in meta-analyses. Second, some studies focused on specific disorders (eg, social anxiety disorder, GAD, separation anxiety disorder, and panic disorder); however, our analyses and sensitivity analyses suggest that the type of anxiety disorder does not influence either the trajectory of magnitude or response. Third, the studies differed in baseline anxiety severity, raising the possibility of a floor effect in studies that included patients with milder symptoms. Fourth, the risk of bias may vary among studies and influence these findings. This may be particularly the case with benzodiazepines which, in general, work quickly and have a distinct tolerability profile relative to other pharmacologic interventions (eg, SSRIs). Fifth, although dropout was examined as a tolerability proxy in some post hoc comparisons, we were limited in our ability to assess tolerability. This limitation was amplified by considerable heterogeneity in adverse event reporting across these studies and the change in adverse event classification over time, particularly for older studies completed prior to the use of standardized medical dictionaries for regulatory activities (ie, MedRA).
Taken together, our results suggest that benzodiazepine response occurs very early, that placebo response plateaus (relatively early) and that pharmacologic characteristics predict benzodiazepine response. Our results buttress available data and prior meta-analyses of the efficacy of benzodiazepines in anxiety disorders. Further, our findings clarify the trajectory of response and suggest that, when benzodiazepines are clinically appropriate, lower doses as well as less lipophilic benzodiazepines provide the greatest and fastest response.
Disclosures
Jeffrey R. Strawn has received research support from the National Institutes of Health (NIMH/NICHD/NIEHS) as well as AbbVie and Neuronetics. He has received material support from Myriad Genetics and honoraria from Intracellular Therapeutics and Genomind. He receives royalties from the publication of two texts (Springer), serves as an author for UpToDate, and an Associate Editor for Current Psychiatry. Jeffrey R. Strawn and Jeffrey A. Mills also received research support from the Yung Family Foundation. Julia Stimpfl reports no potential conflicts of interest.
Author Contributions
Conceptualization: J.N.S., J.R.S., J.A.M.; Data curation: J.N.S., J.A.M., J.R.S.; Formal analysis: J.A.M.; Funding acquisition: J.R.S.; Investigation: J.N.S., J.R.S.; Methodology: J.A.M., J.R.S.; Project administration: J.R.S.; Visualization: J.A.M., J.R.S.; Writing—original draft: J.R.S., J.A.M.; Writing—review and editing: J.NS., J.R.S., J.A.M.
Supplementary Materials
To view supplementary material for this article, please visit http://doi.org/10.1017/S1092852921000870.