


Much evidence shows that lone mothers have poorer mental health than partnered mothers. Although this is often linked to their greater economic hardship (Reference Hope, Power and RodgersHope et al, 1999), other factors have been investigated. Lone mothers report higher rates of childhood abuse (Reference Bifulco, Brown and AlderBifulco et al, 1991) and this may account for their greater prevalence of anxiety and depressive disorders (Reference Lipman, McMillan and BoyleLipman et al, 2001). There is growing recognition of the extent and consequences of violence against women (Reference Watts and ZimmermanWatts & Zimmerman, 2002). This study examines lifetime experience of physical and sexual violence to index a range of traumatic experiences significant to lone mothers, including childhood abuse (Reference Lipman, McMillan and BoyleLipman et al, 2001) and domestic violence (Reference KurzKurz, 1996). The study uses a large national data-set to examine whether lone mothers have greater lifetime experience of physical or sexual violence than partnered mothers; whether greater exposure to such trauma accounts for the poorer mental health of lone mothers; and whether there is a pattern between the types of trauma experienced and different mental health outcomes.
METHOD
Sample
The National Survey of Mental Health and Wellbeing was conducted by the Australian Bureau of Statistics in 1997. The survey was designed to provide data on the prevalence of common mental disorders, disability and health service usage in Australia. It used a representative sample of persons living in private dwellings from all Australian States and Territories. About 13 600 households were approached, with one person aged 18 years or over from each house randomly selected for interview. Overall, 10641 individuals completed the survey (a 78% response rate). The sample was weighted based on State, part-of-State, age, gender and probability of selection to match the overall Australian population.
Measures
The primary diagnostic component of the survey was a computerised version of the Composite International Diagnostic Interview (CIDI), Version 2.1 (Reference Andrews and PetersAndrews & Peters, 1998). The data reported in this paper use the ICD–10 (World Health Organization, 1992) to examine the presence of any anxiety disorder, any affective disorder and harmful alcohol or drug use or dependence within the 12 months prior to interview.
Four questions from the post-traumatic stress disorder module of the CIDI assessing lifetime experience of traumatic events provided measures of physical and sexual violence (Table 1). In addition, a question related to experience of a natural disaster was examined to assess potential response bias.
Table 1 Measures of traumatic experiences, including physical and sexual violence and natural disasters
| Sexual molestation | Were you ever sexually molested? That is, someone touched your genitals when you did not want that person to. |
| Rape | Were you ever raped? That is, someone had sexual intercourse with you when you did not want to by threatening you or using some degree of force. |
| Physical attack | Were you ever seriously physically attacked or assaulted? |
| Threatened with weapon | Have you ever been threatened with a weapon, held captive or kidnapped, or have you ever been tortured or the victim of terrorists? |
| Natural disaster | Were you ever involved in a fire, flood or other natural disaster? |
The survey included the K10 scale to enable the measurement of psychological distress (including subclinical distress) within the past 4 weeks (Reference Kessler, Andrews and ColpeKessler et al, 2002). The scale produces scores within the range 10–50, with a higher score indicating greater distress. Respondents with a score of 20 or greater were classified with a substantial level of psychological distress.
This analysis also assessed a range of socio-demographic information, including age, gender, marital status, labour force status, housing tenure (renting or other) and educational attainment (completed secondary school). Women who reported that government pensions or allowances were their main source of income were classified as income support/welfare recipients. Given Australia's highly targeted, non-contributory welfare system, receipt is a strong indicator of low income and is used as a proxy for financial circumstances. The Australian Bureau of Statistics derived an index of relative social disadvantage that reflects the socio-economic circumstances of geographical areas. Individuals were categorised as living in a low socioeconomic area if their residence was classified in the lowest two quintiles.
Analysis
This analysis explored the mental health of, and physical and sexual violence experienced by, partnered and unpartnered mothers. The identification of women with children was based on report of having ever had a child and reported presence of a child aged under 17 years in the household. To avoid outliers, the analysis was restricted to women under the age of 60 years (excluding 13 partnered and 16 unpartnered women with children). Partnered status was based on reported current marital status. Partnered women were those identified as married or in a de facto relationship, whereas unpartnered women were those who were separated, divorced, widowed or never married.
The association between partnered status and various socio-demographic characteristics was examined using logistic regression analysis, with odds ratios and 95% confidence intervals demonstrating the strength of relationship. The prevalence of physical and sexual violence, psychiatric disorders and psychological distress among lone and partnered mothers was calculated. Again, the relationship between partnered status and each of these variables was examined using logistic regression analyses. Similar analyses compared the different categories within the partnered (married and de facto) and lone mother (separated, divorced, widowed and never married) groups.
A series of univariate and multiple logistic regression analyses was used to assess the relationship between various predictors (partnered status, socio-demographic variables and experience of physical and sexual violence) and the mental health measures. Odds ratios and 95% confidence intervals were used to assess the total and unique contribution of individual measures. To assess the extent to which the effects of lone parent status were mediated by the socio-demographic and physical and sexual violence measures, the ‘explained fraction’ approach (ORa–1)–(ORb–1)/(ORa–1) (Reference Whitehead, Burström and DiderichsenWhitehead et al, 2000) was used. Analyses compared the odds ratios for lone parent status before and following the addition of the mediating variables (considering the mediating effect of socio-demographic characteristics alone, experience of physical or sexual violence alone and the combined effect of both of these sets of measures).
The relative importance of the blocks of socio-demographic and trauma variables was assessed by examining the significance of the change in the log-likelihood brought about by the addition of groups of variables to the constant-only model (total predictive power) or the exclusion of blocks of variables from the full model (unique prediction).
Statistical analyses were conducted using the Statistical Package for the Social Sciences, version 11 and STATA, both for Windows. For the logistic regression models, jack-knife replicate weights included in the Australian Bureau of Statistics data-set were used to derive standard errors and confidence intervals.
RESULTS
Table 2 presents data on the socio-economic circumstances of lone and partnered mothers. Lone mothers were more likely to live in lower socio-economic areas, to receive income support/welfare payments and to be renting (rather than owning or purchasing their own home).
Table 2 Socio-demographic characteristics
| Lone mothers (n=662) | Partnered mothers (n=1610) | Odds ratio | 95% CI | |
|---|---|---|---|---|
| Rental housing | 61.5% | 18.0% | 7.31 | 5.83-9.17 |
| Not completed secondary school | 67.1% | 54.6% | 1.71 | 1.44-2.03 |
| Resides in low socio-economic area | 50.8% | 30.0% | 2.42 | 1.54-3.8 |
| Not employed | 48.0% | 37.4% | 1.56 | 1.28-1.89 |
| Receiving income support/welfare | 63.2% | 26.0% | 4.90 | 3.88-6.17 |
The prevalence of substantial psychological distress and common psychiatric disorders was higher among unpartnered compared with partnered mothers (Fig. 1). The odds ratios were > 2 for each outcome measure. Overall, 27.5% of respondents experienced at least one form of common mental disorder or substantial psychological distress, with unpartnered mothers having significantly greater prevalence than partnered mothers (44.9% of lone and 23.6% of partnered mothers; odds ratio=2.66, 95% CI 2.07–3.40).
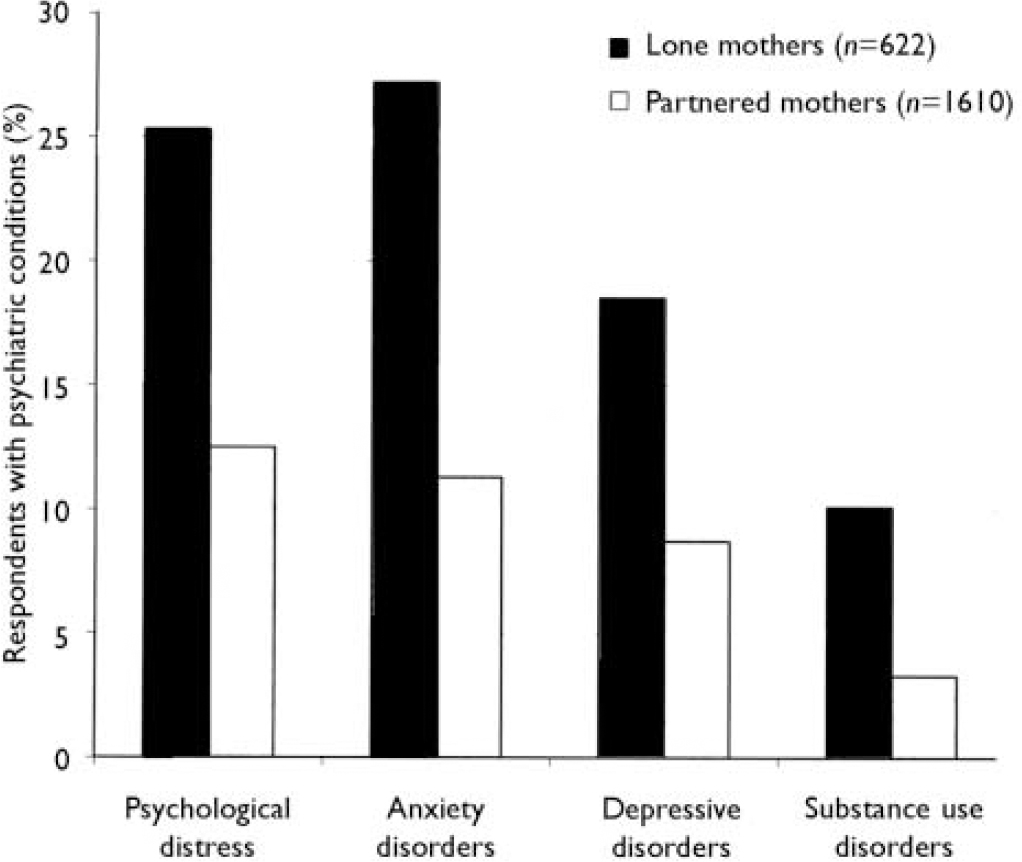
Fig. 1 Prevalence of mental disorders and substantial psychological distress (K10≥20) among lone and partnered mothers.
Data on the prevalence of lone and partnered mothers’ experience of physical and sexual violence are presented in Fig. 2. Lone mothers were significantly more likely to have experienced rape, sexual molestation, severe physical assault or to have been threatened with a weapon or tortured compared with partnered mothers, with odds ratios of >3. Overall, 19.6% of partnered mothers reported an experience of violence, whereas 45.1% of lone mothers reported at least one of these forms of physical and sexual violence (odds ratio=3.41, 95% CI 2.57–4.52). In contrast, lone and partnered mothers did not differ in their reported experience of natural disasters.
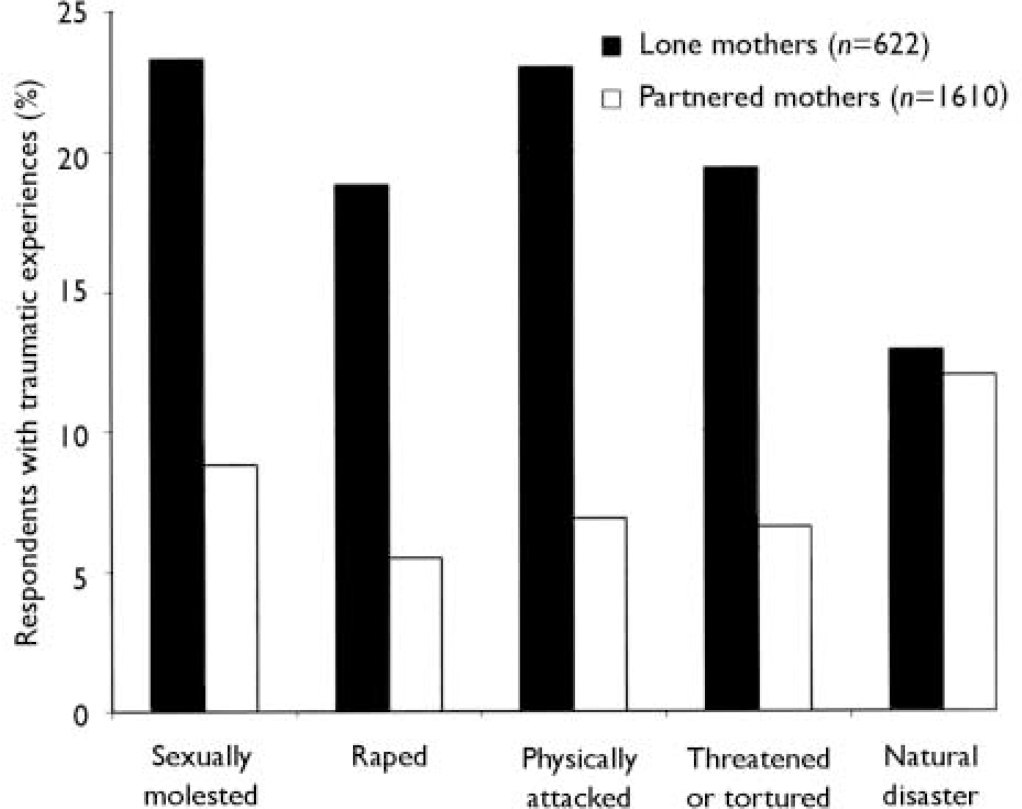
Fig. 2 Prevalence of traumatic experiences (particularly physical and sexual violence) among lone and partnered mothers.
There were consistent differences between the two categories of partnered mothers, with those in de facto relationships consistently reporting higher rates of psychiatric disorders and experience of violence than married mothers. There were, however, no significant differences between the different categories of unpartnered mothers. Although those who were widowed reported lower levels of violence, this was a very small subgroup. The ‘never married’ group did not differ substantially from the other categories of unpartnered mothers across the mental health or violence measures, and within the ‘never married’ category there was little difference between those who reported a previous de facto relationship and those who reported neither a previous marriage nor a de facto relationship.
Table 3 shows the relationships of the measures of lone parent status, sociodemographic characteristics and different forms of physical and sexual violence with the mental health variables for both univariate and simultaneous logistic regression models. The univariate results show that the individual measures of physical and sexual violence were more strongly associated with mental health than were lone parent status or socio-demographic characteristics. The odds ratios for each of the violence measures were all >3 for anxiety, substance use and psychological distress. The association between experience of serious physical attack or assault and the prevalence of anxiety disorders was greatest, with an odds ratio >5. All of the relationships with depression were somewhat less pronounced, but the odds ratios for rape and physical attack were ∼3. Although not as strongly associated as these trauma measures, a number of the sociodemographic characteristics were also significantly associated with psychiatric disorders, the strongest predictors being rental housing and welfare receipt.
Table 3 Logistic regression analyses for each of the mental health measures as a function of lone parent status, socio-demographic measures and measures of physical and sexual violence
| Affective disorder Odds ratio (95% CI) | Anxiety disorder Odds ratio (95% CI) | Substance use disorder Odds ratio (95% CI) | Psychological distress Odds ratio (95% CI) | |
|---|---|---|---|---|
| Univariate results | ||||
| Lone parent status | 2.36 (1.57-3.56) | 3.00 (2.32-3.77) | 3.35 (2.14-5.26) | 2.37 (1.78-3.16) |
| Socio-demographic | ||||
| Low SES area | 1.22 (0.93-1.59) | 1.51 (1.07-2.13) | 1.22 (0.61-2.47) | 1.59 (1.24-2.06) |
| Rental housing | 1.78 (1.25-2.53) | 2.14 (1.66-2.74) | 2.96 (1.67-5.27) | 1.94 (1.53-2.47) |
| Reliant on welfare | 1.54 (1.19-1.99) | 1.98 (1.43-2.76) | 2.20 (1.52-3.20) | 2.22 (1.73-2.85) |
| Not employed | 1.31 (0.98-1.76) | 1.69 (1.26-2.25) | 1.13 (0.73-1.74) | 1.88 (1.43-2.48) |
| Not completed high school | 1.83 (1.23-2.72) | 1.65 (1.20-2.28) | 1.38 (0.96-1.99) | 1.50 (1.18-1.91) |
| Number of children | 1.12 (0.99-1.27) | 1.20 (1.04-1.37) | 0.91 (0.63-1.31) | 1.20 (1.05-1.36) |
| Physical and sexual violence | ||||
| Sexual molestation | 2.36 (1.68-3.31) | 3.57 (2.55-5.00) | 3.63 (1.71-7.74) | 2.21 (1.48-3.30) |
| Rape | 2.87 (1.82-4.53) | 4.03 (2.75-5.89) | 3.64 (2.10-6.30) | 3.73 (2.76-5.03) |
| Physical attack | 2.89 (2.01-4.15) | 5.15 (3.96-6.70) | 4.44 (2.62-7.54) | 3.14 (2.27-4.35) |
| Threatened/tortured | 1.79 (1.04-3.08) | 3.93 (2.35-6.59) | 3.95 (2.29-6.83) | 2.92 (1.91-4.46) |
| Simultaneous results | ||||
| Lone parent status | 1.68 (0.85-3.30) | 1.75 (1.32-2.31) | 1.44 (0.82-2.55) | 1.45 (0.92-2.28) |
| Socio-demographic | ||||
| Low SES area | 0.96 (0.72-1.29) | 1.17 (0.81-1.70) | 0.83 (0.38-1.81) | 1.28 (0.97-1.70) |
| Rental housing | 1.19 (0.77-1.84) | 1.12 (0.87-1.45) | 1.83 (0.90-3.76) | 1.06 (0.75-1.49) |
| Reliant on welfare | 0.99 (0.67-1.46) | 1.06 (0.71-1.58) | 1.73 (0.91-3.32) | 1.33 (0.95-1.86) |
| Not employed | 1.10 (0.73-1.64) | 1.36 (0.97-1.90) | 0.65 (0.34-1.26) | 1.40 (0.97-2.01) |
| Not completed high school | 1.59 (1.07-2.39) | 1.30 (0.84-2.01) | 1.14 (0.76-1.72) | 1.16 (0.87-1.54) |
| Number of children | 1.08 (0.94-1.22) | 1.12 (1.00-1.27) | 0.88 (0.68-1.14) | 1.14 (1.00-1.30) |
| Physical and sexual violence | ||||
| Sexual molestation | 1.55 (1.06-2.28) | 2.10 (1.32-3.35) | 2.07 (0.87-4.94) | 1.24 (0.73-2.11) |
| Rape | 1.54 (0.84-2.80) | 1.43 (0.85-2.38) | 1.22 (0.61-2.45) | 2.08 (1.40-3.08) |
| Physical attack | 1.86 (1.16-2.99) | 2.51 (1.75-3.60) | 2.16 (1.24-3.76) | 1.58 (1.01-2.47) |
| Threatened/tortured | 0.86 (0.46-1.60) | 1.76 (0.88-3.53) | 1.73 (0.93-3.21) | 1.57 (0.93-2.66) |
Initial simultaneous logistic regression analyses checked for the presence of interactions between lone parent status and each of the socio-demographic and violence variables for each mental health measure. Such an interaction could indicate a moderated relationship. Of the 40 interaction terms, only two were significant (both for anxiety disorders) and, in both cases, the main effect on the predictors (employment and experience of being threatened/tortured) was significant. Further, in both cases the interaction reflected the greater prevalence of anxiety disorders for partnered mothers who were unemployed (compared with those who were employed) and those who had been threatened or tortured, with lone mothers showing less difference. Given that these interactions were in the opposite direction to that anticipated, and that they occurred at a chance level (i.e. 2 in 40), further analyses did not include interaction terms.
In the simultaneous models, the physical and sexual violence measures remained significant predictors of psychiatric disorders, whereas few of the socio-demographic variables remained significant. Lone parent status was significantly associated only with anxiety disorders. However, experience of sexual molestation and physical assault were stronger predictors of anxiety disorders than lone parent status. Physical assault and sexual molestation were significantly associated with depression. Previous physical assault was the only significant unique predictor of substance use disorders. Although the odds ratio for sexual molestation was high, the association was nonsignificant owing to the wide confidence intervals. Finally, rape and physical assault were the predictors most strongly associated with general psychological distress.
The simultaneous regression results showed that much of the predictive power of lone parent status was accounted for by other variables within the models.
The explained fraction (Table 4) showed that between 50% and 81% of the difference between lone and partnered mothers in the prevalence of psychiatric disorders was mediated by the physical/sexual violence and socio-demographic measures. For substance use disorders, for example, the inclusion of sociodemographic and violence measures caused a reduction in the odds ratio from 3.35 to 1.44, accounting for 81% of the association with lone motherhood. Considered separately, both the violence measures and the socio-demographic measures mediate the relationship between lone parent status and mental health, although the violence measures are greater for three of the four measures. However, there is also considerable overlap between the two types of variables, as the sum of the two mediation effects is considerably less than the total explained fraction.
Table 4 Fraction of the difference between lone and partnered mothers in the prevalence of psychiatric disorders mediated by physical/sexual violence and socio-demographic measures
| Mediating variable | Affective disorder % | Anxiety disorder % | Substance use disorder % | Psychological distress % |
|---|---|---|---|---|
| Violence only | 30 | 52 | 49 | 46 |
| Socio-demographic only | 26 | 31 | 55 | 42 |
| Violence and demographic | 50 | 63 | 81 | 67 |
To assess further the relative importance of the different blocks of predictors, the χ2 statistics for the change in log-likelihood associated with the addition or deletion of the blocks of socio-demographic and violence variables were considered. The univariate results confirmed that both blocks of variables (socio-demographic characteristics and experience of physical and sexual violence) were significantly associated with each of the psychiatric measures (compared with constant-only models). The block of physical and sexual violence measures was, however, more strongly associated with all mental health measures, particularly anxiety disorders. This same conclusion is reached from analysis of the relative contribution of each block of variables to the full model, which compares models with and without each block of variables. The physical and sexual violence measures consistently made a significant additional contribution.
DISCUSSION
Background
Lone parent families, predominantly headed by women, have become a common family type across Western countries. In Australia, 22% of families with children aged under 15 years are lone parent families, with most of these (around 90%) headed by women (Australian Bureau of Statistics, 2002). British data are virtually identical (Reference Summerfield and BabbOffice for National Statistics, 2003). Therefore, evidence that lone mothers are more likely to have psychiatric disorders and poor mental health (Reference Brown and MoranBrown & Moran, 1997; Reference Lipman, Offord and BoyleLipman et al, 1997; Reference Hope, Power and RodgersHope et al, 1999; Reference Weitoft, Haglund and HjernWeitoft et al, 2000; Reference Whitehead, Burström and DiderichsenWhitehead et al, 2000) identifies a substantial societal issue with implications for a significant number of women and children.
Although economic hardship/poverty is an important explanatory factor (Reference Brown and MoranBrown & Moran, 1997; Reference Hope, Power and RodgersHope et al, 1999), the poorer mental health of lone mothers could also reflect lower levels of social support and personal protective resources (Reference Brown and MoranBrown & Moran, 1997; Reference Whitehead, Burström and DiderichsenWhitehead et al, 2000), unemployment (Reference Hope, Power and RodgersHope et al, 1999) or lack of full-time employment (Reference Macran, Clarke and JoshiMacran et al, 1996), role overload or time poverty (Reference Macran, Clarke and JoshiMacran et al, 1996; Reference Whitehead, Burström and DiderichsenWhitehead et al, 2000) or be a direct consequence of divorce or separation (Reference Lorenz, Simons and CongerLorenz et al, 1997). The association between marital status and psychiatric disorders could also reflect common underlying factors such as early social experiences (Reference Davies, Avison and McAlpineDavies et al, 1997) or childhood abuse (Reference Bifulco, Brown and AlderBifulco et al, 1991; Reference Lipman, McMillan and BoyleLipman et al, 2001). Understanding the mechanism behind their poorer mental health is vital for determining appropriate policy responses and identifying ways to target assistance effectively. Such understanding is also critical given the current focus in many English-speaking countries on reform of welfare/social support systems, including financial assistance to lone mothers.
Summarising and understanding the current findings
The results of the current study are consistent with the previous literature in showing that lone mothers have higher rates of psychiatric disorders than partnered mothers. An advantage of the current analysis is the availability of information on the prevalence of a range of different types of disorders, as well as measures of psychological distress. Much research has focused exclusively on depression. The breadth of the present investigation is important, because the greatest differences between lone and partnered mothers were found in the prevalence of substance use and anxiety disorders. Some previous studies considering substance use disorders (Reference Lipman, Offord and BoyleLipman et al, 1997; Reference Lipman, McMillan and BoyleLipman et al, 2001) found no significant associations with women's marital status (but see Reference Weitoft, Haglund and HjernWeitoft et al, 2000).
Lone mothers were also more likely than partnered mothers to have experienced the physical and sexual violence traumas examined in this study, with odds ratios of 3–4. This difference is not a simple response bias because the two groups reported similar levels of exposure to natural disasters. It is possible that factors such as negative reporting biases associated with current negative mood state reduce the reliability and validity of retrospective reporting of past traumatic events. However, memory for specific events is thought to be reasonably accurate regardless of current mood state (Reference Brewin, Andrews and GotlibBrewin et al, 1993) and when evidence for negative reporting biases is found it does not seem to influence memory for the types of measures considered in this study (physical and sexual violence; see Reference Schraedley, Turner and GotlibSchraedley et al, 2002).
The relationship between trauma and a range of psychiatric disorders (not only post-traumatic stress disorder) has been demonstrated in many studies (e.g. Reference McLeod and KesslerMcLeod & Kessler, 1990; Reference Bifulco, Brown and AlderBifulco et al, 1991; Reference Turner, Wheaton and LloydTurner et al, 1995; Reference Brown and MoranBrown & Moran, 1997). Although the trauma event is generally considered the causal factor, this need not be the case. Mental illness may increase vulnerability to, or likelihood of experiencing, some forms of trauma (e.g. Reference Maciejewski, Prigerson and MazureMaciejewski et al, 2000).
In the current study, the measures of physical and sexual violence were more strongly associated with psychiatric disorders and psychological distress than either partnered status or the socio-demographic characteristics. Much of the difference in mental health between lone and partnered mothers could be accounted for by different exposures to such trauma. The results also showed that different forms of violence were associated with different psychiatric disorders, suggesting different aetiological pathways. Physical assault was associated with all four mental health measures but was the only trauma associated with substance use disorders in the simultaneous analyses. Experience of sexual molestation was associated with depressive and anxiety disorders, whereas experience of rape was significantly associated only with the measure of psychological distress.
Interpreting these findings
There is debate over whether group differences (e.g. social status) in the prevalence of mental health problems are a function of differential vulnerability to stressors (Reference McLeod and KesslerMcLeod & Kessler, 1990) or differences in rates of exposure to trauma (Reference Turner, Wheaton and LloydTurner et al, 1995). Alternatively, the interrelationship between these variables may mean that, although stressors have a negative consequence only in the presence of personal vulnerability, such vulnerability is associated with increased risk of exposure to trauma (e.g. Reference Brown and MoranBrown & Moran, 1997; Reference Maciejewski, Prigerson and MazureMaciejewski et al, 2000). The results support the greater exposure hypothesis, showing that lone parents experience higher rates of physical and sexual violence. However, the current study did not examine the psychological or environmental characteristics related to differential vulnerability (e.g. coping skills, mastery, social support). It may be that some women experience a cycle of trauma and distress where the consequences of these are exaggerated by and contribute to their lack of coping skills and compromise psychological well-being, thereby increasing vulnerability to or experience of dependent life events, and so on (Reference Maciejewski, Prigerson and MazureMaciejewski et al, 2000).
At one level, this study has shown that the experience of a specific type of trauma (i.e. physical and sexual violence) is associated with psychiatric disorders. But this violence measure itself covers a range of different experiences. The Australian Bureau of Statistics women's safety survey found that around one-third of women reporting some form of physical or sexual violence in their lifetime had been the victim of childhood abuse (Australian Bureau of Statistics, 1996). Further, for around one-third of unpartnered women who had experienced violence in adulthood the perpetrator had been a former partner. It may be that the effectiveness of the current measure was due to the fact that it encapsulated diverse and distinct aspects of violence.
The results indicate that experience of physical and sexual violence is a better predictor of current mental health status than are the socio-demographic measures. Few of the individual measures related to social or financial circumstances were significantly associated with experience of psychiatric disorders in the final step of the sequential logistic regression. This was not simply a consequence of the correlation between the various socio-demographic variables. The measures of lifetime violence were more strongly associated with psychiatric disorders than were the socio-demographic variables in both univariate analyses and in analysis of the contribution of each block of variables.
The current results were somewhat unexpected given the body of evidence showing the relationship between financial hardship/poverty and poor mental health. The measures of rental housing and reliance on welfare were those most directly related to individual financial status, and these were the two strongest socio-demographic predictors in the univariate analyses. The current study used reliance on government pensions or payments as an indicator of financial hardship because welfare receipt is strongly associated with income. For Australian households in the lowest income quintile, government payments comprise over 92% of total household income. The corresponding figure for households in the second lowest income quintile is 50% and the rate rapidly decreases to only 1.4% of the income of households in the highest quintile (Australian Bureau of Statistics, 2000).
It is important to recognise that the socio-demographic variables were also important mediators of the relationship between lone parent status and psychiatric disorders (see the explained fraction results in Table 3). However, besides being stronger overall predictors of mental health, the measures of physical and sexual violence were stronger mediators for all but one mental health measure. Further, there was considerable overlap between the violence and socio-demographic mediators.
The current results may reflect that the trauma measures were a more sensitive marker of an underlying distribution of disadvantage. A number of researchers (e.g. Reference PearlinPearlin, 1989; Reference BrownBrown, 2002) have noted the importance of considering the structural context in which stressful life events occur. Rather than separate incidents, traumatic events are episodes that cannot be extricated from, and that reflect, the social circumstances in which they occur. These events can, therefore, be considered surrogate indicators of relatively enduring circumstances or systemic stressors (Reference Turner, Wheaton and LloydTurner et al, 1995). It may be that, for some women, early childhood adversity, poverty and hardship, domestic violence, other forms of physical and sexual violence, mental health problems, relationship difficulties, poor personal resources and coping abilities, limited labour market skills or attachment and poor educational achievement are all inter-correlated and indicative of their more entrenched disadvantage. None of these individual measures can be viewed as the primary causal factor. This could explain why cross-national comparisons consistently show lone mothers to have elevated levels of psychiatric disorders compared with partnered mothers, despite dramatic differences in economic and social conditions across countries (including differences in employment and rates of participation in paid employment, social policy responses, rates of poverty, societal norms and expectations; e.g. Reference Whitehead, Burström and DiderichsenWhitehead et al, 2000).
Future directions
Violence against women is an issue that requires research and policy attention (Reference Watts and ZimmermanWatts & Zimmerman, 2002). Lone mothers are a heterogeneous group, and it must be recognised that most (around 60%) do not have a psychiatric disorder and have not experienced physical or sexual violence. However, the relationship between physical and sexual violence and psychiatric disorders among lone mothers identifies an important direction for future research. Further analysis is needed to explore the co-occurrence and interrelationships between characteristics and experiences. Given that the current study is based on cross-sectional data, it is not possible to make claims of the causal direction of the relationship between trauma and psychiatric disorders. This would require longitudinal or prospective data, or the availability of information on the onset of trauma and disorders that is more robust than that available in the current data-set. There are clues in the current analysis about the nature of the relationship between violence and psychiatric disorders, suggesting that different forms of violence are associated with specific mental health problems and therefore require different types of response. Community-level interventions seem most appropriate given the entrenched nature of the disadvantage (Reference Davies, Avison and McAlpineDavies et al, 1997). It is also important to consider the role of factors such as social support, coping skills and self-efficacy. Although early intervention and prevention may be the most effective way to address this constellation of disadvantage, current strategies to minimise the occurrence of trauma should be complemented by interventions to build personal capacity and resources, because these offer the potential to improve the immediate circumstances of women and their children.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Clinicians and others involved in primary care should be aware that, compared with partnered mothers, lone mothers are significantly more likely to have psychiatric disorders and poor mental health outcomes, particularly anxiety and substance use disorders.
-
▪ Lone mothers are more likely to have experienced physical and sexual violence and these severe traumatic experiences are more strongly associated with the presence of psychiatric disorders than either lone parent status or other socio-demographic characteristics.
-
▪ Exposure to different types of violence is associated with different psychiatric conditions.
LIMITATIONS
-
▪ The data are cross-sectional, limiting conclusions about the direction of relationships.
-
▪ The data-set did not include items to enable an examination of the role of moderating factors such as coping skills or social support.
-
▪ Further research is needed to examine the broader context in which violence occurs, taking account of the co-occurrence of, and interrelationship between, different forms of disadvantage.
Acknowledgements
I thank Bryan Rodgers and Tony Jorm for comments on an earlier draft of. this manuscript, and Ruth Parslow and Keith Dear for statistical advice.







eLetters
No eLetters have been published for this article.