



Introduction
Chronic diseases are heavily influenced by individual lifestyle behaviors. Unhealthy lifestyle behaviors (low physical activity, smoking, etc.) have their roots in childhood and are increasingly prevalent in children. Nudges – interventions rooted in the behavioral sciences – have shown promise in improving lifestyle behaviors in adults, but they have not been tested in children. There are many reasons why nudges may have different levels of acceptability in the pediatric population. This paper uses an online sample of adults to evaluate whether nudges aimed at discouraging smoking or promoting physical activity would be similarly accepted if they targeted adults, parents (in order to influence children's behavior) or children themselves. Adult participants are randomized to one of three conditions (adults – the control condition – parents or children) and are asked whether they find use of those nudges acceptable. I find a high level of acceptability (>75%) for all conditions. After adjusting for sociodemographic factors, there is no statistically significant difference between the three conditions, meaning that nudging parents and children is not perceived significantly differently from nudging adults. These results suggest that when the objective is to improve children's health, adults are accepting of nudging parents and children. This research opens the door to exploring whether this level of acceptability is also found in other domains of medicine and public health where nudges have shown success. More importantly, it suggests the possibility of testing the effectiveness of the proposed nudges to improve health outcomes in children.
Background
Smoking and obesity are among the most significant risk factors for morbidity and early mortality worldwide. The list of negative consequences of smoking is long and includes increased risk of heart attacks and stroke and emphysema, as well as lung, throat and several other cancers (US Department of Health Human Services, 2004). While the smoking rate has decreased in much of the world in the last few decades, the prevalence of tobacco use now plateaus at around 15% in Canada and the USA (Jamal et al., Reference Jamal, Phillips, Gentzke, Homa, Babb, King and Neff2018; Statistics Canada, 2018). The vast majority of current smokers initiated smoking before the age of 18, and the younger the age at initiation, the less likely a person is to succeed in quitting during adulthood (Chen & Millar, Reference Chen and Millar1998; US Department of Health Human Services, 2004).
The prevalence of childhood obesity has increased dramatically over the last three decades, with overweight and obesity now affecting one in four children in Canada and one in three children in the USA (Statistics Canada, 2005, 2013; Skinner et al., Reference Skinner, Ravanbakht, Skelton, Perrin and Armstrong2018). Childhood obesity is a major predictor of adult obesity and a significant risk factor for cardiometabolic diseases resulting in substantial morbidity and mortality and associated health care costs (Barlow & Dietz, Reference Barlow and Dietz2002; Plourde, Reference Plourde2006; Janssen, Reference Janssen2013; Sahoo et al., Reference Sahoo, Sahoo, Choudhury, Sofi, Kumar and Bhadoria2015, Skinner et al., Reference Skinner, Perrin, Moss and Skelton2015). Lifestyle factors, such as low physical activity, have been shown to be important factors in the development and maintenance of overweight and obesity (Lipnowski et al., Reference Lipnowski and Leblanc2012). These unhealthy behaviors have roots in childhood and track into adulthood (Halfon & Hochstein, Reference Halfon and Hochstein2002, Van Cleave et al., Reference Van Cleave, Gortmaker and Perrin2010).
Addressing childhood tobacco use and pediatric obesity is therefore a public health priority in many countries, including the USA (Office of Disease Prevention and Health Promotion, 2014). Given the difficulty of changing unhealthy habits in adults, effective interventions to improve the health behaviors of children represent a significant opportunity for governments and the medical community. This can be achieved by targeting children or parents, who, through access to financial resources and role modeling, have a significant influence on children's behaviors (Ostbye et al., Reference Ostbye, Malhotra, Stroo, Lovelady, Brouwer, Zucker and Fuemmeler2013).
Traditional information campaigns to tackle smoking and physical inactivity have been largely ineffective (Metcalf et al., Reference Metcalf, Henley and Wilkin2012; Peirson et al., Reference Peirson, Ali, Kenny, Raina and Sherifali2016). More coercive interventions, such as regulations and taxes, have had some success in changing behaviors, but many others have faced significant political and legal resistance (Morain et al., Reference Morain, Winickoff and Mello2016; Lee et al., Reference Lee, Falbe, Schillinger, Basu, McCulloch and Madsen2019). Nudges, which are choice-preserving policy options, represent a promising alternative for promoting healthy behaviors in children (Thaler & Sunstein, Reference Thaler and Sunstein2008; Jenssen et al., Reference Jenssen, Buttenheim and Fiks2019). The last few years have seen an exponential growth in the number of interventions rooted in behavioral sciences aimed at promoting socially desirable behaviors, including health-promoting behaviors (Marteau et al., Reference Marteau, Ogilvie, Roland, Suhrcke and Kelly2011; Halpern et al., Reference Halpern, Asch and Volpp2012; Loewenstein et al., Reference Loewenstein, Asch, Friedman, Melichar and Volpp2012; Vallgarda, Reference Vallgarda2012; Milkman et al., Reference Milkman, Minson and Volpp2013; Halpern et al., Reference Halpern, French, Small, Saulsgiver, Harhay, Audrain-McGovern, Loewenstein, Brennan, Asch and Volpp2015; Hansen et al., Reference Hansen, Skov and Skov2016; Reisch et al., Reference Reisch, Sunstein and Gwozdz2017). This approach has seldom been tested in pediatrics.
At the same time, a growing body of literature suggests that cognitive biases contribute to smoking and physical inactivity, suggesting that nudges could be effective. Previous studies in the USA have shown that adults who smoke perceive their risk of tobacco-related diseases to be higher than non-smokers but lower than other ‘average’ smokers (Hahn & Renner, Reference Hahn and Renner1998). A majority of parents believes their children are at lower risk of initiating smoking than the average child, even among parents who smoke (Chadi et al., Reference Chadi, Winickoff and Drouin2019; Drouin et al., Reference Drouin, Winickoff and Thorndike2019a). This optimism bias could help explain why traditional educational approaches have proven ineffective: parents who believe that their children are not likely to start smoking have little motivation to limit their children's exposure to risk factors. There is also some evidence that children themselves display optimism bias with regards to several unhealthy behaviors, including smoking (Whalen et al., Reference Whalen, Henker, O'Neil, Hollingshead, Holman and Moore1994).
Prospect theory predicts that framing of rewards for physical activity as gains or losses would influence physical activity, which was previously demonstrated in adults (Volpp et al., Reference Volpp, John, Troxel, Norton, Fassbender and Loewenstein2008; John et al., Reference John, Loewenstein, Troxel, Norton, Fassbender and Volpp2011). In children, preliminary findings suggest that health message framing (gain versus loss frame) directed at parents may influence physical activity in children (Drouin et al., Reference Drouin, Young and King2018). Nudges could be effective in tackling smoking and physical inactivity in children, yet this approach has so far not been explored.
Before nudges can be tested and used, it is important to determine whether they are acceptable to the general public. In most democracies, a majority of adults finds the use of nudges acceptable (Sunstein et al., Reference Sunstein, Reisch and Rauber2018). However, a non-insignificant number still opposes their use, especially for ‘personal’ decisions, such as health-related behaviors (Blumenthal-Barby & Burroughs, Reference Blumenthal-Barby and Burroughs2012; Aggarwal et al., Reference Aggarwal, Davies and Sullivan2014; Sunstein et al., Reference Sunstein, Reisch and Rauber2018). People may also believe that influencing health behaviors is not the role of government, preferring for this task to be carried out by clinicians who they know and trust. Using nudges in clinical care is a relatively new, very contentious idea (Halpern et al., Reference Halpern, Ubel and Asch2007; Swindell et al., Reference Swindell, McGuire and Halpern2010; Blumenthal-Barby & Burroughs, Reference Blumenthal-Barby and Burroughs2012; Li & Chapman, Reference Li and Chapman2013; Navin, Reference Navin2017). Recent reports suggest that public acceptability of nudges is influenced not only by the mechanism of influence, but also, and perhaps most importantly, by the given nudge's policy objective (Tannenbaum et al., Reference Tannenbaum, Fox and Rogers2017). Nudges aimed at policy objectives that represent near-consensus positions should thus have high acceptability within a given population. Public health issues affecting children, such as teenage smoking and pediatric obesity, may well elicit consensus positions.
There is an ongoing ethical debate surrounding the use of nudges in public policy (Sunstein & Thaler, Reference Sunstein and Thaler2003; Whyte et al., Reference Whyte, Selinger, Caplan and Sadowski2012; Bubb & Pildes, Reference Bubb and Pildes2013; Rebonato, Reference Rebonato2014). While a detailed review of the ethical arguments in this debate is beyond the scope of this paper, it is worth noting the most common concerns about nudges, including their potential to undermine autonomy and dignity (Sunstein, Reference Sunstein2015). By taking advantage of unconscious biases, nudges are invisible to the person being nudged, and as such can be considered manipulative (Rebonato, Reference Rebonato2014). Paternalism is another concern. Nudges are developed by policymakers based on their perception of a group's best interest, and these are then imposed from above. Coercion, erosion of freedom of choice and the insulting nature of paternalism are all well-known critiques (Cornell, Reference Cornell2014).
Examining the acceptability of nudges through an ethical lens would suggest differing levels of acceptability for different types of nudges. This hypothesis is supported by empirical evidence (Reynolds et al., Reference Reynolds, Archer, Pilling, Kenny, Hollands and Marteau2019). Provision of information is considered a nudge by some (Sunstein, Reference Sunstein2015; Reisch et al., Reference Reisch, Sunstein and Gwozdz2017). In empirical studies, such nudges generally have broad support (Petrescu et al., Reference Petrescu, Hollands, Couturier, Ng and Marteau2016; Reisch et al., Reference Reisch, Sunstein and Gwozdz2017), due in part to the fact that this approach is transparent, non-manipulative and generally not perceived as paternalistic. On the other end of the spectrum, some have argued that concerns about autonomy are outweighed by the importance of certain health problems, and that policy options such as taxes and bans that are more coercive than nudges are not only justified, but required (Conly, Reference Conly2012). Beyond theoretical arguments, studying the acceptability of policies, including nudges, is also important given the role that acceptability plays on the adoption of policies (Cullerton et al., Reference Cullerton, Donnet, Lee and Gallegos2016; Reynolds et al., Reference Reynolds, Archer, Pilling, Kenny, Hollands and Marteau2019).
Until now, most of the arguments made for and against nudges have focused on changing the behaviors of competent adults. Ethical and political arguments take on a new dimension if nudges are aimed at the behaviors of children and parents. Children and adolescents’ ongoing neurocognitive development (Steinberg, Reference Steinberg2008) as well as parents’ generally lower risk tolerance for their children than for themselves are two reasons for which nudges that are deemed acceptable for adults might not be considered acceptable for children (Hammitt & Haninger, Reference Hammitt and Haninger2010).
It is important to determine whether nudges aimed at parents and children would be acceptable to the general population and to parents specifically. I test whether the acceptance of nudges varies depending on whether they target adults, parents or children. The hypothesis is that a majority of participants will find nudges targeting children and parents as acceptable as nudges targeting adults for the policy objectives chosen.
Methods
Study design and population
This study is a three-arm, cross-sectional, randomized trial. Participants aged 18 and over and living in the USA were recruited through Amazon's Mechanical Turk platform between March 21 and March 30, 2017 (Buhrmester et al., Reference Buhrmester, Kwang and Gosling2011; Crump et al., Reference Crump, McDonnell and Gureckis2013). Each participant received minor monetary compensation for taking the survey. The average completion time was less than five minutes.
Exposure and outcome
In this study, four scenarios are presented to each adult participant. The study flow is presented in Figure 1. In the first scenario, participants are presented with a hypothetical situation in which the government aims to correct an over-optimism bias as a strategy to help with smoking cessation – an example of a transparent System 2 nudge (Hansen & Jespersen, Reference Hansen and Jespersen2013; Sunstein, Reference Sunstein2016a). In the second scenario, the intervention is the same, but participants are asked to imagine that the strategy is used by a physician they know rather than by the government. The third and fourth scenarios concern the use of message framing to increase physical activity – an example of a non-transparent System 2 nudge (Hansen & Jespersen, Reference Hansen and Jespersen2013). Similarly to the smoking cessation nudge, one scenario describes the nudge as being used by the government, while in the second scenario it is used by a physician who the participants know.

Figure 1. Study design.
Before starting each block of two scenarios, each adult participant is randomized to one of three conditions. In the first condition, the nudge in the scenario is aimed at adults. For example: “Imagine that research has shown that adults are more likely to exercise if they are told about the benefits of physical activity (rather than the risks of being inactive). Knowing this, do you believe it would be acceptable for a public health campaign by the government to emphasize the benefits of physical activity to the population?” This scenario serves as the control condition.
In the second condition, the nudge is described as being aimed at adults, but in an explicit attempt to change the behavior of children. For example: “Imagine that research has shown that children are more likely to exercise if their parents are told about the benefits of physical activity for children (rather than the risks of being inactive). Knowing this, do you believe it would be acceptable for a public health campaign by the government to parents to emphasize the benefits of physical activity for children?”
Finally, in the third condition, the nudge is presented as directly targeting children in an effort to change their behavior. For example: “Imagine that research has shown that children are more likely to exercise if they are told about the benefits of physical activity (rather than the risks of being inactive). Knowing this, do you believe it would be acceptable for a school to emphasize the benefits of physical activity to the children attending the school?”
The scenarios are based on previous publications showing that parents who smoke display over-optimism as much about the health effects on their children as on the effects on their own health (Weinstein et al., Reference Weinstein, Marcus and Moser2005; Drouin et al., Reference Drouin, Winickoff and Thorndike2019a).
Other studies show that parents exposed to a loss-frame message about the health effects of exercise on children report a significantly greater change in their children's level of physical activity at follow-up compared to parents exposed to a gain-framed message (Drouin et al., Reference Drouin, Young and King2018).
Following the description of each practice or policy, participants are asked whether they deem each policy acceptable or unacceptable, using a single dichotomous answer (acceptable versus not acceptable) (Evans et al., Reference Evans, Finkelstein, Kamerow and Renaud2005; Sikorski et al., Reference Sikorski, Luppa, Schomerus, Werner, Konig and Riedel-Heller2012; Lykke et al., Reference Lykke, Pisinger and Glumer2016; Sunstein et al., Reference Sunstein, Reisch and Rauber2018).
Covariates
In this experiment, the following covariates are collected for each participant: age, gender, parental status (parent versus not a parent), age category of the child (<1, 1–5, 6–12, 13–17, 18+ years old), participant's smoking status (current smoker, past smoker, non-smoker), participant's perceived relative health status (five-point scale from much less healthy than average to much more healthy than average), participant's perceived relative physical activity level (five-point scale from much less active than average to much more active than average), political ideology (five-point scale from very liberal to very conservative) and party affiliation (seven-point scale from strong democrat to strong republican).
Analysis plan and statistical methods
χ 2 tests are used to evaluate possible differences in acceptance rates between nudge targets (adults versus parents versus children) for each scenario. In order to determine whether any difference in the acceptability of nudges across targets is attributable to certain covariates, as well as to examine whether any of the covariates predicted the acceptability of nudges, two separate multivariable logistic regression models are used: one for the acceptability of nudging parents and another for the acceptability of nudging children, using the ‘nudging adults’ condition as the reference. For each model, the outcome is the acceptability of the nudges and the main predictor is the nudge target population. Serial models using an increasing number of covariates were created. The first model adjusts only for parental status and nudge ‘messenger’. The second model adjusts for the previous variables, the age and gender of participants and the age of the child. The final model adjusts for political affiliation and party affiliation, in addition to the previous covariates. A standard threshold of p < 0.05 for statistical significance is used. All statistical analyses are performed using SAS 9.4 (Cary, NC).
Results
The sample consists of 211 adult participants. The demographics of the sample are presented in Table 1. Briefly, the mean age of adult participants is 39.9 years (range 18–66 years), 68% of respondents are female, 54% are parents and the participants are equally distributed along the conservative/republican to liberal/democrat axis (Table 1).Footnote 1
Table 1. Participants’ characteristics (n = 211).

A majority of adult participants approves of the correction of over-optimism as a strategy for government to promote smoking cessation in adults (Figure 2), and there is no statistically significant difference in approval rate of the same strategy when aimed at teenagers directly. However, a smaller proportion of participants approves of the use of the same nudge to target parents (96% for adults versus 94% for teenagers versus 76% for parents, χ 2 p-value < 0.001). Use of the same strategy by physicians is also supported by a majority of participants, whether the nudge is aimed at adults, parents or teenagers (approval rate of 97% versus 87% versus 93%, respectively; p = 0.08) (Figure 2).
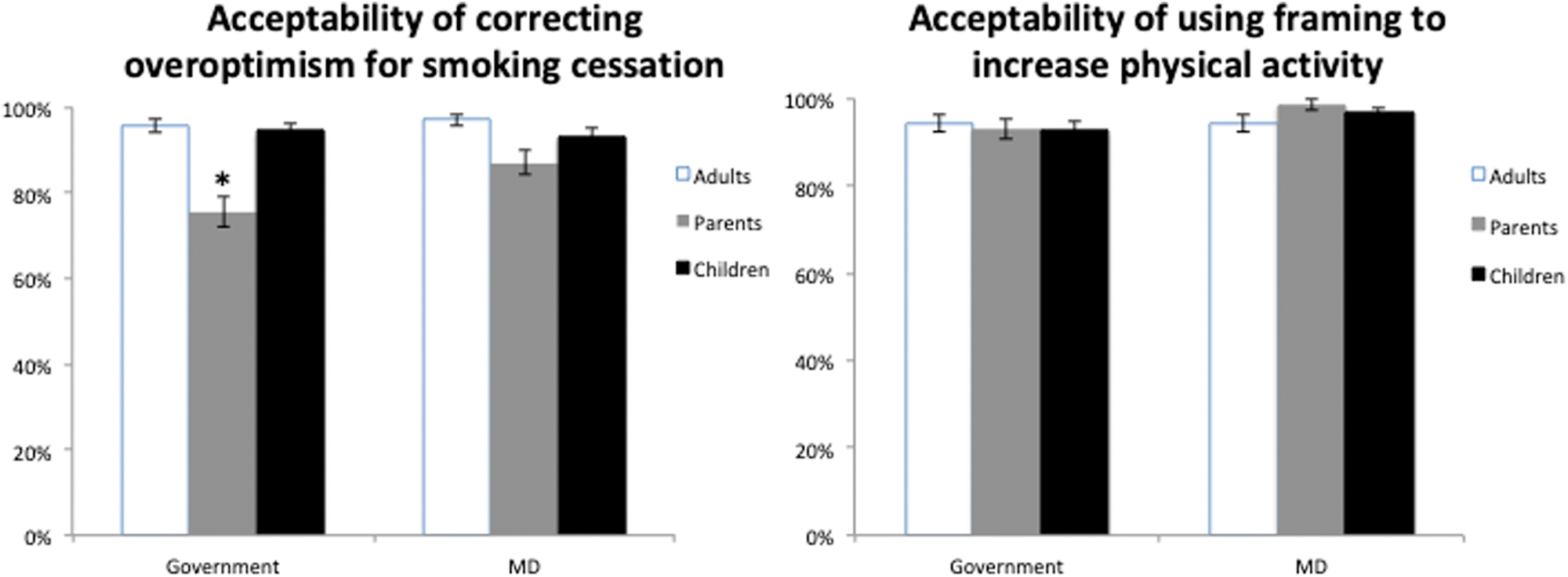
Figure 2. Acceptability of two types of nudge for three target populations, divided by messenger of the nudge. *p < 0.05. MD = physician.
A majority also supports using message framing to promote physical activity, whether the nudge comes from the government (94% for adults versus 93% for parents versus 93% for children; p = 0.92) or from physicians (94% for adults versus 97% for parents versus 99% for children; p = 0.36) (Figure 2).
Using a univariate screen, variation in the acceptability of nudging parents or children according to sociodemographic characteristics is measured. Adult participants who identify as liberal are significantly more likely to accept the use of a nudge targeting parents compared to moderates (unadjusted odds ratio (uOR) = 6.33, 95% confidence interval (CI) = 1.70–22.37) (Table 2). All other covariates are not significant predictors of the acceptability of nudges targeting parents. With regards to predictors of the acceptability of nudges targeting children, only older age (uOR = 1.07 for each additional year, 95% CI = 1.01–1.13) emerges as a significant predictor among the sociodemographic characteristics studied (Table 3).
Table 2. Unadjusted odds ratio of reporting nudging parents as acceptable.

(Reference) = reference category for calculation of the odds ratio, representing a value of 1.00.
*p < 0.05.
NA = not available (i.e., small sample size for this subgroup precludes calculation of reliable estimate).
Table 3. Unadjusted odds ratio of reporting nudging children as acceptable.

(Reference) = reference category for calculation of the odds ratio, representing a value of 1.00.
* p < 0.05.
NA = not available (i.e., small sample size for this subgroup precludes calculation of reliable estimate).
Finally, multivariable models are used to evaluate the acceptability of nudging parents and children compared to adults (the control, or reference point). In the first model, correcting over-optimism is considered to be more acceptable for nudging parents than adults in general in the unadjusted analysis (odds ratio (OR) = 4.32, 95% CI = 1.37–13.58) (Table 4). This relationship remains significant after adjusting for whether or not the participant is himself/herself a parent. While the effect size remains large, the relationship becomes non-statistically significant once adjusted for other sociodemographic characteristics (Table 4). Conversely, using framing to increase physical activity is not more or less acceptable when it targets parents compared to adults in general, in both unadjusted and adjusted analyses (Table 4).
Table 4. Odds ratio of reporting nudging parents as being acceptable (compared to adults).

a Model adjusted for parental status + messenger.
b Model 1 + age, gender and age of the child.
c Model 2 + political ideology and party affiliation.
* p < 0.05.
CI = confidence interval.
A second multivariate model is used to test the acceptability of nudges targeting children, using nudges targeting adults as the reference. For both types of nudges, the odds of reporting the nudge as being acceptable are the same whether children or adults are targeted. This is true across nudge types in both the unadjusted and the adjusted analyses, although the sample size limits the capacity to perform the fully adjusted analysis (Table 5).
Table 5. Odds ratio of reporting nudging children as being acceptable (compared to adults).

a Model adjusted for parental status + messenger.
b Model 1 + age, gender and age of the child.
c Model 2 + political ideology and party affiliation.
CI = confidence interval; NA = not available (i.e., small sample size for this subgroup precludes calculation of reliable estimate).
Discussion
In this study, I find that adult participants accept the idea of nudging parents to improve two child health behaviors. Similarly, a majority also accepts the use of nudges targeting children for the same purpose. Despite theoretical and ethical objections, it appears that the vast majority of adults does not disapprove of using nudges to target parents and children (Swindell et al., Reference Swindell, McGuire and Halpern2010; Blumenthal-Barby & Burroughs, Reference Blumenthal-Barby and Burroughs2012; Navin, Reference Navin2017).
This study expands on previous research showing broad support for a nudge approach to tackling important social problems. The level of support in this study is of similar magnitude to findings from other studies in adults. Sunstein shows approval rates of between 57% and 96% for food- and cigarette-related nudges (Sunstein, Reference Sunstein2016a). He also finds only modest differences in approval between sexes, for all ages and across the political spectrum, similarly to this study. Reynolds et al. find slightly lower levels of support for nudges aimed at reducing tobacco, alcohol and snack consumption, with support ranging from 52% to 89% (Reynolds et al., Reference Reynolds, Archer, Pilling, Kenny, Hollands and Marteau2019). Examining nudges to reduce sugar-sweetened beverage consumption in US and UK samples, Petrescu et al. find acceptability rates ranging from 50.0% to 67.6% (Petrescu et al., Reference Petrescu, Hollands, Couturier, Ng and Marteau2016). Finally, Reisch et al. find that a majority of Europeans supports health nudges, with a range of 52–90% depending on the country for information nudges (nudges most similar to those tested in this study). Interestingly, use of a nudge to address childhood obesity is supported by a greater number, with acceptability ranging from 81% to 90% (Reisch et al., Reference Reisch, Sunstein and Gwozdz2017).
This experiment has some limitations. It uses a convenience sample of adult participants recruited online, which may not be representative of the general population. However, the sample was restricted to US residents in an attempt to improve external validity. The sample obtained was also varied, both in terms of age and political views, thus strengthening the conclusions. This experiment is limited to the acceptability of two nudges to reduce teenage smoking and pediatric obesity. It is not known whether the wide acceptability found in this study applies to other health behaviors that are more contentious, politicized and potentially polarizing (i.e., vaccination) or to behaviors that are perceived as less risky or have lower yields (i.e., sunscreen use, reducing screen time or bicycle helmet use). It is not possible to extrapolate the findings here to other types of nudges that may generally be more acceptable (i.e., information labels) or less acceptable (i.e., non-transparent defaults). This study comments on the acceptability of nudges on their own, not in comparison with other policy tools (i.e., provision of information, financial incentives or mandates). As such, this study is closer to a separate evaluation than to a joint evaluation. This approach has previously been used in the study of the acceptability of nudges (Sunstein et al., Reference Sunstein, Reisch and Rauber2018). Others have used a comparative or joint evaluation approach (Petrescu et al., Reference Petrescu, Hollands, Couturier, Ng and Marteau2016), which some authors have argued against (Davidai & Shafir, Reference Davidai and Shafir2018).
The study design does not allow for comparison of nudge acceptability based on the messenger (government versus physician), the type of nudge (System 1 versus System 2, or transparent versus non-transparent) or the target behavior. Future work could randomize participants based on those variables to examine whether they are important determinants of acceptability (Petrescu et al., Reference Petrescu, Hollands, Couturier, Ng and Marteau2016; Sunstein, Reference Sunstein2016b).
This study's results open the door to a more comprehensive evaluation of the acceptability of nudges to promote healthy behaviors influencing child health. There have been some ethical and conceptual publications on the acceptability of nudges targeting parents and children (Harbach, Reference Harbach2016; Blumenthal-Barby & Opel, Reference Blumenthal-Barby and Opel2018), but this study is the first to empirically test acceptability in the pediatric context. In addition to examining whether the results presented here apply to other nudge types and other behaviors, testing nudge acceptability of child health behaviors among children themselves would be another interesting avenue for future research.
Studying the effect of acceptable nudges with a known effect in adults on behavior changes in children is another promising direction for future research. So far, few nudges have been applied to both parents and children, even if some have advocated for their potential (Stevens, Reference Stevens2014; Jenssen et al., Reference Jenssen, Buttenheim and Fiks2019). In one study, financial incentives are used to create a habit of eating more vegetables among schoolchildren (Loewenstein et al., Reference Loewenstein, Price and Volpp2016). Providing a small financial incentive to schoolchildren doubles the proportion of children eating at least one fruit or vegetable at lunch and, with a treatment period of three to five weeks, a partial effect remains after two months. Another study uses a brief social norms intervention to target parents, leading to an increase in booster seat usage (Jeffrey et al., Reference Jeffrey, Whelan, Pirouz and Snowdon2016). In the field of education, one study finds that reminders to parents in the form of text messages improve parent–child academic interactions and children's reading abilities (Doss et al., Reference Doss, Fahle, Loeb and York2018).
Given that previous research has identified parents as potential targets for nudges to promote healthy behaviors in children (Drouin et al., Reference Drouin, Young and King2018, Reference Drouin, Winickoff and Thorndike2019a, Reference Drouin, Winickoff and Thorndike2019b), the time has come for empirical testing of such nudges’ efficacy.
Conclusion
This paper aims to determine whether nudges targeted at parents and children are acceptable. Using an online sample of adults and two nudge scenarios, findings show that, when the goal is to improve children's health, nudges targeting parents and children have high levels of acceptability, which are not significantly different from those for nudges targeting adults. Most adult participants report that using nudges to promote healthy behaviors in children is acceptable, whether the nudges target parents or children. The proposed nudges are acceptable whether they come from clinicians or governments. For policymakers, these results suggest the possibility of testing nudges to tackle the major challenges of teenage smoking and childhood physical activity, especially given the limited success of traditional public health approaches on both fronts. For health care practitioners, this study opens the door to using nudges in clinical encounters as an alternative way to help patients and families adopt healthier lifestyle behaviors. Next steps in this line of research include exploring the level of acceptability for other nudge types and policy domains, as well as testing the effectiveness of the proposed interventions.
Acknowledgments
The author would like to thank Professor Cass Sunstein for encouragement in conducting this study.
Conflict of interest
The author has no financial relationships relevant to this article to disclose.







