



Introduction
The frontal sinus was historically described as being connected to the anterior ethmoids by a tubular, duct-like structure called the ‘frontonasal duct’, which was later redefined as a recess rather than a duct.Reference Stammberger and Posawetz1,Reference Zinreich, Kuhn, London, Kennedy, Solaiyappan and Hosemann2 In the endoscopic era, the frontal recess was also referred to as the ‘pre-chambers’ or as the most anterior and superior part of the anterior ethmoid complexes with defined boundaries.Reference Stammberger and Posawetz1,Reference Rimmer3 But more recently, three-dimensional (3D) stereoscopic imaging has challenged the idea that the frontal sinus and recess have an exactly definable anatomical landmark separating the two spaces.Reference Zinreich, Kuhn, London, Kennedy, Solaiyappan and Hosemann2
Inflammatory disease of the frontal sinus is believed to occur mostly because of the obstruction caused by anatomical variations of the inferior third of the frontal sinus drainage pathway.Reference Dassi, Demarco, Mangussi-Gomes, Weber, Balsalobre and Stamm4 The agger nasi cell, uncinate process and bulla ethmoidalis are important structures in the frontal recess.Reference Dassi, Demarco, Mangussi-Gomes, Weber, Balsalobre and Stamm4,Reference Wormald5 PJ Wormald proposed the agger nasi cell as the key to understanding the regional anatomy and approach for frontal sinus surgery.Reference Wormald5–Reference Wormald, Hoseman, Callejas, Weber, Kennedy and Citardi7 As the bulla ethmoidalis forms the posterior limit of the frontal recess, its preservation during frontal recess dissection also provides an essential landmark for posterior limit dissection.Reference Dassi, Demarco, Mangussi-Gomes, Weber, Balsalobre and Stamm4 Meanwhile, others have used different insertions of the superior portion of the uncinate process into either the lamina papyracea, skull base, middle turbinate or a combination of these as a landmark for the frontal sinus drainage pathway location. Much emphasis has also been placed on how the upward continuation of the uncinate process is influenced by agger nasi cell pneumatisation and anterior ethmoidal cells in the frontal recess in relation to understanding the frontal sinus drainage pathway.Reference Dassi, Demarco, Mangussi-Gomes, Weber, Balsalobre and Stamm4,Reference Wormald6,Reference Bing, Demin, Huachao, Qjan, Luo and Ming8,Reference Landsberg and Friedman9
Our understanding of the frontal sinus drainage pathway and its landmarks continues to expand with the recent description of the anterior ethmoidal genu by Bolger et al.Reference Bolger, Stammberger, Ishii, Ponikau, Solaiyappan and Zinreich10 Their investigation encountered a posteriorly directed component of the uncinate process and an anteriorly directed component of the ethmoidal bulla that fused together to create a consistent anatomical feature, medial to which the frontal sinus drains in 77 per cent of the cases. Although the uncinate process and bulla ethmoidalis were considered as lamellar structures, this report showed that they are not separate structures. Their fusion point or anterior ethmoidal genu is closely related to the frontal sinus drainage pathway and can be used as a landmark in anterior ethmoid and frontal recess surgery.
We further explored this anatomical description and its relationship to frontal sinus drainage pathway and the cells in the frontal recess in order to expand on earlier findings.
Materials and methods
We performed a retrospective analysis on patients who underwent paranasal sinus computed tomography (CT) scans as part of a clinical workup in tertiary care otorhinolaryngology hospitals. This was a descriptive cross-sectional study, performed at two hospitals, the University Malaya Medical Centre, Malaysia, and Sligo University Hospital, Ireland. The study protocol was approved by the institutional review board from both hospitals.
All CT scans were acquired using Siemens (Dublin, Ireland) and Philips (Kuala Lumpur, Malaysia) equipment without intravenous contrast. The scans were selected at random and screened using inclusion and exclusion criteria.
The inclusion criteria included high resolution CT scans performed on adults who were more than 18 years old with contiguous, fine-cut axial image acquisition (0.6–1 mm slice thickness), allowing for multiplanar reconstruction. Exclusion criteria included CT scans with diseased sinuses, previous trauma, craniofacial anomaly or previous sinus surgery.
Axial, coronal and sagittal reconstruction of the CT images was performed and reviewed on a computer software program with multiplanar and localisation ability (Horos medical image viewing software, version 3.3.6). The anatomy structures were identified and measured using the same software tools.
Sagittal reconstructions were studied from a medial to lateral perspective, beginning within the olfactory cleft and ending at the lamina papyracea. The uncinate process, bulla ethmoidalis and agger nasi cell were visualised to determine if they were separate structures or if they were connected to form the anterior ethmoidal genu. Thereafter, scans were reviewed in the coronal plane from the anterior to posterior and then in an axial plane from the inferior to superior. The anterior ethmoidal genu is recognised when the superior aspect of the vertical part of the uncinate process, attached to the posteromedial wall of agger nasi cell, bends abruptly to attach to the bulla ethmoidalis. In this study, we defined a recess as formed when the anterior ethmoidal genu extends laterally until the lamina papyracea with a space present between the agger nasi cell and bulla ethmoidalis.
The anatomical relationship between the anterior ethmoidal genu, frontal sinus drainage pathway and frontal recess cells was recorded. We also measured the distance between the anterior ethmoidal genu and the frontal sinus ostia. The frontal ostia location was arbitrarily chosen as the point where the line passing through the junction between the posterior table of the frontal sinus and fovea ethmoidalis and the junction of the frontal beak and nasal bone intersects a perpendicular line from the anterior ethmoidal genu. The agger nasi cell dimension (height, width and length) was measured and used for calculation of its volume.
Statistical analyses were performed with SPSS® statistical analysis software (version 22.0). Pearson's correlation analysis was used to determine the relationship between agger nasi cell wall length and anterior ethmoidal genu height and position in the frontal sinus drainage pathway.
Results
The study involved 26 male and 30 female patients, with a total of 112 CT images of sinuses (right and left), recruited for analysis based on normal CT scan reports. However, during analysis, we noticed some of the CT images had artifacts and mucosal thickening around the area of interest, which hinders viewing of the normal anatomy. Therefore, only 102 sides of the normal CT paranasal sinus scans were used for the final analysis. The age of the patients ranged from 21 to 88 years (mean, 50 ± 15.82 years). Thirty-eight CT images were from Caucasians, and 64 CT images were from Malaysians (Table 1).
Table 1. Demographic data

SD = standard deviation.
The anterior ethmoid genu was present in all the CT paranasal sinus images analysed in this study (n = 102; Figure 1). The anterior ethmoidal genu recess was consistently observed when the posterior wall of agger nasi cell and anterior wall of bulla ethmoidalis did not come in contact with each other and the anterior ethmoidal genu extended laterally towards the lamina papyracea. This recess is therefore bound anteriorly by the posterior wall of the agger nasi cell, posteriorly by the bulla ethmoidalis and laterally by lamina papyracea (Figure 2), creating a 3D space.

Fig. 1. The anterior ethmoid genu identified at the crossbar in computed tomography scans reconstructed in multiplanar views: (a) sagittal, (b) axial and (c) coronal view. Sagittal view (a) gives the best appearance of the genu or bend.
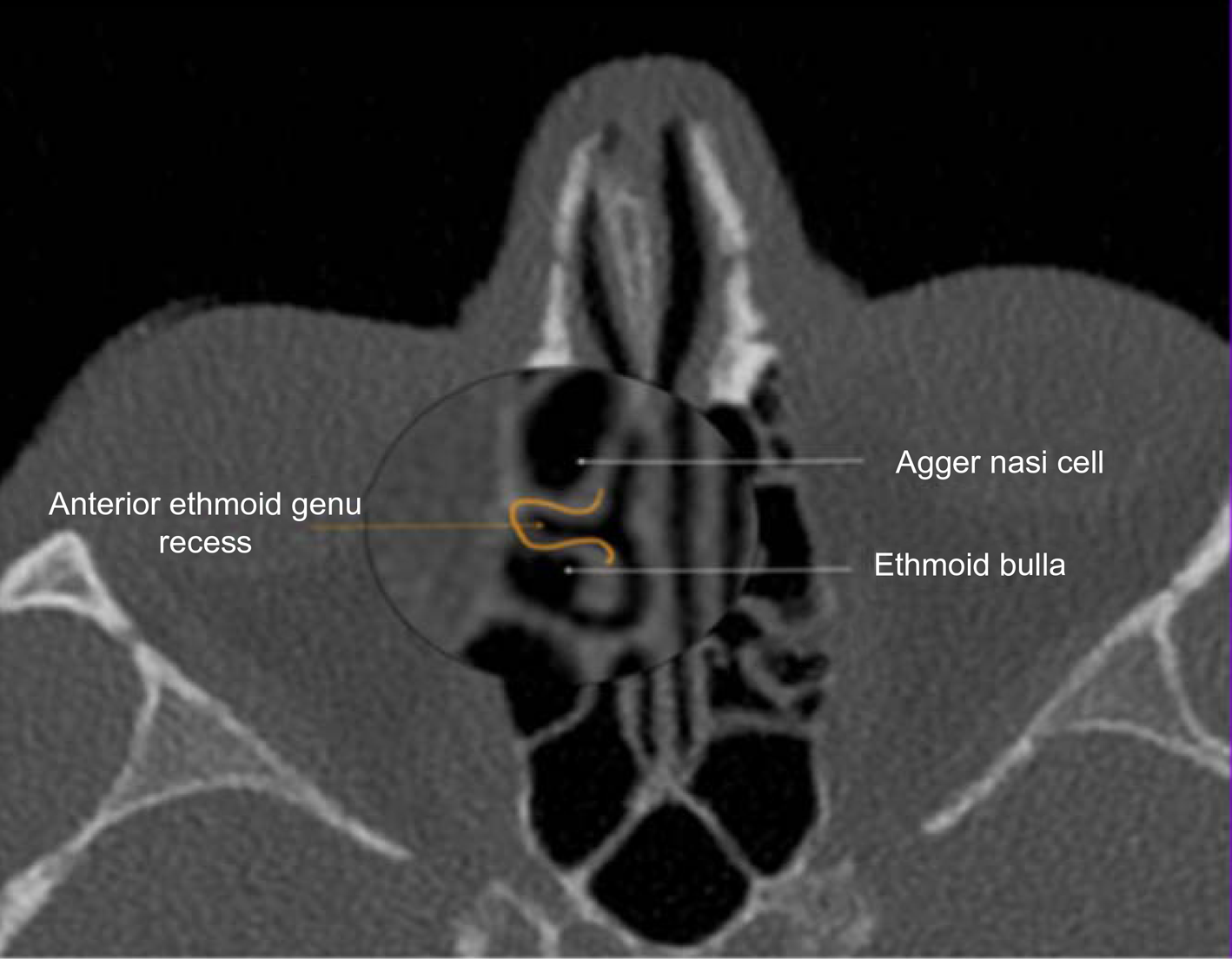
Fig. 2. Axial plane computed tomography image with right anterior ethmoid genu recess boundary marked in orange. It is bounded by the agger nasi cell (anteriorly), bulla ethmoidalis (posteriorly) and lamina papyracea (laterally), creating a three-dimensional space.
The recess was present in 27 patients. The final part of the frontal sinus drainage was within this recess.
In our analysis, the distal part of the frontal sinus drainage pathway drained medial to the anterior ethmoidal genu in the majority of sinus complexes (96 per cent of CT scans; n = 98 of 102). Only four sides demonstrated a drainage pattern lateral to it.
On average, the distance between the anterior ethmoidal genu and frontal sinus isthmus was 12 mm (Figure 3). We observed that the higher the anterior ethmoidal genu position is in the frontal sinus drainage pathway, the shorter the distance between anterior ethmoidal genu and frontal sinus isthmus. This unreciprocal relationship between these two points was further analysed to describe its relationship with the frontal recess cells.
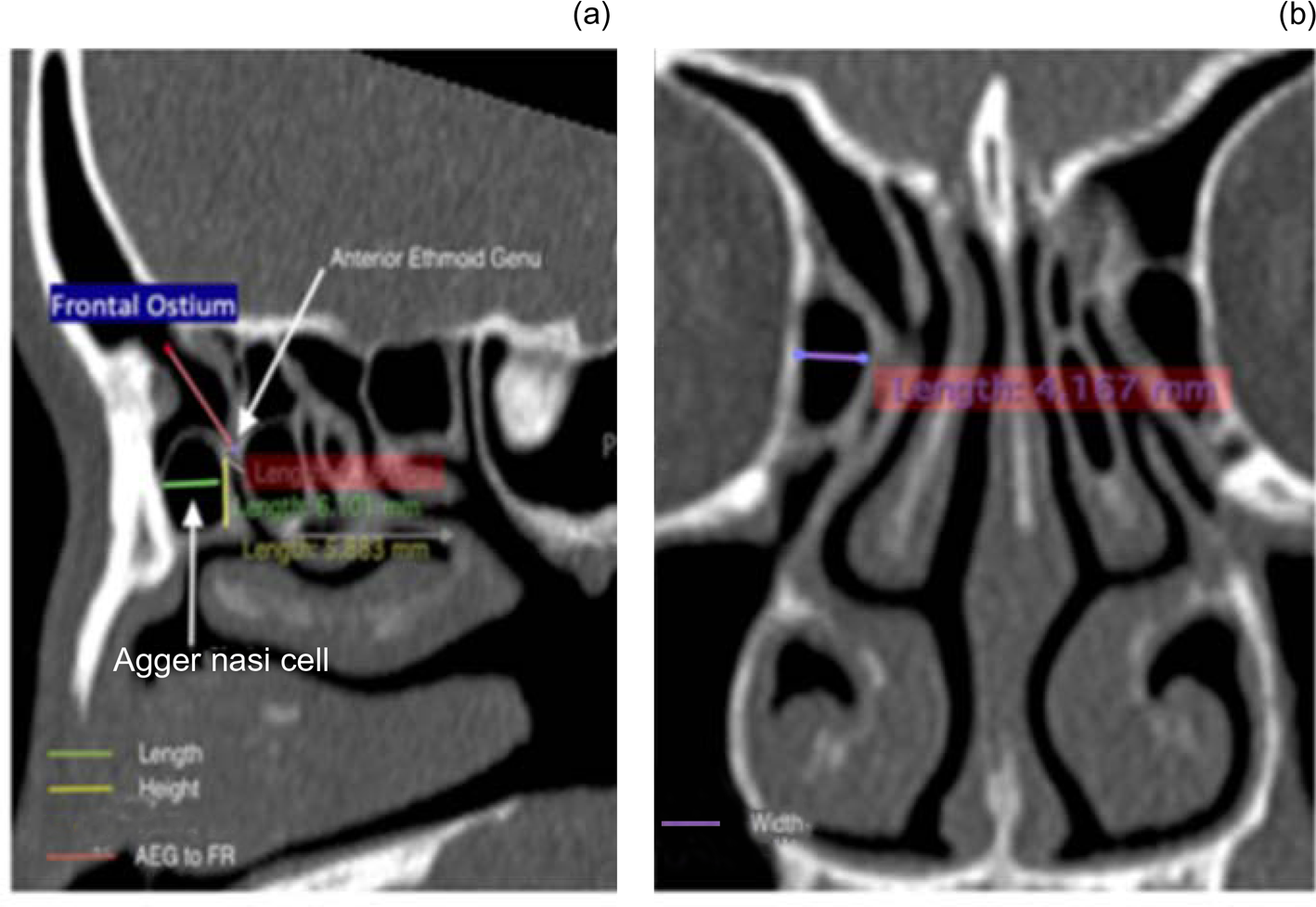
Fig. 3. (a) Sagittal plane computed tomography image showing agger nasi cell dimensions (length in green = 6.10 mm; height in yellow = 5.88 mm). Distance from anterior ethmoid genu (AEG) to frontal recess (FR) (red line) = 11.84 mm. (b) Coronal plane computed tomography image showing agger nasi cell (width in purple = 4.17 mm).
The position of the anterior ethmoidal genu in the frontal sinus drainage pathway is specifically related to the agger nasi cell. The superior part of uncinate process has been shown by previous research to be attached to posteromedial aspect of agger nasi cell. In this study, we also made another observation that the anterior ethmoidal genu is formed at the junction between the posterior wall and roof of the agger nasi cell, and this was consistent in all scans as well. Because it is only attached to posterior wall of agger nasi cell, we hypothesised that rather than the volume, the height and length of the posterior wall of the agger nasi cell determines the position of the anterior ethmoidal genu in the frontal sinus drainage pathway. We explored this relationship by measuring the dimension and size of the agger nasi cell and assessed its correlation to the height and length of the anterior ethmoidal genu.
Interestingly, rather than the volume of agger nasi cell, only the height of posterior wall of agger nasi cell showed significant correlation with regard to the anterior ethmoidal genu position in the frontal sinus drainage pathway. Pearson correlation analysis between the height of the posterior wall and distance from the anterior ethmoidal genu to the frontal ostium showed significant moderate correlation with coefficients of −0.503 (p < 0.001).
Discussion
The agger nasi cell and the uncinate process and their interactions have been repeatedly referred to as important anatomical landmarks for gaining access to the frontal sinus drainage pathway.Reference Wormald5,Reference Ximendes, Gomes, Balieiro, Ferreira, Lopes and Balsalobre11–Reference Ercan, Çakir, Sayin, Başak and Turgut13 The description of anterior ethmoid genu in the 3D CT scanning analysis by Bolger et al. showed that the uncinate process and bulla ethmoidalis were also fused together at the superior aspect of the hiatus semilunaris in a way that resembled a flexed knee or ‘genu’ in all cases.Reference Bolger, Stammberger, Ishii, Ponikau, Solaiyappan and Zinreich10 Using gross anatomic and endoscopic dissection of sinonasal complexes, they found this genu-like feature was closely related to the frontal sinus drainage pathway.Reference Bolger, Stammberger, Ishii, Ponikau, Solaiyappan and Zinreich10
Similar to the study by Bolger et al., all of the 102 scans in this study demonstrated the presence of the anterior ethmoidal genu as a constant landmark independent of age, gender and race. It was an easily recognisable structure on high resolution CT scans of the sinuses with a characteristic ‘genu’ like appearance that was best seen in the sagittal plane.
The frontal sinus may drain either medially or laterally in relation to the anterior ethmoidal genu, and in our cohort of patients, the most common drainage pattern was medial to the anterior ethmoidal genu (96 per cent). A similar drainage pattern was observed in the study by Bolger et al., where the frontal sinus drained medially in 77 per cent of cases (n = 44 of 57). However, in this study, this medial predilection was present more so in the endoscopic and radiographic analysis than in the gross anatomic analysis (endoscopic, 15 of 18, 83 per cent; radiographic, 14 of 15, 93 per cent; gross anatomic, 15 of 24, 63 per cent), probably attributable to the small sample size in each group.Reference Bolger, Stammberger, Ishii, Ponikau, Solaiyappan and Zinreich10
In addition, when the anterior ethmoidal genu formed a recess, the frontal sinus drainage was always medial or within this recess. Bolger et al. made a note of this in their sagittal cadaveric dissections, mentioning a small 3D space lateral to the genu.Reference Bolger, Stammberger, Ishii, Ponikau, Solaiyappan and Zinreich10
A review of the existing landmarks for the frontal recess surgery showed that the ‘region around the anterior ethmoidal genu’ was constantly used as an anatomical landmark by others, but there was a variety of descriptions and nomenclature. Messerklinger (1978) described this as a ‘bridge of bone’ between the uncinate process and the convexity of the bulla.Reference Stammberger and Posawetz1 Yoon et al. showed that the superior portion of the uncinate process and bulla ethmoidalis joined to form the bony plate in the sagittal plane and that it attaches superiorly to the skull base, the frontal bone and the floor of the frontal sinus; they termed it the suprainfundibular plate. Removal of the suprainfundibular plate was advocated as a simplified access to the frontal sinus opening.Reference Stammberger and Posawetz1,Reference Yoon, Moon, Kim, Hong, Kang and Kim14 A further analysis of the 100 CT scans and endoscopic dissection on 50 adult cadavers showed that the frontal sinus opened medially to the suprainfundibular plate in 60 per cent of the cases and laterally in 40 per cent.Reference Yoon, Moon, Kim, Hong, Kang and Kim14
Stamm et al. used the ‘vertical bar’ concept in endoscopic sinus surgery.Reference Stamm, Nogueira, Americo and Solferini Silva15 Here the description of vertical bar refers to the postero-superior portion of the uncinate process that forms the medial wall of the agger nasi cell, which for this discussion can perhaps be considered as the anterior limb of the anterior ethmoidal genu. PJ Wormald also reported that the upward extension of the uncinate process gave a bony leaflet to the bulla ethmoidalis, forming a plate of bone.Reference Wormald5 These prior findings, reported by different authors at different time periods, have essentially described the common lamella that projected from the anterior ethmoidal genu. Therefore the anterior ethmoidal genu is the inferior most border of the common lamella.
In order to understand the anterior ethmoidal genu as an anatomical concept to gain access to frontal sinus drainage pathway endoscopically, it is worthwhile revisiting the anatomy of the anterior ethmoids and frontal sinus region. Embryologically, the uncinate process and ethmoid bulla have a common primitive origin, referred to as secondary ethmoturbinals.Reference Bolger, Stammberger, Ishii, Ponikau, Solaiyappan and Zinreich10 During human development, pneumatisation of this ethmoturbinal leads to evaginations of tissue to form the ethmoidal bulla and uncinate process lamellae and a corresponding invagination between them called the ethmoidal infundibulum. At the superior aspect of the invagination, the secondary ethmoturbinals fuse into a single tissue mass, later differentiating into the bulla ethmoidalis, attached at the superior aspect of the hiatus semilunaris; they are not a separate lamellar structure as taught in the past.
In our analysis of anterior ethmoidal genu, we found agger nasi cell has influence on the position of anterior ethmoidal genu in the frontal sinus drainage pathway. The anterior ethmoidal genu is typically formed at the junction of the posterior wall and roof of agger nasi cell in all cases. In addition, the position of the anterior ethmoidal genu in the frontal recess is determined by the agger nasi cell's posterior wall dimension, regardless of its shape or size.
• Frontal sinus anatomy is complex and highly variable because of multiple lamellae and air cells
• Recent description of the anterior ethmoidal genu has improved understanding of the frontal sinus drainage pathway
• The anterior ethmoid genu can be used as an additional landmark for frontal sinus surgery because it was identified in all cases
• The anterior ethmoidal genu would be an easy landmark to access the frontal sinus
• Further study that explores the functionality of the anterior ethmoidal genu as a reliable landmark to access the frontal sinus is warranted
Yoon et al. also noted that the length and width of the suprainfundibular plate varied.Reference Yoon, Moon, Kim, Hong, Kang and Kim14 Since the anterior ethmoidal genu is positioned distally in the frontal sinus drainage pathway, we measured proximity of the anterior ethmoidal genu to the frontal sinus ostium to give a theoretical estimation for frontal sinus instrumentation. However, since this is a preliminary finding in non-diseased sinuses, interpreting this data in diseased sinuses might be different; thus further cadaveric or endoscopic dissection study is warranted.
Although this study gives an added description of the anterior ethmoidal genu and potentiates its usage as a landmark in frontal sinus surgery, it is not without limitations. CT scans in the present study were limited to patients with non-diseased sinuses to measure the prevalence of anterior ethmoidal genu. Assessment in diseased sinuses might impose difficulties in identifying this anatomy. This should be kept in mind when translating this finding to diseased patients. The understanding and evaluation of the surgical anatomy of the frontal recess and frontal sinus will not be complete without a comprehensive analysis of all other anatomical variants of this region as well.
Conclusion
The anterior ethmoid genu can be used as an additional landmark for frontal sinus surgery because it was identified in all cases and the frontal sinus drainage is mostly medial to it. It is also easily detectable with high resolution CT scans of paranasal sinuses.
Although this analysis was performed on non-diseased sinuses, the outcome of this study has recognised the anatomical interaction between the uncinate process, agger nasi cell and ethmoid bulla forming a common lamella with the anterior ethmoidal genu being the inferior most margin of it. Being a constant anatomical structure in the frontal sinus drainage pathway, the anterior ethmoidal genu should be explored further by endoscopic analysis to assess its full potential as an anatomical landmark for endoscopic sinus surgery.
Acknowledgements
The authors would like to take this opportunity to extend gratitude to all who have made this research possible. Sincere thanks go to Dr William E Bolger who encouraged the authors to further explore his preliminary findings on the anterior ethmoid genu. In addition, the authors are grateful to Dr Aynesha Letchimikanthan for her assistance in collecting computed tomography imaging.
Competing interests
None declared




