


Introduction
Arytenoid granuloma is a benign exophytic inflammatory lesion that arises from the vocal process of the arytenoid cartilage. Arytenoid granulomas are also termed vocal process granulomas.Reference Devaney, Rinaldo and Ferlito1,Reference Carroll, Gartner-Schmidt, Statham and Rosen2 On videolaryngostroboscopy, arytenoid granuloma appears as a fleshy pale or sometimes reddish pedunculated mass with an underlying erythematous ulcer base, or it may take the form of a nodular or exophytic mass lesion (often reddish or pale grey), as shown in Figure 1.

Fig. 1. Grade 3a right-sided arytenoid granuloma with a pale fleshy appearance.
Arytenoid granuloma is most commonly encountered in males.Reference Carroll, Gartner-Schmidt, Statham and Rosen2 Frequent throat clearing, globus sensation, chronic cough, difficulty in swallowing, pain in the throat and change in voice are the usual presenting symptoms.Reference Ylitalo and Lindestad3 Laryngopharyngeal reflux (LPR), vocal abuse, continuous voice use in excess of 4–6 hours a day, and prolonged endotracheal intubation are the predominant factors associated with the development of arytenoid granuloma.Reference Damrose and Damrose4
The Reflux Symptom Index and Reflux Finding Score are used to quantify the symptoms of LPR.Reference Kirti5 The Reflux Symptom Index is a clinical questionnaire administered to patients with LPR symptoms, such as excess throat mucus and repeated throat clearing. The Reflux Finding Score is an endoscopic scoring system for diagnosing mucosal changes caused by LPR, such as erythema or hyperaemia, and posterior commissure hypertrophy.
A wide variety of therapeutic methods, such as simple observation, voice therapy, voice rest, anti-reflux therapy, antibiotics, corticosteroids (injected, inhaled or parenteral) and local injection of Botulinum toxin, have been used for the treatment of arytenoid granuloma.Reference Lee, Hong, Choi, Sun, Park and Lee6,Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7 In persistent and refractory cases, invasive procedures such as endoscopic cold steel removal, laser excision and low-dose radiotherapy have also been used.Reference Lee, Hong, Choi, Sun, Park and Lee6 However, none of the treatment modalities has been uniformly successful. Likewise, there are also no randomised, controlled trials or large cohort studies to support the effectiveness of one modality over another.Reference Tsai, Ma, Shih, Tsou and Sung8
There is good evidence that aggressive and prolonged anti-reflux treatment, in conjunction with or without voice therapy, forms the main treatment strategy, and is associated with low recurrence rates.Reference Lee, Hong, Choi, Sun, Park and Lee6,Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7 The role of surgical management in the treatment of arytenoid granuloma is controversial, as the majority of studies have reported low response rates and a high risk of recurrence following surgery.Reference Ylitalo and Lindestad3,Reference Havas, Priestley and Lowinger9–Reference Chang, Xu and Cheng12
However, surgical removal as the first-line treatment has been advocated for large granulomas, based on an endoscopic grading system proposed by Farwell et al. (grades 1–4; unilateral cases and bilateral cases are classified as ‘a’ and ‘b’, respectively).Reference Farwell, Belafsky and Rees13 Surgery is also advocated for those granulomas causing airway obstruction (grade 3a or 4a), bilateral granulomas (grade 3b or 4b), and those with a short history, along with a history of tobacco or alcohol consumption, and clinical findings suggestive of malignancy needing histological confirmation. Surgery is also required for granulomas that fail to respond to conservative management.Reference Chen, Chen, Yang, Li, Wu and Chen11,Reference Chang, Xu and Cheng12
Surgical excision has been carried out with cold steel instruments, the carbon dioxide (CO2) laser and the potassium titanyl phosphate (KTP) laser.Reference Chen, Chen, Yang, Li, Wu and Chen11,Reference Hirano, Kojima, Tateya and Ito14,Reference Dominguez, Brown and Simpson15 The CO2 laser has been the preferred tool in recent times, as it offers precise cutting with a minimum of collateral thermal damage to the underlying tissue.Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7
This study aimed to assess the outcome of a combination of proton pump inhibitor (PPI) treatment, voice therapy and lifestyle modification. It also aimed to identify the indications for surgical management of arytenoid granuloma and the role of Botulinum toxin injection.
Materials and methods
This was a retrospective data analysis study conducted at a tertiary level care hospital in Pune, India. Institutional ethics committee approval was obtained.
The records of patients with clinically suggestive arytenoid granuloma, managed between July 2012 and June 2019, were retrieved and included in the study. The data retrieved included: age; sex; presenting complaints; history of symptoms suggestive of any systemic disease such as tuberculosis; history of intubation; history of smoking, alcohol intake or vocal abuse; Reflux Symptom Index; Reflux Finding Score; type and duration of treatment received; and histopathological examination reports of operated patients.
Videolaryngostroboscopy recordings and i-Scan® screening findings were reviewed (Figure 2a and 2b). The i-Scan tool is a dynamic software-based endoscopic image enhancement technology that provides an enhanced view of the texture of the mucosal surface and blood vessels, allowing recognition of pathological lesions like dysplasia and malignancy that are otherwise not visible with conventional white-light endoscopy. This optical diagnostic software is available as a Pentax® system, and similar narrow-band imaging software is available via Olympus Medical®.

Fig. 2. (a) i-Scan image of right-sided grade 1 arytenoid granuloma and left-sided grade 4 arytenoid granuloma, showing contrast enhancement and sharpened view of blood vessels supplying the lesion. (b) i-Scan image of left-sided grade 1 arytenoid granuloma, showing contrast enhancement and sharpened view of blood vessels supplying the lesion. R = right; L = left
Conservative management
The conservative treatment group included patients with LPR symptoms who were given anti-reflux medication (the PPI esomeprazole, 40 mg twice daily for three months). Those with a history of vocal abuse were given 8–10 sessions of voice therapy. In a few patients, both PPI treatment and voice therapy were given for the same duration. Intubation granulomas were treated conservatively with anti-inflammatories (i.e. oral and inhaled corticosteroids), anti-reflux medication, antibiotics and voice therapy.
During the course of treatment, patients were advised to attend for follow up every four to six weeks, for symptom assessment and endoscopic examination, until symptom resolution and normal endoscopy findings. Complete symptom resolution and arytenoid granuloma resolution after three months of conservative management was considered indicative of successful treatment.
Surgical management
Granulomas causing airway obstruction (grade 3a or 4a), bilateral granulomas (grade 3b or 4b), those with a short history, patients with a history of tobacco or alcohol consumption, and those who demonstrated clinical findings suggestive of malignancy needing histological confirmation were selected for surgical management with transoral CO2 laser surgical excision. Patients for whom conservative treatment had failed were also managed with surgical excision.
Transoral CO2 laser surgical excision was undertaken under general anaesthesia, with the patient in the supine position. The larynx was suspended using a Lindholm operating laryngoscope (Karl Storz, Tuttlingen, Germany) and was visualised through a Leica® microscope. Using microlaryngeal instruments, and an Acu-Blade® CO2 laser at 2–3 W power in a continuous mode, the lesion was grasped and excised, along with its base, from the surrounding normal mucosa. Care was taken to prevent ‘ghost strikes’ on the exposed arytenoid cartilage. Excised tissue was sent for histopathological examination. Patients were given a course of broad-spectrum antibiotics, and continued on PPIs and vocal hygiene post-operatively.
Patients were advised to attend follow-up appointments every four to six weeks following surgery. Symptom assessment and endoscopic examination were performed during each visit. Complete symptom resolution and arytenoid granuloma resolution on endoscopy after three months of surgery was considered indicative of successful treatment. The cases that recurred after surgical excision were managed with revision surgery along with 10 units of Botox® injection into the ipsilateral thyroarytenoid muscle.
Results
The records of 62 patients diagnosed with arytenoid granuloma were retrieved and analysed. Fifty-three patients (85.5 per cent) were males; the male to female ratio was 5.9:1. The most common age at presentation was the fifth decade, for both males and females; the age distribution of the patients is shown in Table 1. A change in voice (45.2 per cent) and pain in the neck (41.9 per cent) were the predominant symptoms in our patients; the distribution of symptoms among the patients is shown in Table 2.
Table 1. Age distribution of patients

Table 2. Predominant symptoms of patients

Symptoms suggestive of LPR were found in 38 patients (61.2 per cent). Vocal abuse and vocal misuse history were found in 16 patients (25.8 per cent). Other risk factors, such as a history of smoking, were found in 10 patients (16.1 per cent). Two patients (3.2 per cent) had a history of intubation. In eight patients (12.8 per cent), no risk factors could be elicited, as shown in Table 3.
Table 3. Risk factors for arytenoid granuloma

Videolaryngostroboscopy images of different grades of arytenoid granuloma are presented in Figure 3. Bilateral grade 4b intubation granuloma is shown in Figure 4.
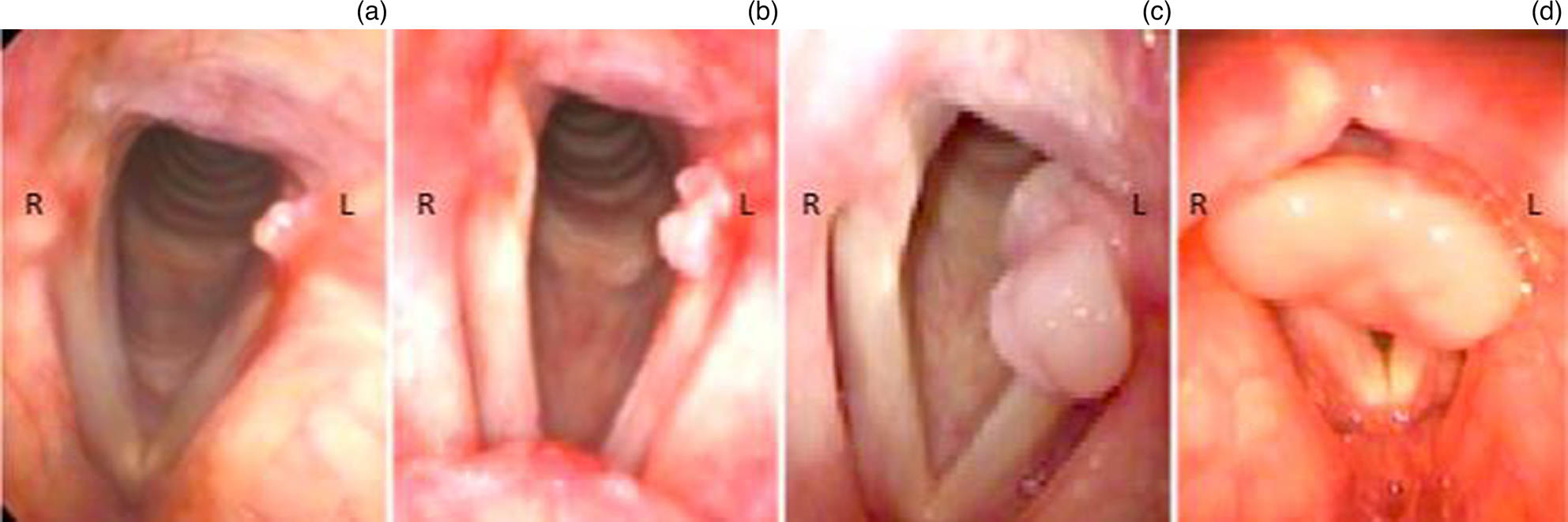
Fig. 3. Endoscopic images showing various grades of arytenoid granuloma: (a) grade 1a, (b) grade 2a, (c) grade 3a and (d) grade 4a. R = right; L = left

Fig. 4. Bilateral grade 4b intubation granulomas. R = right; L = left
Conservative management findings
Out of 48 patients, 32 (66.6 per cent) responded to conservative management, with complete and permanent resolution of symptoms and endoscopy findings. Twenty out of 32 patients (62.5 per cent) responded to PPI alone, 9 out of 12 (75 per cent) responded to a combination of PPI and voice therapy, and 3 out of 4 (75 per cent) responded to voice therapy alone, as shown in Table 4.
Table 4. Patients who received conservative management

PPI = proton pump inhibitor
Sixteen patients in whom medical management failed (33.3 per cent) were recommended for surgery. Four of the 16 patients opted for continuation of conservative management. They were recommended PPI and voice therapy for another three months. Two of these patients did not recover and were scheduled for surgery.
Surgical management findings
Twenty-eight patients underwent surgery. In 14 patients, it was the primary treatment modality; in the remaining 14 patients, conservative management had failed (Table 5). Of the 28 patients, 23 (82.1 per cent) had complete resolution of granuloma following surgery.
Table 5. Patients who received surgical management

In 10 out of 28 operated patients, specimens were sent for rapid microscopic analysis because of doubtful features on clinical examination. The histopathology report revealed tuberculosis in three cases, which was treated with anti-tubercular therapy, and squamous cell carcinoma in two cases, for which the patients underwent radiotherapy. Surgical excision was completed in two cases of pyogenic granuloma, and in one case each of pleomorphic adenoma, moderate dysplasia, and moderate to severe dysplasia. Histopathology reports of the remaining 18 patients who underwent complete excision revealed 16 cases of inflammatory granuloma, and 1 case each of amyloidosis and mild dysplasia.
Pain in the throat and dry cough were the most common complaints in the post-operative period. None of the patients developed any major complications, such as posterior glottic stenosis, following surgery.
Eleven of 16 patients with inflammatory granuloma (68.8 per cent) had complete resolution of arytenoid granuloma following a single surgical procedure. Recurrence was seen in five patients (31.3 per cent), with inflammatory granuloma occurring within 6–12 weeks following surgery. All patients with recurrence underwent revision surgery after a trial of PPI and voice therapy. These patients were also injected with 10 units of Botox into the ipsilateral thyroarytenoid muscle. None of these five patients had recurrence on follow up after three months.
Analysing the outcome of conservative treatment, we found only two cases initially misidentified as arytenoid granulomas, and neither showed sinister disease (one amyloidosis and the other mild dysplasia). They were diagnosed after a failure of three months of conservative treatment.
Histopathology
The most common pathology identified was inflammatory granuloma, with hyperplastic epithelium and chronic inflammation in 16 out of 28 patients (57.1 per cent) (Table 6). Other pathologies included: tuberculosis (three cases); pyogenic granuloma (two cases); pleomorphic adenoma (one case); amyloidosis (one case); mild, moderate and severe dysplasia (one case of each); and squamous cell carcinoma (two cases).
Table 6. Histopathological diagnoses

Discussion
Arytenoid granuloma is most commonly seen in males, with a predominance in the fourth and fifth decades of life.Reference Lemos, Sennes, Imamura and Tsuji16,Reference Wang, Ko, Wang, Hu and Hsiao17 A similar male predominance (85 per cent) was also observed in our study. Our study population compares favourably with most published work. A systematic review of arytenoid granuloma management identified 14 papers suitable for analysis.Reference Tsai, Ma, Shih, Tsou and Sung8 Of these, only two presented larger numbers of patients than our study.
The causes of arytenoid granuloma are not well known, and there is no standard management protocol.Reference Lemos, Sennes, Imamura and Tsuji16 History and findings suggestive of LPR (61 per cent) and vocal abuse (26 per cent) were the predominant risk factors identified in our patients with arytenoid granuloma, which is similar to other studies.Reference Lemos, Sennes, Imamura and Tsuji16,Reference Hoffman, Overholt, Karnell and McCulloch18,Reference de Lima Pontes, De Biase and Gadelha19
A systematic review by Karkos et al. concluded that aggressive and prolonged anti-reflux medication, with or without voice therapy, forms the main treatment strategy, and is associated with fewer recurrences.Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7 Recent studies also emphasise these findings, and highlight the importance of continuing lifestyle modifications to prevent future recurrence.Reference Kobayashi, Tsunoda, Ueha, Fujimaki, Nito and Yamasoba10,Reference Chen, Chen, Yang, Li, Wu and Chen11
We achieved resolution rates of 62.5 per cent with anti-reflux treatment and 75 per cent with voice therapy alone, which are similar to other studies.Reference de Lima Pontes, De Biase and Gadelha19 A resolution rate of 75 per cent with combination treatment was achieved in our study, which is similar to that reported in a study by Chen et al., of 72.1 per cent.Reference Chen, Chen, Yang, Li, Wu and Chen11 The better resolution of granulomas following combination treatment instead of a single treatment in our study may be because of a better selection of patients, and possibly because of the prolonged treatment duration (i.e. three months). Combination treatment including voice therapy will change vocal behaviour and provide better circumstances for the healing process.Reference Ylitalo and Lindestad3
A multicentre study by Lee et al. also claimed that PPI and Botox were effective treatments only in the short term, whereas voice therapy provided significant long-term improvement.Reference Lee, Hong, Choi, Sun, Park and Lee6
Surprisingly, not many studies have described the duration of conservative treatment with PPI required for the complete resolution of granulomas. Despite conservative management with PPI for three months, 29 per cent of patients in our study had no resolution, which was similar to that reported in other studies.Reference Lemos, Sennes, Imamura and Tsuji16 This proves the need for prolonged control of underlying reflux, combined with voice therapy and continuing lifestyle modifications, for the treatment of arytenoid granuloma.Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7,Reference Havas, Priestley and Lowinger9–Reference Chen, Chen, Yang, Li, Wu and Chen11
The role of surgical management for arytenoid granuloma is unclear and remains controversial, with the majority of studies reporting a high recurrence rate following surgery.Reference Lee, Hong, Choi, Sun, Park and Lee6,Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7,Reference Chen, Chen, Yang, Li, Wu and Chen11,Reference Chang, Xu and Cheng12 A recent systematic review by Tsai et al. reported that 98 per cent of patients treated conservatively and 84 per cent of patients treated with surgery alone improved or resolved.Reference Tsai, Ma, Shih, Tsou and Sung8 Surgical treatment is based on the removal of the mass burden, while conservative management is based on reducing inflammation and the alteration of vocal behaviour. Both approaches help in reducing granulomas.Reference Lee, Hong, Choi, Sun, Park and Lee6 Surgical treatment shows a favourable outcome in the form of immediate improvement of voice parameters such as Voice Handicap Index-10 and maximum phonation time, but there is an increased likelihood of recurrence with surgical treatment alone.Reference Tsai, Ma, Shih, Tsou and Sung8 However, larger granulomas affecting voice and causing airway symptoms need to be removed surgically, but this should be followed by a conservative regimen to reduce the risk of recurrence.Reference Tsai, Ma, Shih, Tsou and Sung8 Finally, surgical management is also reserved for patients whose condition has not resolved with medical management, or in cases with risk factors for malignant changes, such as smoking and alcohol consumption.Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7,Reference Hoffman, Overholt, Karnell and McCulloch18
Cold steel excision has been replaced by the use of the laser because of the latter's precise cutting, reduced tissue damage and lower recurrence rate. Different types of lasers, like the KTP laser, the pulsed dye laser and the CO2 laser, have been used in out-patient settings and in the operating theatre. The CO2 laser has become the most popular choice because of its precise cutting and reduced injury to surrounding tissue.Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7 In comparison to CO2 laser surgery, Hirano et al.Reference Hirano, Kojima, Tateya and Ito14 and Dominguez et al.Reference Dominguez, Brown and Simpson15 removed arytenoid granulomas using an in-office-based, pulsed KTP laser, and concluded that this is an effective treatment option for arytenoid granuloma. There are no comparative studies that describe the advantages of the CO2 laser over the KTP laser, or vice versa.
In our study, 82.1 per cent of patients who underwent surgical excision had complete resolution, which is comparable to a study by Lemos et al. (90 per cent).Reference Lemos, Sennes, Imamura and Tsuji16 Chen et al. reported a smaller response rate of 38.9 per cent following CO2 laser surgery, and this could be because of a lack of adequate conservative treatment before surgery in their patients.Reference Chen, Chen, Yang, Li, Wu and Chen11
In our study, the recurrence rate following surgery was 17.9 per cent, which is lower when compared with the majority of studies. For example, Havas et al.Reference Havas, Priestley and Lowinger9 reported a 50 per cent recurrence rate, Ylitalo and LindestadReference Ylitalo and Lindestad3 reported a 92 per cent rate, and Kobayashi et al.Reference Kobayashi, Tsunoda, Ueha, Fujimaki, Nito and Yamasoba10 reported a 75 per cent rate. The low recurrence rate in our study could be because of the use of the CO2 laser, which has high precision and offers a bloodless operative field. The use of PPI pre-operatively as well as post-operatively is another factor supported by other studies.Reference Karkos, George, Van Der Veen, Atkinson, Dwivedi and Kim7
We combined laser surgery with Botox injection in five patients, and achieved complete resolution in all of them. Many studies have highlighted the use of Botox as an adjuvant treatment, as it causes temporary paralysis of the ipsilateral thyroarytenoid muscle, which gives sufficient time for healing.Reference Hoffman, Overholt, Karnell and McCulloch18 Percutaneous Botulinum toxin has been used as a safe and effective treatment for arytenoid granuloma in patients for whom conventional treatment has failed.Reference Damrose and Damrose4,Reference Lee, Hong, Choi, Sun, Park and Lee6 There is no consensus regarding the dose and use of Botox injection either during conservative management or during primary or revision surgery.
The use of image enhancement technology, such as narrow-band imaging or i-Scan, in addition to white-light endoscopy, increases the sensitivity for detection of early neoplastic and preneoplastic glottic lesions.Reference Ahmadzada, Tseros, Sritharan, Singh, Smith and Palme20 We used i-Scan (Pentax Medical), and were able to detect a few cases of arytenoid granuloma with abnormal morphological features of dysplasia, as shown in Figure 5b. We advised surgical intervention in these cases. We encountered other pathologies with an appearance of arytenoid granuloma, including pleomorphic adenoma, tuberculosis, dysplasia and amyloidosis, as shown in Figure 5. It has been documented that failure to establish a proper histopathological diagnosis can misdirect definitive treatment.Reference Wenig and Heffner21

Fig. 5. Various pathologies mimicking arytenoid granuloma: (a) tuberculomas of the vocal process of the arytenoid bilaterally, (b) i-Scan image showing dysplasia of the vocal process of the left arytenoid, (c) pleomorphic adenoma of the left arytenoid, and (d) sarcomatoid carcinoma of the right arytenoid. R = right; L = left
The cause of arytenoid granuloma is multifactorial and is the result of a complex inflammatory process. Trauma to the laryngeal mucosa is the initial insult, leading to ulceration of the vocal process. This causes chronic inflammation, resulting in the formation of granulation tissue. Surgical removal does not eliminate the underlying cause. Therefore, these patients need to be managed further, depending on their underlying risk factors.Reference Tsai, Ma, Shih, Tsou and Sung8 As reported by Tsai et al., the recurrence rate following conservative management is lower compared with surgical management, but this difference did not reach statistical significance.Reference Tsai, Ma, Shih, Tsou and Sung8 We believe that surgery has a definite role to play in managing these patients, provided there is a proper combination of conservative management in the pre- and post-operative periods.
• Combination treatment with anti-reflux medication and voice therapy is effective first-line management for arytenoid granuloma
• Pre- and post-surgery adjuvant treatment with proton pump inhibitor and voice therapy improves transoral laser surgery results in selected cases
• Local injection of Botox used with revision surgery was successful in treatment of failed surgical cases
• Careful clinical history and examination should be employed to exclude other pathologies
It has been recently concluded that granulomas with minimal symptoms can be managed conservatively with a low chance of recurrence and a good response, whereas large and symptomatic granulomas require surgical excision followed by conservative management to reduce the chance of recurrence.Reference Tsai, Ma, Shih, Tsou and Sung8 Neither this nor the effects of smoking and alcohol consumption have been evaluated in this study. Finally, there is a need for future studies to define the timeline of conservative treatment for complete remission and to determine proper treatment guidelines for managing this rare entity.
Conclusion
Combination treatment with anti-reflux medication and voice therapy is effective first-line management for patients with arytenoid granuloma. Pre- and post-surgery adjuvant treatment with PPI and voice therapy improves the results of transoral laser surgery in selected cases. Local injection of Botox used with revision surgery was successful in the treatment of failed surgical cases. Careful clinical history and examination should be employed to exclude other pathologies.
Acknowledgements
We would like to deeply acknowledge Dr Liam M Flood, for his valuable inputs in preparing and drafting the manuscript. We would like to extend our heartfelt thanks to all our colleagues from the ENT department who provided insights and expertise that assisted the research.
Competing interests
None declared











