



Introduction
Ultra-processed foods (UPFs), according to the NOVA classification, are industrial formulations of processed food substances (oils, fats, sugars, starch, protein isolates) that contain little or no whole food and typically include flavourings, colourings, emulsifiers and other cosmetic additives(Reference Monteiro, Cannon and Levy1). Processes and ingredients used for the manufacture of UPFs are designed to create low-cost, highly profitable products, which are extremely palatable, convenient to use (ready-to-eat and long-lasting) and are liable to displace all other NOVA food groups (unprocessed, minimally processed and processed) and the culinary preparations made with these foods(Reference Monteiro, Cannon and Levy1).
Large cohort studies carried out in different countries have shown that increased dietary share of UPFs results in a higher risk of overweight/obesity, hypertension, coronary and cerebrovascular diseases, diabetes, overall and breast cancer, and all-cause mortality(Reference Srour, Fezeu and Kesse-Guyot2–Reference Schnabel, Kesse-Guyot and Allès4). The positive association of diets high in UPFs with excessive energy intake and weight gain was confirmed in a randomized clinical trial(Reference Hall, Ayuketah and Brychta5).
Although multiple mechanisms for the association between UPF intake and non-communicable diseases (NCDs) have been envisaged(Reference Monteiro, Cannon and Levy1) including the lower satiety potential and higher glycemic index of these foods(Reference Monteiro, Cannon and Levy1) and the presence of additives such as artificial sweeteners and emulsifiers(Reference Srour, Fezeu and Kesse-Guyot2), and of compounds that are neoformed during processing or released from packaging(Reference Srour, Fezeu and Kesse-Guyot2), the most obvious mechanism is their effect on the nutrient profile of the overall diet.
Indeed, nationally representative studies conducted in Brazil(Reference Costa Louzada, Martins and Canella6), Chile(Reference Cediel, Reyes and Corvalán7), Colombia(Reference Parra, da Costa-Louzada and Moubarac8), Mexico(Reference Marrón-Ponce, Flores and Cediel9), Australia(Reference Machado, Martinez Steele and Levy10), the UK(Reference Rauber, da Costa Louzada and Steele11), Canada(Reference Moubarac, Batal and Louzada12) and the US(Reference Martínez Steele, Popkin and Swinburn13) have shown that increased UPF intake was associated with non-recommended intakes of most nutrients critical to NCDs, including saturated fatty acids(14).
Although recent evidence suggests that the health effects of saturated fatty acids may vary depending on the type of fatty acid and on the specific food source(Reference Astrup, Bertram and Bonjour15), a recent dietary recommendation from the World Health Organization confirmed the need of limiting saturated fatty acid intake to less than 10 % of total energy intake(16). This recommendation was based on systematic review and meta-analyses of results from all randomized controlled trials and cohort studies that have examined the association between saturated fatty acid intake and incidence of and mortality by cardiovascular disease (CVD)(16). Also based on systematic review and meta-analyses, the American Heart Association is still more restrictive and recommends limiting saturated fatty acid intake to 5–6 % of total energy intake(Reference Van Horn, Carson and Appel17). The most recent national dietary guidelines from each of eight countries included in the present study also recommend limiting saturated fatty acid intake to reduce CVDs(18–25).
The present paper describes for the first time, the proportion of excessive saturated fatty acid intake (>10 % of total energy intake) that could be potentially avoided, if UPF consumption was reduced to levels observed among the lowest consumers (the first quintile) across eight countries.
Material and methods
Data sources
All data used by the present study come from most recently available national dietary surveys carried out in Brazil (2008–9)(Reference Costa Louzada, Martins and Canella6), Chile (2010)(Reference Cediel, Reyes and Corvalán7), Colombia (2005)(Reference Parra, da Costa-Louzada and Moubarac8), Mexico (2012)(Reference Marrón-Ponce, Flores and Cediel9), Australia (2011–12)(Reference Machado, Martinez Steele and Levy10), the UK (2008–16)(Reference Rauber, da Costa Louzada and Steele11), Canada (2015)(Reference Moubarac, Batal and Louzada12) and the US (2015–16)(Reference Martínez Steele, Popkin and Swinburn13). Relevant characteristics of these surveys, including age groups studied, sample sizes, dietary assessment methods and food composition tables, are described in Table 1. Briefly, UK used 4-d food diaries; Mexico and Canada used 1-d 24-h recalls, while the remaining countries used 2-d 24-h recalls. The analytical samples were restricted to participants with 3 or 4 d of food diary in the UK, one dietary recall in Mexico and Canada, two dietary recalls in Brazil and up to two dietary recalls in the remaining countries.
Table 1. Characteristics of nationally representative dietary surveys in eight countries

The present study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Research Ethics Committee from the Faculdade de Saúde Pública at the Universidade de São Paulo (Protocol 128958, 19 October 2012); Comité de Ética de Investigación de la Escuela de Medicina de la Pontificia Universidad Católica de Chile; Comité de ética de la Universidad del Rosario (Bogotá, Colombia); INSP Research, Biosafety, and Ethics Committee in Cuernavaca, Mexico; Australian Government Department of Health and Ageing Departmental Ethnics Committee in 2011; UK relevant research ethics and governance committees; Comité d’éthique de la recherche en sciences et en santé (CERSES) of Université de Montréal (17-017-CERES-D); US NCHS Research Ethics Review Board (ERB) Approval (Continuation of Protocol #2011–17). Written informed consent was obtained from all subjects.
Data analysis
All analyses were run separately for each country using mean of 3 or 4 d of food diaries in the UK, day 1 dietary recall data in Mexico and Canada, mean day 1 and day 2 dietary recall data in Brazil, and mean day 1 and day 2 dietary recall data if available and day 1 otherwise in the remaining countries. Continuous variables presented an approximately normal distribution. First, we calculated the mean percentage of energy intake from UPFs (classified using the NOVA system)(Reference Monteiro, Cannon and Levy1), the mean percentage of energy intake from saturated fatty acids and the percentage of intakes with excessive saturated fatty acid (>10 % of energy intake, according to WHO recommendation)(14,16) . Then, we used linear regression models to estimate the association between the dietary energy contribution of UPFs (categorised into quintiles) and the dietary content of saturated fatty acids (expressed as percentage of total energy). Poisson regression models with robust variance were used to assess whether the percentage of intakes with excessive saturated fatty acid increased across quintiles of the dietary energy contribution of UPFs.
To evaluate dose-response associations, tests of linear trend were performed by treating quintiles of UPF consumption as an ordinal (1–5) variable.
Finally, we estimated, again for each country, the UPF population attributable fraction (PAF) defined as the proportion of intakes with excessive saturated fatty acid intake that would be potentially avoided if UPF consumption (the exposure) was reduced to attainable values. We assumed attainable values to be those estimated in the first quintile of UPF consumption for each country.
We calculated PAF(Reference Steenland and Armstrong26,Reference Rezende and Eluf-Neto27) through the following equation:

where P population is the percentage of intakes with excessive saturated fatty acid in the total population and P nonexposed is the percentage of intakes with excessive saturated fatty acid in the first quintile of UPF consumption. All models were adjusted for the sociodemographic covariates displayed in Table 1. Statistical hypotheses were tested using a two-tailed P ≤ 0⋅05 level of significance. All analyses were conducted with Stata statistical software package version 14.
Results
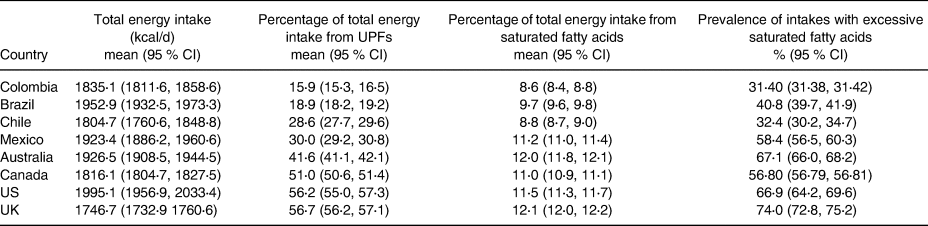
Table 2 describes overall energy contributions of UPF and saturated fatty acid intakes across the eight studied countries. The mean energy contribution of UPFs varied from 15⋅9 % (95 % CI 15⋅3, 16⋅5) in Colombia to 56⋅7 % (95 % CI 56⋅2, 57⋅1) in the UK. Colombia showed the lowest mean dietary intake of saturated fatty acids (8⋅6 % (95 % CI 8⋅4, 8⋅8) of total energy intake) and the lowest percentage of intakes with excessive saturated fatty acids (31⋅40 % (95 % CI 31⋅38, 31⋅42)) while the highest estimates for these two parameters were observed in the UK (12⋅1 % (95 % CI 12⋅0, 12⋅2) and 74⋅0 % (95 % CI 72⋅8, 75⋅2), respectively).
Table 2. Contribution of UPFs and saturated fatty acids to total energy intake (kcal/d) and prevalence of excessive saturated fatty acid intakes in eight countries
As depicted in Fig. 1, the adjusted mean dietary intake of saturated fatty acids increased significantly across quintiles of the dietary contribution of UPFs in all countries (P for linear trend <0⋅05). Supplementary Table S1 of Supplementary material describes the mean and range of the dietary contribution of UPFs per quintile.
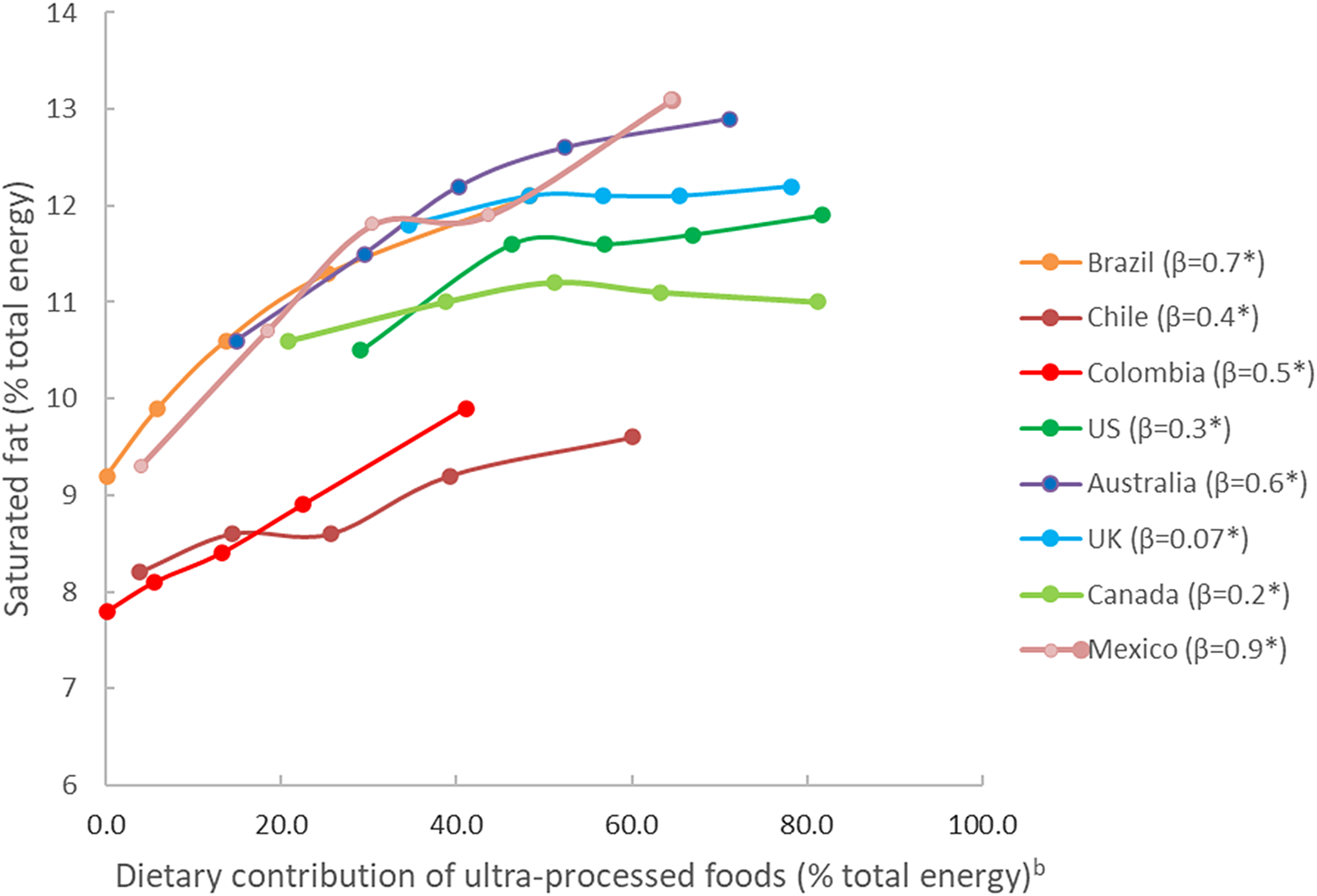
Fig. 1. Adjusteda mean dietary content of saturated fatty acids across quintiles of the dietary contribution of UPFs in eight countries. aAdjusted according to covariates listed in Table 1. bKnots corresponding to country-specific quintiles of the dietary contribution of UPFs. *Statistically significant coefficient for linear trend (P < 0⋅05).
Table 3 shows the adjusted percentage of excessive saturated fatty acid intakes according to quintiles of the dietary contribution of UPFs. In all eight countries, the percentage of intakes with excessive saturated fatty acids increased significantly across the quintiles (P for linear trend <0⋅001). The adjusted ratio of the percentage of intakes with excessive saturated fatty acid between extreme UPF quintiles ranged from 1⋅14 (95 % CI 1⋅07, 1⋅22) in Canada up to 2⋅05 (95 % CI 1⋅65, 2⋅54) in Chile (Fig. 2). The values in the first v. the last quintile almost doubled in Brazil, Mexico and Chile.

Fig. 2. Adjusteda PR of excessive saturated fatty acid intake (>10 %) between extreme quintiles of the dietary contribution of UPFs in eight countries. aAdjusted according to covariates listed in Table 1.
Table 3. Adjusteda percentage of intakes with excessive saturated fatty acids (>10 %) across quintiles of the dietary contribution of UPFs in eight countries
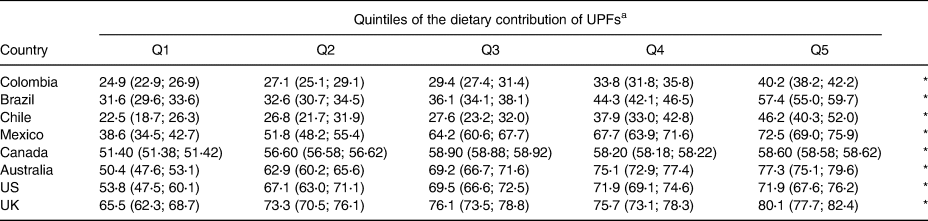
a Adjusted according to covariates listed in Table 1. 95 % CI in parenthesis.
* Statistically significant linear trend (P≤0⋅05).
If the dietary contribution of UPFs was reduced to levels observed in the first quintile of each country, statistically significant reductions in the percentage of excessive saturated fatty acid intakes would be observed in all eight countries. The reductions would vary from 10⋅0 % (95 % CI 6⋅2, 13⋅6) in Canada all the way up to 35⋅0 % (95 % CI 28⋅7, 40⋅8) in Mexico (Fig. 3).
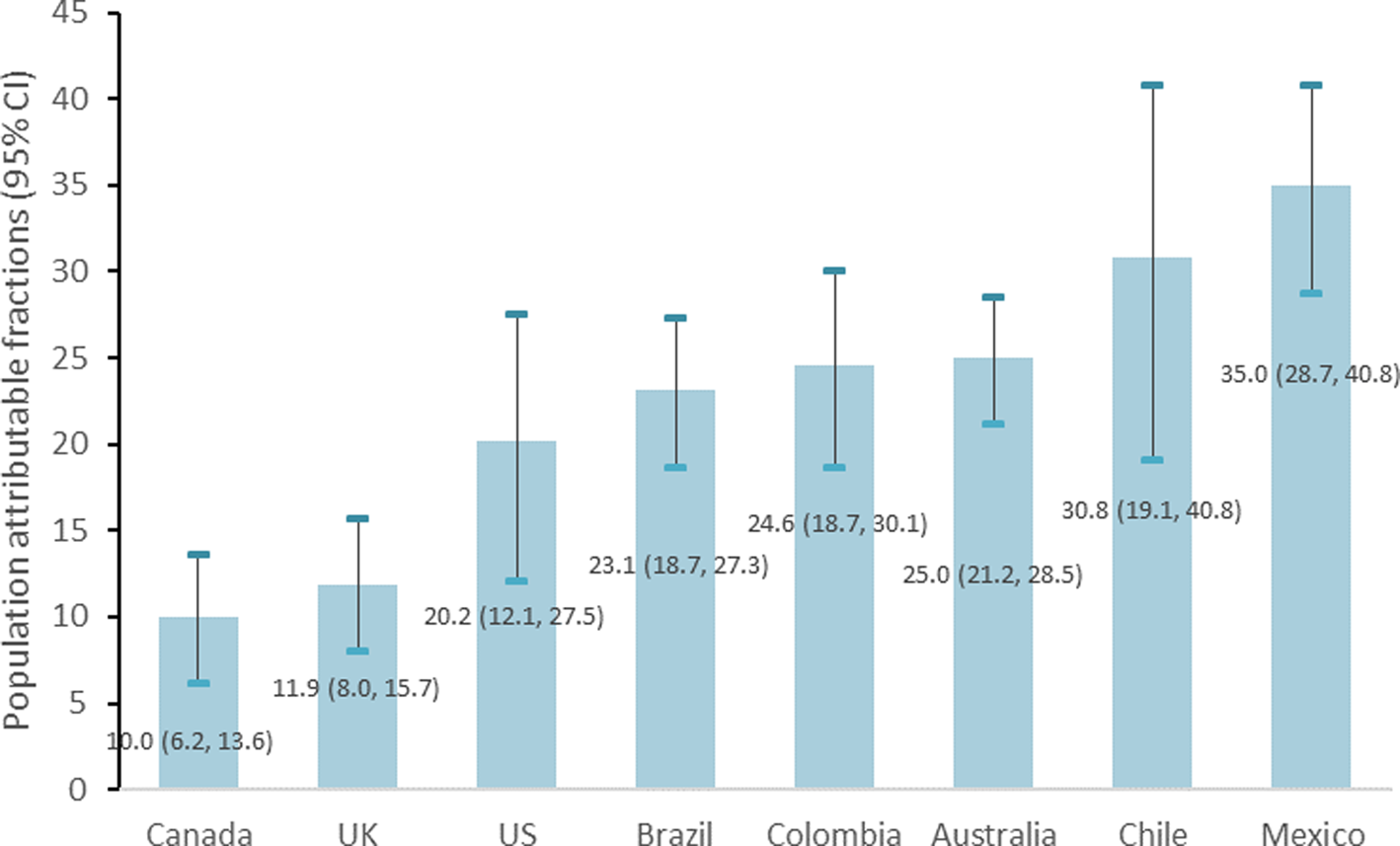
Fig. 3. Impact of UPF consumption on the adjusteda prevalence of excessive saturated fatty acid intake in eight countries. aAdjusted according to covariates listed in Table 1.
Discussion
In the present study across eight middle- and high-income countries, we observed that the rise in UPF consumption was systematically associated with an increase in both the mean saturated fatty acid intakes and in the percentage of excessive intakes. The percentage of excessive saturated fatty acid intakes would be significantly reduced in all countries (between 10 % in Canada and 35 % in Mexico), if UPF consumption was decreased to context-specific attainable levels such as those estimated for the lowest quintile of UPF consumption in each country.
Despite the fact that not all UPF items are a source of saturated fatty acids and some of them are even exempt of fat, soft drinks being an example, our findings show that, irrespective of the country, dietary patterns characterised by relatively higher overall contribution of UPFs tend to have a higher content of saturated fatty acids. One likely explanation is the frequent use of saturated fatty acid rich crude palm oil (51 % content of saturated fatty acids) and palm kernel oil (84 % content of saturated fatty acids)(Reference Vaclavik and Christian28) in the manufacture of several UPFs such as baked goods, candies, cakes, cheese analogues, chips, chocolate, confectionary fats, cookies, crackers, doughnuts, frozen meals (pancakes, pies, pizza, potatoes), ice cream, instant noodles, margarines, shortenings and other butter substitutes, microwave popcorn, non-dairy creamers, salad dressings, snacks, soups, among others(Reference Mba, Dumont and Ngadi29,Reference Mancini, Imperlini and Nigro30) . The preference for these oils and their fractions and blends lies in their fragrance and neutral taste and in their capacity to confer the texture obtained with the use of butter or lard (without the need of using hydrogenation, thus reducing trans-fat content) as well as to increase the thermal and oxidative stability of the fat, and thus the shelf life of the final product(Reference Vaclavik and Christian28,Reference Mba, Dumont and Ngadi29) . The high productivity of palm oil, which is able to produce up to ten times more oil per hectare of plantation than other leading oilseed crops(31), may be an additional economic force driving its use in UPFs. In fact, in 2012, crude palm oil and palm kernel oil (both extracted from palm fruit) overtook soybean oil as the most important vegetable oil in the world, accounting for 32 % of global fats and oils production, 90 % of which being used by the edible food industry(Reference Mba, Dumont and Ngadi29,31) .
The relationship found between UPF consumption and excessive saturated fatty acid intake indicates that these intakes may be one of the mechanisms for the prospective association between UPF consumption and both cardiovascular diseases(Reference Srour, Fezeu and Kesse-Guyot2,Reference Bonaccio, Di Castelnuovo and Costanzo32) and several major risk factors for these diseases, including overweight and obesity, hypertension, dyslipidaemia and diabetes(Reference Srour, Fezeu and Kesse-Guyot2,Reference Srour, Fezeu and Kesse-Guyot3,Reference Rauber, Campagnolo and Hoffman33) .
Taxes, front-of-pack labels and dietary guidelines are potential vehicles that can be used to discourage the consumption of UPFs. However, while reducing UPF consumption to levels observed in the first quintile would help, this is not enough to eliminate excessive saturated fatty acid intake. Australia, UK, Canada and US would still have over 50 % percentage of excessive intakes, Brazil and Mexico over 30 %, and Chile and Colombia over 20 %. Especially in the UK and US but also in Australia and Canada, with already significant UPF consumption in the first quintile, countries would need to set goals to reduce UPFs well below levels observed in the first quintile. In Brazil, Mexico, Chile and Colombia, in which mean UPF contribution is already below 5 % in the first quintile, countries would need to extend the reduction to non-ultra-processed sources of saturated fatty acids such as meat, butter and cheese.
On the other hand, in all eight countries evaluated in the present study, UPF consumption was shown to be inversely related to protein and fibre intakes and directly related to free sugar intake(Reference Costa Louzada, Martins and Canella6–Reference Martínez Steele, Popkin and Swinburn13) suggesting that UPFs tend to replace healthier sources of food and that reducing its consumption would probably entail additional cardiovascular and other health benefits.
Strengths of the present study include the use of large, nationally representative samples of the population of eight middle- and high-income countries, maximising external validity of results. The use of individual consumption data rather than market disappearance or household purchasing data, which may under- or overestimate amounts consumed, is an additional strength of the present study as well as the fact that the NOVA classification was applied similarly across all countries after disaggregating handmade recipes into underlying ingredients, maximising the comparability across settings. The use of context-specific scenarios across the countries for estimating the reduction in the percentage of intakes with excessive fatty acids is also a strength of the present study.
Though the most recent surveys were used for each country, the years of data collection were less recent in some countries possibly not reflecting actual consumption and also limiting comparisons across countries. Despite existing evidence of the increasing trends in UPF consumption in many countries(Reference Vandevijvere, Jaacks and Monteiro34), how this should affect the population attributable fractions is less clear because it depends much more on the difference in risk between the first and all other quintiles than on the absolute contribution of UPFs to the diet. Though sample sizes varied from country to country ranging from 4920 in Chile to 38 643 in Colombia, all provided statistically significant and relatively precise PAFs (see Fig. 3). Random and systematic error may bias self-reported dietary intake data collected through 24-h recall/food diaries, especially regarding absolute energy intakes, even though the applied standardised methods should contribute to minimising it, and also the fact that we always used relative estimates. Though social desirability bias may lead to an underestimation of the dietary contribution of UPFs and of saturated fatty acids, this would most likely not affect the association between the two variables or it would bias the association towards the null. Despite these limitations inherent to self-reported diet, 24-h recalls/food diaries are considered the least biased method and the best for describing dietary intake at the population level(Reference Prentice, Mossavar-Rahmani and Huang35). In most countries, the assessment of dietary intakes was exclusively or mostly based on 1 d recalls potentially overestimating the frequency of individuals with very low or very high long-term saturated fatty acid intakes(Reference Herrick, Rossen and Parsons36). Though most countries included participants aged 1 or 2 years onwards, in Brazil only participants aged 10 years and older were included. If as shown in other countries such as the US(Reference Baraldi, Steele, Canella and Monteiro37), children consume more UPFs than adults, UPF consumption, saturated fatty acids and thus, PAF, of the overall population may be underestimated in Brazil.
In addition, although all studies collected some information indicative of the type of processing to which foods were submitted before consumption or culinary preparation (i.e. place of meals and product brands), this information was not available for all food items, which could lead to modest over- or underestimation of UPF consumption. An additional source of error may be the use of combined foreign and national food composition tables in some countries (i.e. Brazil and Chile). Also, reformulation could have decreased saturated fatty acid content of UPFs since data collection, though the fact that associations persisted in studies with more recent data suggests that this is unlikely the case. Finally, PAFs need to be interpreted with caution especially because these are applied to population estimates and do not account for individual-level behaviour changes including food substitutions, replacements and abandonment effects associated with the reduction in UPF consumption.
In summary, the present study, carried out in nationally representative samples of the population of eight middle- and high-income countries, indicates that lowering the dietary contribution of UPFs to attainable, context-specific levels is a potentially effective way to reduce saturated fatty acid intake and the percentage of intakes with excessive content, which may play an important role in the prevention of NCDs, particularly cardiovascular diseases.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2021.30.
Acknowledgments
This work was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) [with grant numbers 2015/14900-9; 2016/14302-7; 2018/17972-9].
E. M. S., R. B. L. and C. A. M. formulated the research question and designed the study; E. M. S., C. B., G. C., M. L. C. L., N. K., P. M., J.-C. M. and F. R. analysed the data; E. M. S., C. B., G. C. M. L. C. L., N. K., P. M., J.-C. M., F. R., M. R. J., R. B. L. and C. A. M. wrote the article.
E. M. S., F. R. are beneficiaries of Postdoctoral Fellowship. Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) had no role in the design, analysis or writing of this article.
There are no conflicts of interest.









 Open access
Open access