



Introduction
Very preterm birth (VPT; birth before 32 weeks of gestation) includes approximately 1–2% of all births worldwide (Chawanpaiboon et al., Reference Chawanpaiboon, Vogel, Moller, Lumbiganon, Petzold, Hogan, Landoulsi, Jampathong, Kongwattanakul, Laopaiboon, Lewis, Rattanakanokchal, Ten, Thinkhamrop, Watananirun, Zhang, Zhou and Gülmezoglu2019), and has been associated with reduced brain volume, abnormalities in the brain structures which are particularly important for socio-emotional problems such as cerebral white matter and the prefrontal cortex (Volpe, Reference Volpe2009), as well as abnormalities in brain connectivity (Menegaux et al., Reference Menegaux, Meng, Bäuml, Berndt, Hedderich, Schmitz-Koep, Schneider, Nuttall, Zimmermann, Daamen, Zimmer, Boecker, Bartmann, Wolke and Sorg2021). There is increasing evidence that VPT birth is associated with later difficulties in several developmental domains (Bilgin et al., Reference Bilgin, Mendonca and Wolke2018; Heuser et al., Reference Heuser, Jaekel and Wolke2018; Montagna & Nosarti, Reference Montagna and Nosarti2016; Wolke et al., Reference Wolke, Johnson and Mendonça2019). In addition, VPT birth has been associated with a behavioral and personality phenotype including being timid, socially withdrawn and disinclined to take risks (Allin et al., Reference Allin, Rooney, Cuddy, Wyatt, Walshe, Rifkin and Murray2006; Montagna & Nosarti, Reference Montagna and Nosarti2016). These difficulties could predispose VPT children to be at an increased risk of emotional problems (Montagna & Nosarti, Reference Montagna and Nosarti2016; Wolke et al., Reference Wolke, Johnson and Mendonça2019), and an increased risk for peer victimization (Day et al., Reference Day, Van Lieshout, Vaillancourt and Schmidt2015; Nadeau et al., Reference Nadeau, Tessier, Lefebvre and Robaey2004; Wolke et al., Reference Wolke, Baumann, Strauss, Johnson and Marlow2015). Peer victimization refers to being exposed to hurtful acts of interpersonal aggression committed repeatedly by one or more peers which includes a power imbalance between the victim and the perpetrator (i.e., bully) (Copeland et al., Reference Copeland, Wolke, Angold and Costello2013).
There is evidence that individuals born VPT might be at a particular risk for emotional problems and peer victimization during adolescence (Bilgin, Brylka, et al., Reference Bilgin, Brylka, Wolke, Trower, Baumann and Lemola2021; Grindvik et al., Reference Grindvik, Hodøl, Vik, Evensen, Skranes, Brubakk and Indredavik2009; Johnson & Wolke, Reference Johnson and Wolke2013) given that it is a period of several physical, biological, and social transitions with peers and friendship relationships becoming increasingly important, and those born VPT might find it harder to master these transitions than those born full-term (FT) (Choudhury et al., Reference Choudhury, Blakemore and Charman2006). Nevertheless, many VPT born adolescents do not develop emotional problems or experience peer victimization. One factor which moderates the relationship between VPT birth and adolescence emotional problems, or experience peer victimization could be their self-control skills in childhood.
Self-control
One significant task for all children to accomplish is to be able to regulate and control their behaviors and emotions (Eisenberg et al., Reference Eisenberg, Spinrad and Eggum2010; Fergusson et al., Reference Fergusson, Boden and Horwood2013). This skill is often labeled as self-control which includes the individual’s capacity to change and regulate their responses leading to the inhibition of undesirable behaviors, thoughts, and emotions, while promoting the desired ones in order to attain long-term goals (Tangney et al., Reference Tangney, Baumeister and Boone2004). There are three types of self-control which are movement (i.e., the ability to manage body movements), emotional (i.e., the ability to manage feelings) and impulse control (i.e., the ability to stop and think before acting) (Bronson, Reference Bronson2000). The current study focuses on impulse control which allows individuals to see tasks through and think about the consequences of their actions and is closely related to effortful control. Thus, impulse control has both an attentional (i.e., the ability to shift and/or focus attention) and a behavioral aspect (i.e., the ability to think through before acting) (Moffitt et al., Reference Moffitt, Arseneault, Belsky, Dickson, Hancox, Harrington, Houts, Poulton, Roberts, Ross, Sears, Thomson and Caspi2011), which can be measured by observations and parent reports (Valiente et al., Reference Valiente, Eisenberg, Spinrad, Reiser, Cumberland, Losoya and Liew2006; Zentner & Bates, Reference Zentner and Bates2008; de Ridder et al., Reference de Ridder, Lensvelt-Mulders, Finkenauer, Stok and Baumeister2012).
Self-control emerges during the early years of life and develops rapidly until school age, and then continues to improve more slowly until adolescence (Kochanska et al., Reference Kochanska, Murray and Harlan2000). There is extensive evidence that several life-long outcomes depend on the level of self-control in childhood (Fergusson et al., Reference Fergusson, Boden and Horwood2013; Moffitt et al., Reference Moffitt, Arseneault, Belsky, Dickson, Hancox, Harrington, Houts, Poulton, Roberts, Ross, Sears, Thomson and Caspi2011; Tangney et al., Reference Tangney, Baumeister and Boone2004). For example, children with better self-control skills have better financial security, interpersonal relationships and academic performance, improved physical health, slower aging, and lower risk of externalizing problems, criminal behavior, and substance use during adulthood in comparison to those with lower self-control skills (Eisenberg et al., Reference Eisenberg, Spinrad and Eggum2010; Fergusson et al., Reference Fergusson, Boden and Horwood2013; Moffitt et al., Reference Moffitt, Arseneault, Belsky, Dickson, Hancox, Harrington, Houts, Poulton, Roberts, Ross, Sears, Thomson and Caspi2011; Tangney et al., Reference Tangney, Baumeister and Boone2004).
Moreover, it has been suggested that good self-control skills are associated with low levels of internalizing problems such as emotional problems (Robson et al., Reference Robson, Allen and Howard2020). Symptoms of emotional problems include problems with controlling one’s attention, cognition, and emotions (e.g., rumination) (Bernaras et al., Reference Bernaras, Jaureguizar and Garaigordobil2019). Having high self-control skills could help individuals to move their attention from negative thoughts and emotions to positive ones (Silk et al., Reference Silk, Steinberg and Morris2003). Thus, high self-control skills would help to attain desired outcomes, which may increase positive emotions and decrease negative ones (Eisenberg et al., Reference Eisenberg, Hofer, Vaughan and Gross2007).
In addition to emotional problems, self-control skills, particularly impulse control, have been reported to be associated with peer victimization (Arseneault et al., Reference Arseneault, Bowes and Shakoor2010). In a stressful situation such as victimization in peer context, children who have low impulse control might be more likely to take impulsive actions to alleviate distress such as reacting quickly to negative emotions and taking actions without consideration of consequences reflecting low social competence (Robson et al., Reference Robson, Allen and Howard2020). Moreover, they might be implementing less effective conflict management strategies such as responding to peer provocation with aggressive or withdrawn behaviors, which would increase their risk for peer victimization (Fogleman et al., Reference Fogleman, Slaughter, Rosen, Leaberry and Walerius2018). However, the existing limited number of studies were either cross-sectional or focused only on the childhood period (Robson et al., Reference Robson, Allen and Howard2020). Thus, it is unclear if high self-control skills in childhood is associated with low peer victimization in adolescence.
Very preterm birth and self-control
Few studies have investigated the role of self-control skills on emotional problems in the preterm (PT) population. One study including children born at or less than 35 weeks of gestation showed that higher effortful control was associated with lower levels of behavioral problems at 3 years of age, but this association was not significant when the analysis was adjusted for the role of socioeconomic factors such as parental education level (Burnson et al., Reference Burnson, Poehlmann and Schwichtenberg2013). Another study showed that PT children (<37 weeks of gestation) who had high levels of self-control (i.e., delayed gratification) at 24 months were more likely to have good peer relationships and fewer emotional problems at 6 years of age (Poehlmann-Tynan et al., Reference Poehlmann-Tynan, Gerstein, Burnson, Weymouth, Bolt, Maleck and Schwichtenberg2015). Existing studies on PT samples only focused on the role of self-control abilities on emotional outcomes during preschool years. It is unknown whether the positive effect of childhood self-control skills on emotional problems and peer victimization is still evident in adolescence in a VPT group.
Current study
To the best of our knowledge, this is the first study to investigate childhood self-control skills as a moderator of the association between VPT birth and adolescence emotional problems and peer victimization. The current study focuses on the sub-group of PT children who were born VPT as this group has been shown to be at highest risk for later emotional problems (Montagna & Nosarti, Reference Montagna and Nosarti2016). Further, associations between PT birth and peer victimization were shown particularly for VPT born children (Day et al., Reference Day, Van Lieshout, Vaillancourt and Schmidt2015). It has been suggested that PT birth could be an environmental sensitivity factor increasing the vulnerability to environmental factors, which could be both negative and positive (Lionetti et al., Reference Lionetti, Dellagiulia, Prudentino, Spinelli, Pluess and Fasolo2021). This means that PT children may be more negatively influenced by non-optimal environments than FT children, however, they may also benefit more from positive environments (Lionetti et al., Reference Lionetti, Dellagiulia, Prudentino, Spinelli, Pluess and Fasolo2021). The current study focuses on the positive influence of self-control skills which is in line with the vantage sensitivity model (Pluess & Belsky, Reference Pluess and Belsky2013). According to the vantage sensitivity model, there are differences between individuals regarding how much they benefit from positive experiences (de Villiers et al., Reference de Villiers, Lionetti and Pluess2018). In line with this model, it could be expected that self-control skills in childhood would benefit VPT adolescents more than FT adolescents in terms of emotional problems and peer victimization.
The current study undertakes a multi-cohort approach including prospective longitudinal data from four cohorts in three countries while accounting for the role of participants’ age at the assessment of the outcomes, sex, minority ethnicity, and the self-reported level of education of either parent at participants’ birth as a proxy for socioeconomic status. We have first conducted the analyses with the four cohorts separately and then combined their findings in an individual participant data (IPD) meta-analysis, which increases the statistical power and yields more reliable results compared to focusing on a single cohort (Fisher, Reference Fisher2015). In line with the previous research findings outlined above, we expected (1) a positive association between VPT birth and adolescence emotional problems and peer victimization, (2) a negative association between self-control skills in childhood and adolescence emotional problems and peer victimization suggesting that higher self-control skills in childhood will decrease both emotional problems and peer victimization in adolescence in VPT and FT groups in a similar manner, and (3) a significant interaction between VPT birth and self-control skills in childhood for adolescence emotional problems and peer victimization, suggesting that VPT born adolescents might benefit from good self-control skills more than FT born adolescents.
Method
The present study utilized data from four cohorts: The Avon Longitudinal Study of Parents and Children (ALSPAC; UK; 1991–1992); the Bavarian Longitudinal Study (BLS; Germany; 1985–1986); The Basel Study of Preterm Children (BSPC; Switzerland; 2001–2006); and the Millennium Cohort Study (MCS; UK; 2000–2002). Ethical approval for the present study was obtained from the Ethics Committee at the University of Warwick (reference 96/17-18).
Samples
The Avon Longitudinal Study of Parents and Children
ALSPAC is a UK birth cohort of 13,988 children, which has been described in detail elsewhere (Boyd et al., Reference Boyd, Golding, Macleod, Lawlor, Fraser, Henderson, Molloy, Ness, Ring and Davey Smith2013). ALSPAC recruited 14,541 pregnant women with expected delivery dates of 1st April 1991 to 31st December 1992. Of the initial pregnancies, there were 14,676 fetuses resulting in 14,062 live births; 13,988 children were alive at 1 year of age. A total of 13,978 children formed the original cohort. Ethical approval was obtained from the ALSPAC Law and Ethics committee and the local research ethics committee. Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time. From the first trimester of pregnancy, parents completed postal questionnaires about themselves and the study child. Children were invited to annual assessment clinics, including face-to-face interviews, and psychological and physical tests from 7 years onwards. The study website contains details of all data available through a fully searchable dictionary (http://www.bris.ac.uk/alspac/researchers/data-access/data-dictionary/). At 16 years assessment, information was available for 41 VPT and 4,253 FT participants.
Bavarian Longitudinal Study
BLS is a prospective geographically defined whole population sample of neonatal at-risk children born between January 1985 and March 1986 in Southern Bavaria (Germany) who required admission to a children’s hospital within the first 10 days after birth (N = 7,505) (Wolke et al., Reference Wolke, Ratschinski, Ohrt and Riegel1994). Of the 7,505 at-risk children, 682 were born very PT or very low birth weight. In addition, 916 healthy infants born at term in the same hospitals were recruited as controls. At 13 years, 451 very PT or very low birth weight and 350 control children were eligible for follow up. Ethical approval for the study was granted by the ethics committees of the University of Munich Children’s Hospital and the Bavarian Health Council. Informed consent was obtained from all participants.
Basel Study of Preterm Children
The BSPC is a cohort study of children who were born between June 2001 and December 2006. The PT sample was drawn from an initial cohort of 260 prematurely born children, who were treated after birth at the University Children’s Hospital of Basel (Maurer et al., Reference Maurer, Perkinson-Gloor, Stalder, Hagmann-von Arx, Brand, Holsboer-Trachsler, Wellmann, Grob, Weber and Lemola2016), while the FT sex- and age-matched control sample was recruited at an average of 8 years of age, based on official birth notifications. The initial sample included N = 108 PT and N = 106 FT born children, while data at 12 years of age was available for N = 74 PT and N = 81 FT born children. Detailed information on the sampling of the BSPC has been published previously (Maurer et al., Reference Maurer, Perkinson-Gloor, Stalder, Hagmann-von Arx, Brand, Holsboer-Trachsler, Wellmann, Grob, Weber and Lemola2016) and can be found here: https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/AYBAAN. Ethical approval and written informed consent were obtained (Ethikkommission Nordwest- und Zentralschweiz, reference number 122/11).
Millennium Cohort Study
MCS is a national birth cohort of 18,818 children born between September 2000 and January 2002 in England, Wales, Scotland, and Northern Ireland (Connelly & Platt, Reference Connelly and Platt2014). The first sweep of interviews with cohort members’ mothers took place when the infants were 9 months old, and 7 sweeps have been completed so far. The interviews included questions on a wide variety of topics, including health, education, social, family, and economic status of the cohort members’ households. Detailed information on the sampling and scope of MCS is available at: http://www.cls.ioe.ac.uk/. Ethical approval and written informed consent for all participants were obtained (London – Hampstead Research Ethics Committee, REC reference 14/LO/0868). At 14 years assessment, information was available for 106 VPT and 9537 FT participants.
Measures
Very preterm birth
Gestational age in full weeks plus days was extracted from medical records. The continuous variable was recoded into a categorical variable with the following categories: 0 = FT (37–41 completed weeks of gestation); 1 = VPT (<32 completed weeks of gestation).
Self-control in childhood
In ALSPAC, BSPC and MCS, mother-reported self-control in childhood was measured using the Strengths and Difficulties Questionnaire (SDQ) (Goodman, Reference Goodman1997), which is a 25-item rating scale with five subscales: Emotional symptoms, conduct problems, inattention or hyperactivity, peer problems and prosocial behavior. The inattention or hyperactivity subscale includes the following two items that reflect self-control similar to items included in other large-scale prospective studies (Howard & Williams, Reference Howard and Williams2018; Moffitt et al., Reference Moffitt, Arseneault, Belsky, Dickson, Hancox, Harrington, Houts, Poulton, Roberts, Ross, Sears, Thomson and Caspi2011): “child thinks things out before acting” and “child sees tasks through to the end and has good attention span.” The items are rated on a three-point scale: 0 = Not true; 1 = Somewhat true; 2 = Certainly true. In BLS, mothers reported on self-control using the effortful control subscale of Emotionality, Activity, Sociability Temperament Assessment (Reyes et al., Reference Reyes, Jaekel, Kreppner, Wolke and Sonuga-Barke2020). The effortful control subscale included the following three items: “switches toys often,” “gives up quickly if a game is difficult” and “gives up quickly when s/he struggles with difficulties.” The reliability scores of the effortful control were α = .82 at 6 years and α = .81 at 8 years assessment. Mothers reported on self-control at three time points across childhood: preschool (5–6 years; ALSPAC, BLS, MCS), middle childhood (7–9 years; ALSPAC, BLS, BSPC, MCS) and late childhood (10–11 years; ALSPAC, BSPC, MCS). Scores were aggregated across these time points (i.e., summed up across two time points for BLS and BSPC and three time points for ALSPAC and MCS) within each cohort to create a composite score for each cohort. Afterwards, the aggregated scores were z-standardized to harmonize the data across cohorts. Higher scores reflect higher levels of self-control.
Emotional problems in adolescence
In ALSPAC at 16 years and in MCS at 14 years, participants reported on their emotional problems using the short version of the Moods and Feelings Questionnaire (Angold et al., Reference Angold, Costello, Messer and Pickles1995), which is a widely used questionnaire to assess depressive symptoms over the last two weeks on a three-point scale (0 = Not true, 1 = Sometimes true, 2 = True) with good reliability and validity (Rhew et al., Reference Rhew, Simpson, Tracy, Lymp, McCauley, Tsuang and Stoep2010; Turner et al., Reference Turner, Joinson, Peters, Wiles and Lewis2014). In BSPC, participants reported on their emotional problems using the eight-item Child Depression Screener (ChilD-S) (Frühe et al., Reference Frühe, Allgaier, Pietsch, Baethmann, Peters, Kellnar, Heep, Burdach, von Schweinitz and Schulte-Körne2012) at 12 years, which has good validity and assesses depressive symptoms over the last two weeks. The response scale ranged from 0 = None of the time to 3 = Most or all the time. In BLS, participants reported on their emotional problems using the emotional problems subscale of the SDQ (Goodman, Reference Goodman1997) at 13 years of age. The emotional problems subscale of the SDQ includes five items on a three-point response scale (0 = Not true, 1 = Somewhat true, 2 = Certainly true). The reliability scores ranged from good to high across all cohorts (ALSPAC: α = .91; BLS; α = .70; BSPC; α = .77; MCS; α = .93).
In addition to participants’ self-reports, mothers reported on the emotional problems of their adolescents using the emotional problems subscale of the SDQ (Goodman, Reference Goodman1997) in all cohorts. The reliability scores were good across all cohorts (ALSPAC: α = .71; BLS; α = .72; BSPC; α = .70; MCS; α = .73).
Peer victimization in adolescence
In ALSPAC, participants reported on peer victimization via the Bullying and Friendship Interview Schedule at 13 years of age (Zwierzynska et al., Reference Zwierzynska, Wolke and Lereya2013). Frequency of being bullied was rated on a 4-point scale (0 = Never, 1 = Seldom, 2 = Frequently, 3 = Very frequently) across five types of overt bullying (theft, threats or blackmail, physical violence, nasty names, nasty tricks), and four types of relational bullying (social exclusion, spreading lies or rumors, coercive behavior, deliberately spoiling games). The reliability of this scale was good (α = .73). In BLS, participants reported on peer victimization with one item from the SDQ at 13 years of age (Goodman, Reference Goodman1997; Wolke et al., Reference Wolke, Baumann, Strauss, Johnson and Marlow2015): “Other children pick on or bully me.” In BSPC, participants reported on peer victimization at 12 years with the following three items of the KIDSCREEN-52 (Herdman et al., Reference Herdman, Rajmil, Ravens-Sieberer, Bullinger, Power and Alonso2002), which is a valid and reliable measure of quality of life: “Have you been afraid of other girls and boys?” “Have other girls and boys made fun of you?” “Have other girls and boys bullied you?” The answering scale was a five-point Likert-type scale (0 = Never, 1 = Seldom, 2 = Sometimes, 3 = Often, 4 = Always). The reliability of this scale was low but acceptable for a scale with three items (α = .52). In MCS, participants reported on peer victimization with the following one item at 14 years: “How often other children hurt or pick on you?” The response scale ranged from 1 = Never to 6 = Most days. In addition, mothers reported on peer victimization using the following one item from SDQ in all cohorts: “Picked on or bullied by other children.”
Covariates
The following covariates were used in the analysis: participants’ age at the assessment of the outcomes, sex, minority ethnicity, and the self-reported highest level of education of either parent at participants’ birth as a proxy for socioeconomic status. Ethnic minority group membership was measured as the adolescents’ first language (0 = German; 1 = Other) in the BSPC and BLS, and with parent-reported ethnic minority status (0 = White British; 1 = Other) in ALSPAC and MCS. Parental education was defined by the highest educational level of either parent (0 = Obligatory education or lower; 1 = A level or vocational equivalent or higher education or university degree).
Statistical analysis
Missing data strategy
Sampling weights were applied to the analyses of MCS data to account for the stratified clustered design of the data and the oversampling of subgroups. Sampling weights were not required for the other three cohorts. Missing data in all analyses was accounted for with multiple imputation using chained equations with the "mi" command in Stata. Each data set was imputed 20 times.
Main analyses
All statistical analyses were conducted with Stata, version 15.0 (StataCorp, 2017) in two steps. In the first step, we conducted hierarchical regression analyses where we added the variables into the regression using the following three steps following the procedure of Aiken and West (Reference Aiken and West1991): (1) covariates (participants’ age at the assessment of the outcomes, sex, minority ethnicity, and the self-reported highest level of education of either parent at participants’ birth) and VPT; (2) self-control; and (3) interaction term between VPT and self-control. The analyses were repeated for the two outcome variables (i.e., emotional problems and peer victimization) and separately for self- and mother-reports. Outcome variables and self-control were standardized for comparisons across cohorts.
In the second step, the results from the individual cohorts regarding the main effects of VPT and self-control, as well as the interaction effect between VPT and self-control were combined in IPD meta-analyses using the "ipdmetan" command in Stata (Fisher, Reference Fisher2015). The DerSimonian and Laird procedure was used to compute the pooled effects and 95% confidence intervals (CIs). Between-study heterogeneity was tested using the Cochran’s Q statistic and quantified by the I2 value as follows: low heterogeneity when I2 < 25%; moderate heterogeneity when 25% < I2 < 75%; and high heterogeneity when I2 > 75%.
Sensitivity analyses
Two sets of sensitivity analyses were conducted. First, the main analyses were repeated after excluding participants with neurosensory impairment considering the possible influence of neurosensory impairment on emotional problems and peer victimization (Sentenac et al., Reference Sentenac, Gavin, Gabhainn, Molcho, Due, Ravens-Sieberer, Matos, Malkowska-Szkutnik, Gobina, Vollebergh, Arnaud and Godeau2013). Neurosensory impairment was either extracted from medical records or parent-reported and indicated by the presence of either (a) an IQ score for fluid reasoning of 3SDs below the mean identified between 5–11 years, (b) parent- or school-reported visual or hearing impairment, or (c) severe congenital malformations identified during the child’s first year of life. Second, the main analyses were repeated using data without imputation to examine whether drop-out resulted in biased findings.
Results
Characteristics of the participants in four cohorts are presented in Table 1. Self-control of VPT children was lower than self-control of FT children in mother-reports (p < .05), except in the ALSPAC cohort. There were no significant differences between VPT and FT groups in self-reported emotional problems in adolescence in any cohorts. However, VPT born adolescents had higher scores of mother-reported emotional problems in comparison to FT born adolescents in BLS and MCS cohorts.
Table 1. Characteristics of very preterm and full-term children in four cohorts

ALSPAC: Avon Longitudinal Study of Parents and Children; BLS: Bavarian Longitudinal Study; BSPC: Basel Study of Preterm Children; MCS: Millennium Cohort Study. VPT: Very preterm (<32nd gestational week); FT: Full-term (≥37th gestational week).
a Please note that the age at assessment for the ALSPAC cohort is very similar for each participant with only a couple of weeks difference.
VPT born adolescents in the BLS cohort had higher self- and mother-reported peer victimization scores in comparison to FT born adolescents (p < .001), whereas there were no significant differences between the two groups in the other cohorts. Bivariate correlations between study variables are presented separately for each cohort in Tables S1a–d in the supplement.
Associations between very preterm birth, self-control in childhood and self- and mother-reported emotional problems in adolescence
Results of the hierarchical regression analyses for all cohorts are displayed in Table S2 in the supplement. Findings of the IPD meta-analysis showed no significant associations between VPT birth and self-reported emotional problems, however there was a significant association between VPT birth and mother-reported emotional problems in adolescence (β = .13; 95% CI = .01; .24) (Figure 1). Moreover, there was a significant negative association between self-control in childhood and emotional problems in adolescence in self-reports (β = −.11; 95% CI = −.16; −.06), and mother-reports (β = −.22; 95% CI = −.34; −.11) among all participants. On the other hand, there was no significant interaction effect between VPT birth and self-control skills in childhood on self- and mother-reported emotional problems in adolescence (Figure 1). There was a significant moderate to high heterogeneity (Table S3 in the supplement) between cohorts in the analysis of the association between self-control in childhood and self- and mother-reported emotional problems (I 2 = 64.9, p < .05; I 2 = 95.9, p < .001, respectively). Findings remained the same when the analyses were repeated excluding participants with neurosensory impairment (Table S4 in the supplement) and without data imputation (Table S5 in the supplement).
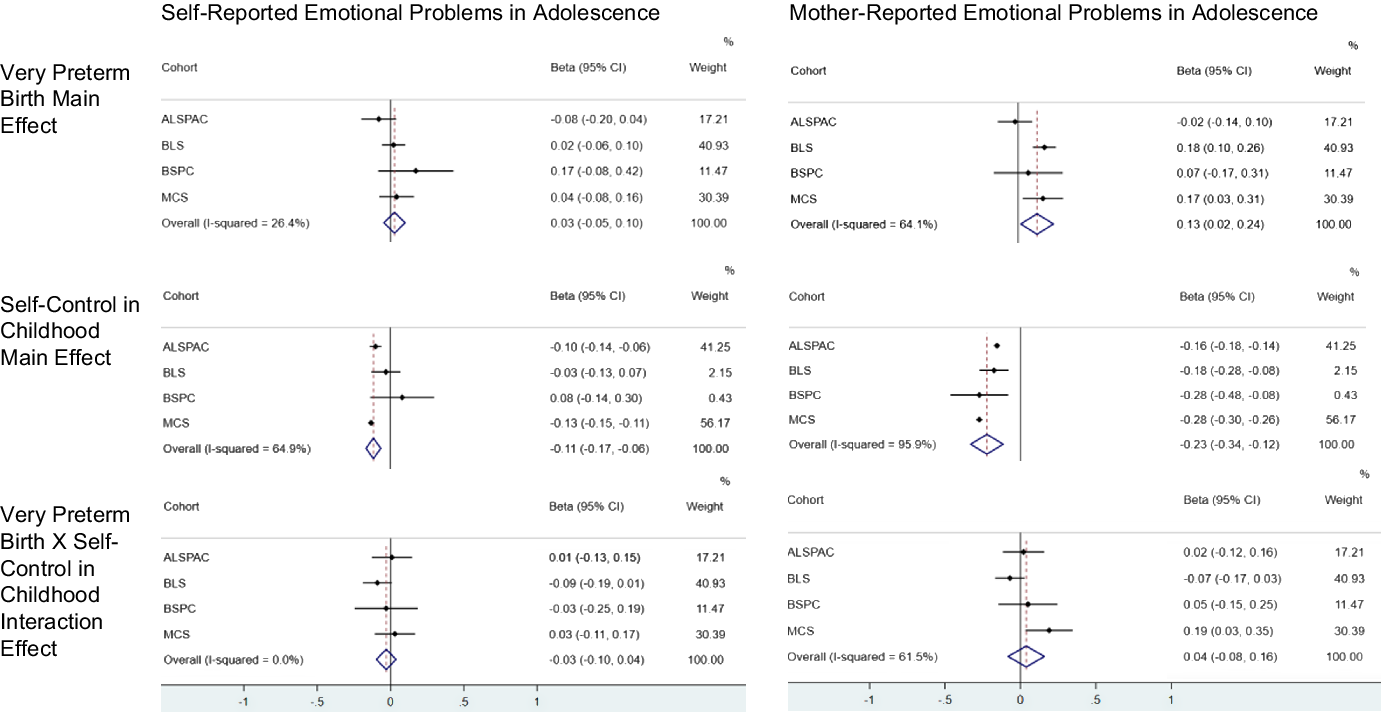
Figure 1. Findings of the individual participant data meta-analysis on the associations between very preterm birth, self-control, and emotional problems in adolescence.
Associations between very preterm birth, self-control in childhood, and self- and mother-reported peer victimization in adolescence
Results of the hierarchical regression analyses for all cohorts are displayed in Table S6 in the supplement. Findings of the IPD meta-analysis did not yield significant associations between VPT birth and self-reported peer victimization in adolescence, however, there was a significant association between VPT birth and mother-reported peer victimization in adolescence (β = .13; 95% CI = .06; .20) (Figure 2). In addition, IPD meta-analysis revealed a significant negative association between self-control in childhood and both self-reported (β = −.13; 95% CI = −.18; −.09) and mother-reported peer victimization in adolescence (β = −.24; 95% CI = −.33; −.14). There was no significant interaction effect between VPT and self-control on self- and mother-reported peer victimization in adolescence (Figure 2). There was significant heterogeneity between the cohorts in the analysis for mother-reported peer victimization (I 2 = 94.3, p < .001) but not in self-reported peer victimization (Table S3 in the supplement). The association between VPT birth and mother-reported peer victimization disappeared when the analyses were repeated excluding participants with neurosensory impairment (Table S4 in the supplement) and using data without imputation (Table S5 in the supplement). Moreover, the association between self-control skills and mother-reported peer victimization disappeared when the analyses were repeated excluding participants with neurosensory impairment (Table S4 in the supplement).

Figure 2. Findings of the individual participant data meta-analysis on the associations between very preterm birth, self-control, and peer victimization in adolescence.
Discussion
Findings of this prospective, multi-cohort and multi-informant study revealed that higher self-control skills in childhood are associated with fewer emotional problems and reduced peer victimization in both VPT and FT born adolescents. However, self-control skills in childhood did not moderate the association between VPT birth and adolescence emotional problems and peer victimization. These findings provide no evidence for a vantage sensitivity model; however, the findings show support for a protective effect model for both groups of adolescents.
The main finding of the current study was that having higher self-control skills does not particularly benefit VPT born adolescents more than those born FT, however high self-control skills in childhood are associated with lower emotional problems and peer victimization in adolescence in both groups. This finding is in line with the results of a recent meta-analysis study showing a negative association between childhood self-control and consequent internalizing problems and peer victimization (Robson et al., Reference Robson, Allen and Howard2020). The results, regarding the link between self-control in childhood and emotional problems in adolescence, were consistent in both self- and mother-reports and is also consistent with the self-control model of depression suggesting that deficits in self-control processes play a key role in understanding the development of depressive symptoms (Rehm, Reference Rehm1977). Furthermore, this result accords with intervention studies that showed that increasing the self-control skills of individuals is effective in decreasing symptoms of depression (Strauman & Eddington, Reference Strauman and Eddington2017). Our results revealed self-control skills in childhood are a protective factor against self- or mother-reported peer victimization. This provides further support for the self-control theory, which suggests that low self-control skills put individuals at risk for victimization since those with low self-control skills may be less likely to consider later consequences than those who have high self-control skills (Gottfredson & Hirschi, Reference Gottfredson and Hirschi1990). Thus, having higher self-control skills is a protective factor in both VPT and FT born adolescents regarding emotional problems and peer victimization.
Although self-control skills in childhood have been identified as a resiliency factor in community samples in the face of growing up with disadvantage and adversity (Masten, Reference Masten2001), few studies have investigated the role of childhood self-control skills on later socio-emotional outcomes in a PT sample. One study (Poehlmann-Tynan et al., Reference Poehlmann-Tynan, Gerstein, Burnson, Weymouth, Bolt, Maleck and Schwichtenberg2015) identified delay of gratification at 2 years of age as a resiliency factor in 6-year-old PT children. In this study, resiliency was identified using a latent profile analysis approach where a resilient group was defined based on their score across several domains (e.g., learning, effortful control, social activity, peer relationships, internalizing behavior). However, the effect size of the influence of delay of gratification on resiliency was very small (β = .06). In another study, the association between effortful control and behavioral problems at 3 years of age diminished when the role of socioeconomic factors was considered (Burnson et al., Reference Burnson, Poehlmann and Schwichtenberg2013). Considering these findings, it can be suggested that there is not yet strong evidence for the resiliency effect of self-control skills in particular to PT adolescents regarding emotional problems and peer victimization. Regarding resiliency, that is, the interaction of VPT birth as risk with other protective factors such as high maternal sensitivity and low negative parenting (i.e., anger, criticism) could play a bigger role than self-control skills in childhood (Faure et al., Reference Faure, Habersaat, Harari, Müller-Nix, Borghini, Ansermet, Tolsa and Urben2017; Wolke et al., Reference Wolke, Jaekel, Hall and Baumann2013).
There was a significant association between VPT birth and increased emotional problems and peer victimization in adolescence in mother-reports, but this was not evident in self-reports. This finding is in line with previous studies showing low agreement in reports of emotional and behavioral problems between parent and child reports in PT samples (Bilgin, Wolke, et al., Reference Bilgin, Wolke, Baumann, Trower, Brylka, Räikkönen, Heinonen, Kajantie, Schnitzlein and Lemola2021; Eves et al., Reference Eves, von Mühlenen, Mendonça, Johnson, O’Reilly, Bartmann, Marlow and Wolke2020). This finding could be due to adolescents under-reporting their symptoms of emotional problems and peer victimization (Lærum et al., Reference Lærum, Reitan, Evensen, Lydersen, Brubakk, Skranes and Indredavik2019). Alternatively, mothers of VPT born adolescents might have a tendency to report more emotional and behavioral problems than VPT adolescents themselves due to their perception of increased vulnerability (Allen et al., Reference Allen, Manuel, Legault, Naughton, Pivor and O’Shea2004). This could be due to PT birth being an emotionally challenging event as it is often unexpected and associated with a higher risk of medical complications and neonatal difficulties (Horwitz et al., Reference Horwitz, Storfer-Isser, Kerker, Lilo, Leibovitz, St John and Shaw2015). It has been suggested that mothers might continue to perceive their premature born child as vulnerable beyond the infancy period, which could result in overprotective parenting (Horwitz et al., Reference Horwitz, Storfer-Isser, Kerker, Lilo, Leibovitz, St John and Shaw2015). Although there is evidence that maternal sensitive parenting is not influenced by PT birth (Bilgin & Wolke, Reference Bilgin and Wolke2015), overprotective and controlling parenting behaviors in mothers of PT born children have been recently documented (Faleschini et al., Reference Faleschini, Matte-Gagné, Luu, Côté, Tremblay and Boivin2020). Thus, it would be important to include the assessment of other informants such as fathers in future studies.
The sensitivity analyses excluding participants with neurosensory impairment or using data imputation reproduced the same findings regarding the association of self-control and emotional problems in adolescence. However, there were changes in the association between VPT birth and mother-reported peer victimization in adolescence. Moreover, the association between self-control skills in childhood and mother-reported peer victimization in adolescence disappeared when we repeated the main analyses without participants with neurosensory impairment. These changes suggest that having neurosensory impairment could influence mother-reports particularly for peer victimization in adolescence. This is in line with the findings of a study which found that adolescents with disability or chronic illness are at an higher risk of victimization than those without disability or chronic illness given that disability or chronic illness is much more frequent in the VPT group (Sentenac et al., Reference Sentenac, Gavin, Arnaud, Molcho, Godeau and Nic Gabhainn2011).
There are several strengths of the current longitudinal study including the large sample size combining IPD across four cohorts, high power to detect statistically significant differences, the use of multiple imputation to account for missing data, as well as using both self- and mother-reports of emotional problems and peer victimization in adolescence. A further strength of the current study was being able to control for the same covariates across cohorts. Moreover, self-control skills in childhood were aggregated across three assessment points in childhood. However, there are also limitations. First, pubertal timing was not included as a covariate in the current study, which could have an influence on our findings due to its link with mental health problems (Graber et al., Reference Graber, Lewinsohn, Seeley and Brooks-Gunn1997). However, we could not include pubertal timing as a covariate since it was not measured across all cohorts. Second, self-control in childhood was assessed with parental reports using two items from SDQ in three of the cohorts (i.e., ALSPAC, BSPC, MCS), which reflects impulse control only. Thus, the measurement of self-control in the current study captures one aspect of self-control and might be more prone to social desirability bias than task-based assessments of self-control. It would have been preferable to measure self-control with a multi-informant assessment (e.g., mother, father and teacher-reports) using multi-methods (a self-control questionnaire and task-based assessment). However, parental reports of self-control are commonly used in large-scale prospective longitudinal studies due to practicality and they are likely to have better ecological validity than task-based assessments of self-control (Howard & Williams, Reference Howard and Williams2018; Moffitt et al., Reference Moffitt, Arseneault, Belsky, Dickson, Hancox, Harrington, Houts, Poulton, Roberts, Ross, Sears, Thomson and Caspi2011). Further, it was shown that questionnaire-based assessments of self-control have higher test-retest reliability than task-based assessments (Enkavi et al., Reference Enkavi, Eisenberg, Bissett, Mazza, MacKinnon, Marsch and Poldrack2019). Third, there was moderate to high heterogeneity between the cohorts for some of the IPD meta-analyses even though it was statistically not significant for all associations. This suggests that differences between either the scales or the cohorts (e.g., differences between countries) might have had an impact on the results. It is important to note that participants in two of the samples (i.e., ALSPAC and BLS) were recruited before the year 2000 and changes in neonatal care are likely to have led to more PT children surviving in the most recent cohorts (i.e., BSPC and MCS) who were recruited in the 2000s. Although there is little evidence that the quality of survival has improved (Cheong et al., Reference Cheong, Spittle, Burnett, Anderson and Doyle2020; Marlow et al., Reference Marlow, Ni, Lancaster, Suonpera, Bernardi, Fahy, Larsen, Trickett, Hurst, Morris, Wolke and Johnson2021; Ni et al., Reference Ni, Johnson, Marlow and Wolke2022), changes in care may have contributed to the heterogeneity across cohorts.
To conclude, self-control skills in childhood are a protective factor for the development of emotional problems and peer victimization for all children whether born VPT or FT. Thus, improving the self-control skills of VPT and FT children would benefit them equally and could help to decrease emotional problems and peer victimization in adolescence.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579422001201
Funding statement
This study has received funding from The Economic and Social Research Council New Opportunities for Research Funding Agency Co-operation in Europe (NORFACE), for Life Course Dynamics after Preterm Birth: Protective Factors for Social and Educational Transitions, Health, and Prosperity, under grant number 462-16-040.
Conflict of interest
The authors have no conflicts of interest to disclose.






 Open access
Open access