


Whether high intelligence represents positive (adaptive, desired) outcomes or may come with disadvantages has been a topic of debate. Reference Gale, Batty, Mcintosh, Porteous, Deary and Rasmussen1–Reference Vreeker, Boks, Abramovic, Verkooijen, van Bergen and Hillegers6 On one hand high IQ scores have been associated with excellent behavioural, cognitive and emotional control, coupled with good academic performance, along with better outcomes as regards education, occupation, mental and physical health and mortality (see review by Plomin & Deary). Reference Plomin and Deary5 On the other hand, several studies have shown that high intelligence scores and/or superior performance in (high) school predispose towards developing bipolar disorder, psychosis and/or schizophrenia. Reference Gale, Batty, Mcintosh, Porteous, Deary and Rasmussen1,Reference Karlsson2,Reference MacCabe, Lambe, Cnattingius, Sham, David and Reichenberg4,Reference Vreeker, Boks, Abramovic, Verkooijen, van Bergen and Hillegers6,Reference Tiihonen, Haukka, Henriksson, cannon, Kieseppa and Laaksonen7 It is also clear that a high IQ score by itself is not sufficient to result in high educational and occupational achievement, Reference Sternberg, Grigorenko and Bundy8 suggesting that other factors may undermine the strong positive effect of high intelligence on achievement. From an evolutionary perspective, scoring in the average range of the intelligence continuum may represent a favourable trade-off between advantages and disadvantages of extreme polygenic liabilities, as has been shown for personality traits. Reference Nettle9 Whether such a U-curve exists for IQ scores in relation to problems of attention-deficit hyperactivity disorder (ADHD) (i.e. both low and high intelligence scores are related to increased levels of ADHD problems) has been vigorously debated but not systematically studied. Some argue that high intelligence (like low intelligence) is inherently related to characteristics indicative of ADHD, such as high activity levels, low impulse control, frustration and boredom, and poor attention span. Reference Budding and Chidekel10–Reference Webb, Amend, Webb, Goerss, Beljan and Olenchak12 However, it has also been stated that these problems diverge from those seen in individuals with ADHD of below-average intelligence, by being specific to situations that evoke boredom and frustration rather than pervasive. This may occur in situations of poor matching of school tasks to the student's ability level. This raises the question of whether ADHD problems in highly intelligent students are less predictive of functional impairment (since they depend on the student's specific circumstances) than ADHD problems in students with average IQ scores. Reference Webb, Amend, Webb, Goerss, Beljan and Olenchak12 Conversely, the hypothesis that ADHD is underdiagnosed in highly intelligent individuals derives from the idea that high intellect may mask ADHD problems and associated cognitive deficits, Reference Milioni, Chaim, Cavallet, de Oliveira, Annes and dos Santos13,Reference Moon, Niehart, Reis, Robinson and Moon14 although these nonetheless exert their negative effects on functioning by causing performance at a level below the cognitive abilities of these individuals. Currently, this debate is fuelled by studies that suffer from severe selection biases by including only participants enrolled in special education programmes for highly intelligent students, using various cut-off scores for high intelligence (ranging mostly from 0.1% to 7.5% of the population, with some studies stretching this to even 16%), having a small sample size and/or using invalid measures for assessing ADHD (see for instance Alloway & Elsworth and Richards et al, reviewed by Rommelse et al). Reference Alloway and Elsworth15,Reference Rommelse, van der Kruijs, Damhuis, Hoek, Smeets and Antshel17 Our aim therefore was to address the following questions in a large, unbiased population-based study of children and adolescents aged 10–12 years. First, are high IQ scores – as are low scores – related to increased levels of ADHD and other problems compared with average intelligence? Second, are ADHD symptoms and externalising and internalising problems less pervasive across situations in children with high intelligence scores compared with children with average scores? Third, do ADHD problems in highly intelligent individuals predict functional school impairment to the same degree as in individuals with average IQ scores?
Method
This study is part of the Tracking Adolescents' Individual Lives Survey (TRAILS), a Dutch general population cohort study following 2230 children from early adolescence into young adulthood. Participants were recruited from the general population in five municipalities in the northern part of The Netherlands, including both urban and rural areas. All children living in these municipalities and born between October 1989 and September 1990 (two sites) and October 1990 and September 1991 (three sites) were selected (n = 3483). Their date of birth and contact information were obtained through the municipality administrations. The first exclusion criterion was non-participation by the school (9.6% of schools, 338 children). If the school of a selected child was willing to participate, parents were approached with information brochures (one for themselves and one for their children) and a follow-up telephone call in which they were invited to participate. Children were excluded from the study if they were incapable of participating because of intellectual disability or a serious physical illness or handicap; or if no Dutch-speaking parent or parent surrogate was available and it was not feasible to administer part of the measurements in the parent's language (n = 210). Of the 3483 selected children 2935 were eligible for the study, of whom 2230 participated (age range 10–12 years). For the current study 2221 (99.6%) children were included for whom intelligence data were available, of whom 39 (1.8%) were treated with methylphenidate. Further details of TRAILS have been described elsewhere. Reference De Winter, Oldehinkel, Veenstra, Brunnekreef, Verhulst and Ormel18,Reference Huisman, oldehinkel, de Winter, Minderaa, de Bildt and Huizink19 Written informed consent was obtained from all participants and their parents. The study was approved by the Dutch Central Medical Ethics Committee and all participants were compensated for their involvement in this study.
Measures
Full-scale IQ score was estimated by combining scores on the two subtests of the Revised Wechsler Intelligence Scales (WISC-R) that show the highest correlation (r = 0.90) with full-scale IQ: Vocabulary and Block Design. Reference Van Haasen, De Bruyn, Pijl, Poortinga, Lutje Spelberg and vander steene20,Reference wechsler21 For the assessment of ADHD and comorbid problems we used the Dutch translations of the parent-reported Child Behavior Checklist for school-age children (CBCL/6–18), the Youth Self-Report and a short version of the Teacher Report Form. Reference De Winter, Oldehinkel, Veenstra, Brunnekreef, Verhulst and Ormel18,Reference Sattler22,Reference Achenbach and Rescorla23 All questionnaires have been found valid and reliable. Reference De Winter, Oldehinkel, Veenstra, Brunnekreef, Verhulst and Ormel18 For the analyses in this review the two DSM-IV sub-dimensions for ADHD were used (attention problems and hyperactivity-impulsivity) as well as the two broad-band scores ‘internalising’ (based on three narrow-band scores: anxious/depressed, somatic complaints, withdrawn/depressed) and ‘externalising’ (based on two narrow-band scores: aggressive behaviour and delinquent behaviour). For all scales the raw mean scores (range 0–2) were used for further analyses. In addition, three measures indicative of functional impairment at school were assessed: school progress (parental report: −1 repeated grade or special education for learning disability, 0 regular, +1 skipped a grade), additional telephone calls because of problems at school (parental report: 0 no, 1 yes) and performance below own capacity (teacher report: 0 no, 1 yes). Socioeconomic status (SES) was based on ratings of occupation and education of both mother and father, as well as income; Z-scores of all five components were calculated and categorised as low (lowest 25%), medium (mid 50%) and high (upper 25%) SES. Ethnicity was parent-reported and dichotomised as Dutch or non-Dutch.
Statistical analysis
Analyses were carried out in SPSS Statistics version 23. The proportion of missing data was below 8% for all variables except teacher ratings (13.5%) and data were not replaced. Main analyses used IQ score as a continuous variable. Post hoc analyses and visualisation of results were performed with IQ-based groups: 55–70 (n = 65), 70–85 (n = 318), 85–100 (n = 805), 100–115 (n = 721), 115–130 (n = 268), 130–145 (n = 39). Five children with an IQ score of 45–55 were excluded from the post hoc tests since they formed too small a group. First, to test whether intelligence was related to increased levels of ADHD and other problems, curves were fitted on the data including linear (Y = b0+(b1*IQ)), inverse (Y = b0+(b1/IQ)), quadratic (Y = b0+(b1*IQ)+ (b2*IQ**2)) and cubic (Y = b0+(b1*IQ)+(b2*IQ**2)+(b3*IQ**3)) terms of IQ as predictor and the questionnaire scores as outcomes (Y). The best-fitting model was selected based on the largest F and R 2 values. Analyses were performed separately for different raters. In the second stage analyses were repeated using the difference score per symptom domain between teacher and parent as dependent measures to examine if rater discrepancy – reflective of situational (non-)pervasiveness of problems – was related to IQ score. In addition, to examine if rater agreement was influenced by IQ, both parent and parent × IQ scores were regressed onto teacher scores. In a final step, it was examined whether ADHD (and other) problems had a differential effect on functional impairment at school depending on IQ score. For this purpose, logistic regression analyses were performed on the three school impairment measures with the main effects (IQ score and symptom domains) and interaction effect (IQ score × symptom domains) included as predictors. Sensitivity analyses were conducted performing analyses separately for girls and boys, and excluding the most extreme IQ scores (plus or minus 2 standard deviations; IQ < 70 and IQ > 130) to test whether results were strongly influenced by the extreme ends of the IQ curve. All analyses were corrected for multiple testing (false discovery rate, α = 0.05). Reference Benjamini and Hochberg24
Results
Demographic and clinical descriptors of the sample are given in Table 1. Estimated IQ score was normally distributed (skewness −0.02, kurtosis 0.03) with a mean of 97.2 (s.d. = 15.0, range 45–149). Scores differed as a function of gender (t = 2.93, P < 0.001), with boys having an overall higher estimated IQ than girls (mean 98.1 v. 96.3). Boys were significantly overrepresented in the highest IQ group (IQ 130+, P = 0.025). Scores were significantly yet weakly associated with age: r = −0.08, P < 0.001. Post hoc tests indicated that the two lowest IQ groups (scores 55–69 and 70–84) were slightly older (1.2 months) than the other IQ groups (P values <0.001 to 0.05). The IQ score was related to SES: F (2,2178) = 159.99, P < 0.001. Low SES was overrepresented in the two lowest IQ groups (P < 0.001), whereas high SES was over-represented in the two highest IQ groups (scores 115–129 and 130+; P < 0.001) and middle SES overrepresented in the two average IQ groups (scores 85–99 and 100–114; P < 0.001). Scores were also related to ethnicity (F (1,2219) = 54.57, P < 0.001): non-Dutch ethnicity was relatively overrepresented in the three lowest IQ groups (scores 55–69, 70–84 and 85–99; P < 0.001) and underrepresented in the three higher IQ groups (scores 100–114, 115–129 and 130+; P <0.001). Scores were significantly related to functional impairment at school (school progress: F (2,2218) = 194.84, P < 0.001; parents receiving telephone call because of problems: F (1,2114) = 33.82, P < 0.001; performing below own capacity: F (1,1909) = 20.95, P < 0.001). On all three indices the two lowest IQ groups (scores 55–69 and 70–84) were more impaired compared with the full sample mean (all P values <0.001) and the two highest groups (scores 115–129 and 130+) were least impaired (all P values <0.001).
Table 1 IQ scores in relation to gender, age, socioeconomic status, ethnicity and functional impairment at school
| IQ score | ||||||||
|---|---|---|---|---|---|---|---|---|
| Full sample a | 55–69 | 70–84 | 85–99 | 100–114 | 115–129 | 130+ | Test statistics b | |
| n | 2230 | 65 | 318 | 805 | 721 | 268 | 39 | |
| Gender, % female | 50.8 | 58.5 | 54.1 | 52.4 | 50.2 | 45.1 | 30.8 | t = 2.93, P < 0.001 |
| Age, years: mean (s.d.) | 11.1 (0.56) | 11.3 (0.59) | 11.2 (0.56) | 11.1 (0.54) | 11.1 (0.56) | 11.1 (0.56) | 11.1 (0.51) | r = −0.08, P < 0.001 |
| Ethnicity, % Dutch | 86.5 | 72.3 | 78.3 | 84.5 | 91.4 | 92.9 | 89.7 | F(1,2219) = 54.57, P < 0.001 |
| SES, % | F(2,2178) = 159.99, P < 0.001 | |||||||
| Low | 25.3 | 57.8 | 48.1 | 26.9 | 17.2 | 7.9 | 10.3 | |
| Middle | 49.5 | 28.1 | 42.0 | 55.5 | 51.1 | 43.6 | 41.0 | |
| High | 25.2 | 14.1 | 9.9 | 17.5 | 31.6 | 48.5 | 48.7 | |
| School progress, % | F(2,2218) = 194.84, P < 0.001 | |||||||
| Regular | 75.4 | 24.6 | 54.7 | 72.9 | 86.5 | 89.9 | 89.7 | |
| Repeated grade or special education for intellectual disability |
22.5 | 75.4 | 44.7 | 25.6 | 11.8 | 4.1 | 2.6 | |
| Skipped a grade | 2.2 | 0 | 0.6 | 1.5 | 1.7 | 6.0 | 7.7 | |
| Parents received telephone call because of problems at school, % |
17.0 | 27.0 | 24.4 | 17.3 | 15.1 | 10.5 | 5.4 | F(1,2114) = 33.82, P < 0.001 |
| Performs below capacity according to teacher, % |
20.2 | 33.3 | 23.8 | 21.3 | 18.6 | 13.7 | 12.5 | F(1,909) = 20.95, P < 0.001 |
SES, socioeconomic status.
a. Full sample includes 5 children with IQ scores of 45–51 who formed too small a group for illustrating group means and s.d.s for psychopathology measures.
b. Analyses performed with estimated IQ score (Vocabulary and Block Design) as continuously distributed predictor.
Relation of IQ to symptoms
Results of analyses of IQ scores in relation to ADHD, externalising and internalising symptom levels are shown in Fig. 1 and online Table DS1. Effects were similar for boys and girls and similar when data for children with IQ scores below 70 or above 130 were excluded from the analyses. Curve estimations showed that of all symptom domains IQ score related most strongly and linearly to attention problems and hyperactivity-impulsivity problems according to parents and teachers, indicating that higher IQ score was related to lower levels of attention problems (4.1% and 8.5% explained variance in parent and teacher ratings, respectively) and hyperactivity-impulsivity problems (3.8% and 2.9% explained variance in parent and teacher ratings respectively). A similar linear (but weaker) association was found between IQ score and externalising problems according to both raters (explaining 3.1% and 2.4% of the variance in parent and teacher ratings respectively) and only teacher ratings of internalising problems related to estimated intelligence (2.0% explained variance) with lower levels of problems in the higher IQ range. No relationship between intelligence and self-reported symptom levels was found.
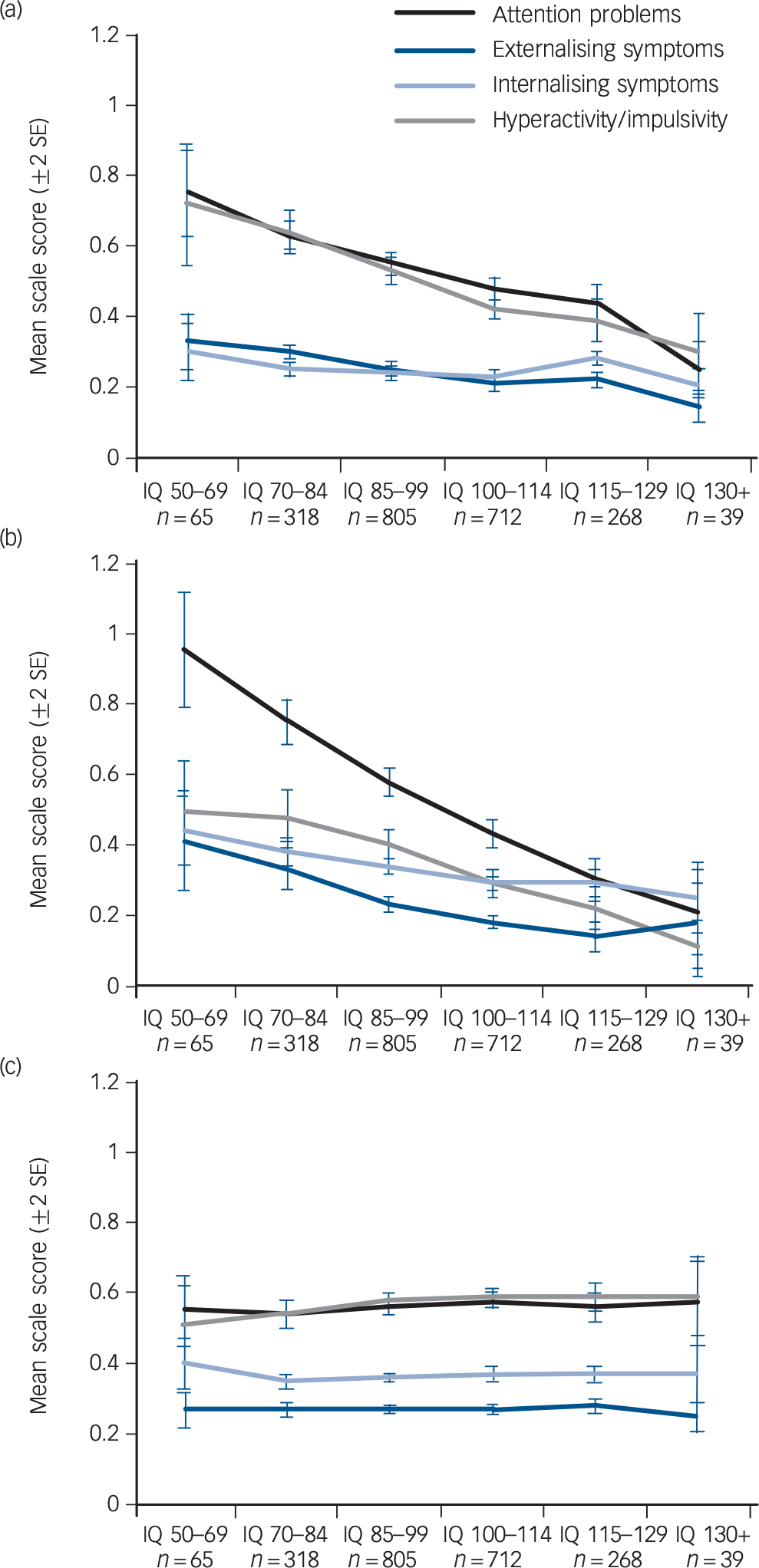
Fig. 1 Problems rated by (a) parents, (b) teachers and (c) self in relation to estimated IQ score. Problem scores are means plus or minus 2 standard deviations.
Rater discrepancies
Results of analyses of IQ scores in relation to rater discrepancy of ADHD, externalising and internalising symptom levels are shown in Fig. 2 and online Table DS2. Effects were similar when children with scores below 70 or above 130 were excluded from the analyses. Scores had the strongest effect on the rater discrepancy for attention problems (explaining 2.2% of the discrepancy), with less rater discrepancy in the middle IQ range than at the lower and higher ends. The effect remained when controlling for the mean level of attention problems, indicating this was not an artefact of the mean level of scores. Parents reported more attention problems than did teachers in children with high estimated IQ scores, whereas the reverse was found for children with low estimated scores. No such effect was found for rater discrepancy for hyperactivity-impulsivity problems: regardless of IQ score parents reported higher levels of these problems than did teachers and this difference was similar across the IQ range. The scores had no effect on rater discrepancy for externalising problems in girls but did in boys, with less rater discrepancy in the average to higher IQ spectrum than in the lower IQ spectrum (teachers rating more externalising problems than parents). There was a small effect of IQ on rater discrepancy for internalising problems, with less discrepancy in parent-teacher ratings in children with higher IQ scores, explaining 0.5–1.15% of the variance.

Fig. 2 Relation of IQ scores to rater discrepancy of attention-deficit hyperactivity disorder (ADHD), externalising and internalising symptom scores. Differences are means plus or minus 2 standard deviations.
Parent-teacher correlations were not similar across the IQ range for all problem domains, and were most strongly discrepant for attention problems (online Table DS2). Agreement for attention problems was highest in the middle IQ range as opposed to the low and high ends. Parent-teacher correlations for hyperactivity-impulsivity were also not constant across the IQ range, but no clear pattern of agreement along the IQ continuum emerged. Parent-teacher correlations for externalising problems were highest at the low end of the IQ range, whereas parent-teacher correlations for internalising problems were highest in the mid to high end of the IQ range.
Functional impairment
Potential differential effects of ADHD and other problems on functional impairment at school depending on IQ score are shown in Fig. 3 and online Table DS3. As described in Table 1, IQ score significantly related to all three functional impairment measures regarding school performance. In the logistic regression analyses with parent, teacher and self-reported problems (separate analyses), attention problems were the most common predictor of functional impairment at school according to parents and teachers. Attention problems negatively predicted school progress (according to parents and teachers), extra telephone calls because of problems at school (according to parents and teachers) and performance below own capacity (parents, teachers and self-report). Effects were stronger for girls than for boys according to teacher reports. Performing below own capacity and receiving extra telephone calls as a result of attention problems was moderated by IQ score according to teachers. Post hoc analyses indicated that teacher-rated attention problems predicted performing below own capacity most strongly in the average to higher IQ groups (score 70–84 t = 6.69, P < 0.001; score 85–99 t = 11.01, P < 0.001; score 100–114 t = 12.50, P < 0.001; score 115–129 t = 8.14, P < 0.001; score 130+ contained too few participants with teacher-rated suspected performance below own capacity for post hoc analyses) but less so in the below-average IQ group (score 55–69, t = 2.54, P = 0.02) (Fig. 3). Similar findings were found for extra telephone calls. Problems of hyperactivity-impulsivity did not robustly predict functional impairment at school across raters and impairment indices. One effect was found, with higher levels of parent-rated problems independent of IQ predicting worse school progress. Externalising problems were an important reason for functional impairment at school according to all three raters independent of IQ, predicting extra telephone calls (parent, teacher, self) and performance below own capacity (teacher, self). Internalising problems were the reason for extra telephone calls (according to parents) and performance below own capacity (self) independent of IQ score. Main results were similar when children with scores below 70 or above 130 were excluded from the analyses.
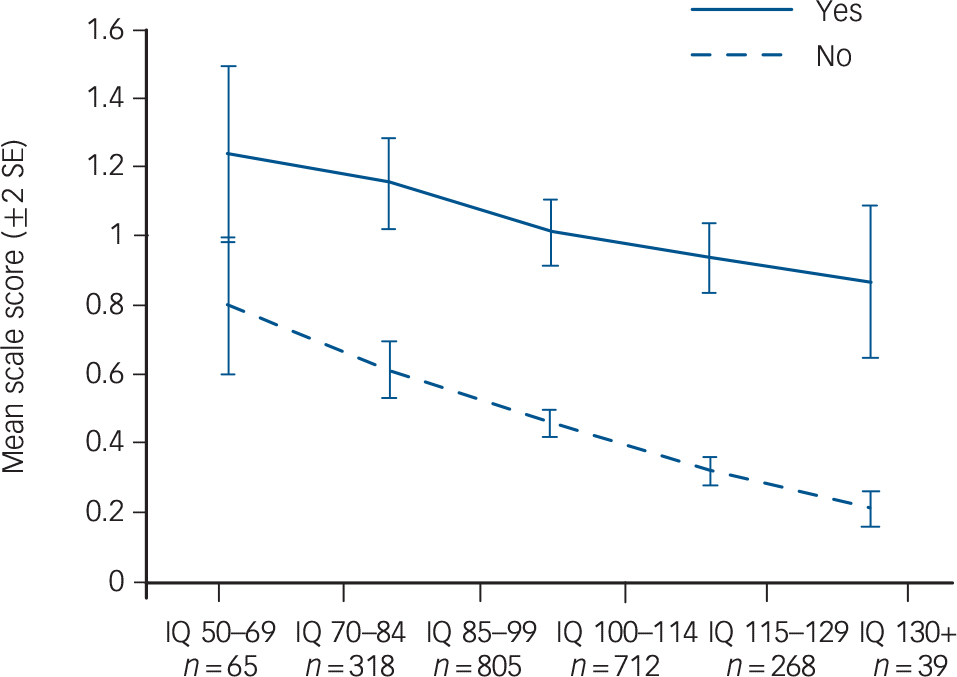
Fig. 3 Effect of teacher-reported attention problems on functional impairment at school for children categorised by IQ score range. Graph indicates whether child performs below own capacity according to teachers: yes, solid line; no, dashed line. Problem scores are means plus or minus 2 standard deviations.
Discussion
This study aimed to contribute empirically to the debate about whether an IQ score trade-off exists in relation to ADHD and related problems by examining whether a high score is related to increased levels of ADHD and other problems, less pervasiveness of problems across situations and less associated functional impairment. To the best of our knowledge, this is the first large, general population-based study employing valid assessment tools for IQ and psychopathology without applying arbitrary cut-offs for both to address this issue. With regard to the first question, of all symptom domains measured IQ score was most strongly and linearly related to attention problems (4.1% explained variance in parent ratings, 8.5% in teacher ratings), with higher scores related to less attention problems compared with lower scores. Similarly (but only according to teachers), smaller effects were found for hyperactivity-impulsivity problems and externalising problems, with lower levels of problems in the high average to high end of the IQ continuum. There was no relationship between IQ score and self-reported problems and only minimally with internalising problems. Thus, results indicate that high IQ scores are related to decreased levels of ADHD problems, predominantly in relation to attention problems. With regard to pervasiveness, of all symptom domains measured IQ score had the strongest influence on rater discrepancy (mean difference in scores) and rater disagreement (correlation between ratings) for attention problems, with more discrepancy and disagreement at the low and high ends of the IQ range v. the mid-range. Parents reported more attention problems than did teachers in children with high estimated IQ scores, whereas the reverse was found for children with low estimated IQ. No such effect was found for rater discrepancy of hyperactivity-impulsivity problems. This suggests that attention problems in highly intelligent children are expressed more and/or noticed more at home than at school compared with children of average intelligence (i.e. less situational pervasiveness) or that attention problems are less easily noticed in these children at school. Finally, with regard to functional impairment, attention problems (followed by externalising problems) were of all symptom domains the strongest predictor of repeating grades and suspected performance below own capacity. Conversely, hyperactivity-impulsivity problems were minimally predictive of functional impairment. Teacher-rated attention problems predicted functional impairments also in the higher IQ range (inattention had functional consequences regardless of IQ level), arguing against the hypothesis that attention problems have fewer functional consequences in highly intelligent children.
Attention v. hyperactivity/impulsivity problems
These results argue against the hypothesis that higher IQ scores may increase the risk of ADHD-like or other problems, as has been argued on the basis mostly of clinical impressions rather than empirical studies. Reference Budding and Chidekel10–Reference Webb, Amend, Webb, Goerss, Beljan and Olenchak12 Both ADHD symptom dimensions, as well as externalising and internalising problems, were lower at the high end of the IQ continuum. These data suggest that this holds more true for attention problems than for problems of hyperactivity-impulsivity. This is in line with previous studies showing that high intelligence scores are particularly related to lower attention problems, Reference Alloway and Elsworth15,Reference Richards, Encel and Shute16,Reference Bracken and Brown25,Reference Gere, Capps, Mitchell and Grubbs26 and potentially to a lesser degree to hyperactivity-impulsivity problems. Reference Alloway and Elsworth15,Reference Ackerman27,Reference Bouchet and Falk28 Moreover, teacher-rated attention problems predicted performance below the child's own capacity also at the higher end of the IQ continuum, suggesting these problems are not merely harmless ‘mimics’ of ADHD. The current and previous studies suggest that high levels of psychopathological symptoms (particularly attention problems) are actually more relatively deviant in highly intelligent individuals than in individuals of below-average intelligence, considering the mean level of attention problems in that IQ range.
Pervasiveness of ADHD problems in children with high IQ
A widely held assumption is that ‘ADHD-mimicking’ traits in highly intelligent individuals can be differentiated from ‘true’ symptoms indicative of ADHD by a lack of situational pervasiveness. That is, these traits are thought to be less pervasive across situations in highly intelligent individuals as a consequence of being situationally linked to a mismatch between the child's cognitive ability and offered stimulation. Reference Budding and Chidekel10–Reference Webb, Amend, Webb, Goerss, Beljan and Olenchak12 Some support for this view was found. Parent-teacher discrepancy and disagreement were higher in the high IQ range than average IQ range (but note the discrepancy was highest in the lowest IQ range), with more attention problems reported by parents compared with teachers as opposed to similar levels of attention problems in the mid IQ range. It may be proposed that school is a cognitively more stimulating environment than home, evoking less attention problems in highly intelligent children. The argument that attention problems in children with high intelligence may easily go unnoticed by teachers and lead to underachievement seems not to be supported by the data, given that there was a negative linear relationship between IQ score and performing below capacity according to teachers and that there were low levels of attention problems reported by teachers in children with high IQ scores. It is of interest, however, that the findings of parent-teacher rater discrepancy regarding attention problems were not paralleled by rater discrepancies for hyperactivity-impulsivity symptoms, which were constant across the IQ range (higher levels reported by parents than teachers). This seems to suggest that situational pervasiveness of hyperactivity-impulsivity symptoms is less linked to IQ in comparison with attention problems.
Strengths and limitations
Strengths of the study include a large, unselected population-based sample, valid assessments of intelligence and psychopathology, the use of multiple raters (parent, teacher, self), measures of functional impairment at school, and use of IQ scores as a continuous measure instead of working with arbitrary cut-off points (IQ groups were only formed for illustrative purposes and post hoc comparisons). A limitation is the narrow age range of the sample preventing analyses on potential age-moderating effects. In addition, only questionnaire data were used instead of diagnostic interview data. However, parent and teacher ratings revealed similar findings and the use of multi-informant questionnaire data allowed us to test explicitly for pervasiveness of problems across situations. Further, we used only two subtests instead of the full battery to estimate IQ. Given that even full IQ tests are not always reliable representations of intelligence, with the possibility that particularly participants with high levels of ADHD symptoms may obtain lower scores due to their symptoms, replication of the findings is needed. However, using two subsets to estimate full-scale intelligence is commonly done in large epidemiological studies and the currently estimated IQ score appeared to be valid, since it robustly related to school performance and SES. Last, only subtests were used that did not rely on working memory, causing a risk of overestimating the IQ scores of children with high levels of attention problems. However, the inverse relationship between IQ score and attention problems suggest this has not been a substantial confounder.






eLetters
No eLetters have been published for this article.