


The prevalence of overweight and obesity is increasing rapidly, especially in higher-income countriesReference Lobstein and Frelut1, Reference Jolliffe2. Body weight and body composition in childhood are important determinants of overweight in adulthoodReference Rimm and Rimm3–Reference Janssen, Katzmarzyk, Srinivasan, Chen, Malina and Bouchard6. There is increasing evidence that the development of overweight and obesity in children has deleterious social and health consequencesReference Livingstone7. In Italy, 15–25% of children under 18 years of age are already classed as overweight or obeseReference Maffeis, Talamini and Tatò8–Reference Celi, Bini, De Giorgi, Molinari, Faraoni and Di Stefano12.
In describing the nutritional status of a population, the body mass index (BMI) represents the most complete indicator and, at the same time, is the easiest to use. In particular, it is known that in all infant ages body fat is better correlated with the BMI than with other indicatorsReference Cole and Himes13–Reference Scholler15. The International Obesity Task Force (IOTF) recommends cut-off points for BMI in childhood that are based on international data and linked to the widely accepted adult cut-off pointsReference Cole, Bellizzi, Flegal and Dietz16. In order to effect appropriate public health measures for the treatment and prevention of childhood overweight and obesity, accurate estimates of these prevalences are required. The aim of the present study was to provide regional estimates for overweight and obesity in school-aged children residing in Veneto Region, Italy.
Subjects and methods
Veneto is a region in the north-east of Italy with a population of 4 527 694 inhabitants in 200117; children 9 years of age who attend 3rd year primary schools (born in 1995) numbered 39 525 and children of 11 years of age who attend 5th year primary schools (born in 1993) numbered 39 825.
Relevant data of primary schools (name, location and number of students attending the 3rd and 5th years) were obtained from the local education authorities. Schools were randomly sampled in the reference territory of the local health authorities until reaching 20% of the students of the 3rd year and of the 5th year.
The ‘Service of Food Hygiene and Nutrition’ of each local health authority registered measurements of the children’s weight and height during the period April–June 2004. In order to acquire the competences necessary for correct registration of the anthropometric measurements, the people involved – 45 operators in all – participated in the ‘Course in surveying anthropometrical indexes’ held at the Department of Environmental Medicine and Public Health at Padua University.
The same height stand and scales were used throughout the study. Weight was measured to the nearest 0.1 kg using electronic scales (Wunder). Height was measured to the nearest 0.1 cm using a portable stadiometer (Seca). The instruments used were calibrated before every measuring session. During the measuring the children wore underclothes only and were barefoot.
The measurements obtained were registered and sent to the Laboratory of Environmental Epidemiology at the Department of Environmental Medicine and Public Health at Padua University.
BMI was calculated as body weight divided by the square of body height. To define overweight and obesity, the sex- and age-specific BMI cut-offs recommended by the IOTF were usedReference Cole, Bellizzi, Flegal and Dietz16. This is based on average percentiles, which equate to a BMI of 25 or 30 kg m−2 at age 18 years for overweight or obesity, respectively. Here, obesity is defined as BMI on or above the obesity cut-off, while overweight is a BMI on or above the overweight cut-off and below the obesity cut-off.
Statistical methods
The sample examined was subdivided into three groups representing the different realities of the Veneto Region: rural areas, urban areas and mountain areas (local communes of the mountain territory identified with regional laws18).
The results are presented as crude cross-sectional prevalence (95% confidence limits) of overweight and obesity. The odds ratio and 95% confidence interval (OR, 95% CI) was used for the univariate comparisons. The Mantel–Haenszel method was used to examine differences between different geographical areas stratifying the sample by sex and age.
Results
The total number of measurements taken in Veneto was 13 234 (6510 girls and 6724 boys), the number of valid (corrected by year born) measurements was 12 832 (6311 girls and 6521 boys). Subjects aged 9 years numbered 6508 (16.88% of the same aged Veneto population), subjects aged 11 years numbered 6345 (16.37% of the same aged Veneto population). The characteristics of the sample are summarised in Table 1.
Table 1 The characteristics of the sample
Among boys the prevalence of overweight was 21.06%, while obesity prevalence was 5.92%; among girls overweight prevalence was 21.30%, while obesity prevalence was 5.15%. Tables 2 and 3 show the prevalence of overweight and obesity among our population subdivided by age, sex and geographical area.
Table 2 Prevalence of overweight and obesityFootnote * according to sex and age

* Overweight is defined as body mass index (BMI) on or above the overweight cut-off and below the obesity cut-off of the International Obesity Task Force (IOFT); obesity is defined as BMI on or above the IOTF obesity cut-off.
Table 3 Prevalence of overweight and obesityFootnote * according to sex, age and geographical area
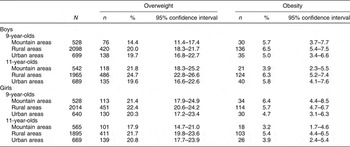
* Overweight is defined as body mass index (BMI) on or above the overweight cut-off and below the obesity cut-off of the International Obesity Task Force (IOFT); obesity is defined as BMI on or above the IOTF obesity cut-off.
When comparing the results according to sex and age, a significant difference was observed for: the prevalence of overweight, which was higher among 11-year-old boys (OR = 1.21; 95% CI: 1.09–1.36) than 9-year-old boys; the prevalence of overweight plus obesity, which was higher among boys aged 11 years (OR = 1.19; 95% CI: 1.06–1.33) than girls of the same age; and the prevalence of overweight plus obesity, which was higher among girls aged 9 years (OR = 1.13; 95% CI: 1.01–1.26) than among boys of the same age.
These results suggest a positive trend with age in boys and a negative trend in girls. Comparison of the combined prevalence of overweight and obesity in the three different geographical areas revealed a higher risk for children resident in rural areas, both in relation to those resident in mountain areas18 (Mantel–Haenszel OR = 1.27; 95% CI: 1.13–1.42; χ 2 = 17.55; P < 0.0001) and those resident in urban areas (Mantel–Haenszel OR = 1.18; 95% CI: 1.07–1.31; χ 2 = 10.39; P < 0.001). Comparing the combined prevalence of overweight and obesity among children from urban areas and from mountain areas, no significant differences were found.
Discussion
The results obtained in this study are the most recent and indeed the only available data on overweight and obesity in children of Veneto Region. These data, concerning representative samples of 9- and 11-year-old children, provide an important baseline from which to study future trends in overweight and obesity, to address preventive interventions and to monitor the impact of public health strategies.
The research gave to all Services of Food Hygiene and Nutrition of Veneto Region the opportunity to acquire a rigorous and reproducible methodology that will be useful to future studies.
This paper has highlighted a high prevalence of overweight and obese children in Veneto Region, in line with the high prevalence registered in southern European countriesReference Livingstone7, Reference Chinn and Rona19–Reference Will, Zeeb and Baune22. A lower prevalence in the northern regions of Italy with respect to that of central ItalyReference Celi, Bini, De Giorgi, Molinari, Faraoni and Di Stefano12 is confirmed.
Similar levels of overweight plus obesity were seen in boys and girls. Comparing the prevalence of overweight plus obesity by gender and age group, the results suggested a positive trend with age in boys and a negative trend in girls. However, there is a relationship between puberty and BMI that may affect the performance of the cut-off points in the age group considered. Pubertal growth acceleration starts with hormonal and physical modifications in children between the ages of 8 and 12 years, in both genders. Several studies have documented a change in body fat as girls progress through puberty, during which time a larger fat deposition is described. In addition, obesity is an important contributing factor to the earlier onset of puberty in girls. In boys puberty is characterised by a greater development of skeletal-muscle massReference Maffeis, Talamini and Tatò8, Reference Bini, Celi, Berioli, Bacosi, Stella and Giglio23, Reference Kaplowitz, Slora, Wasserman, Pedlow and Herman-Giddens24.
A significantly higher prevalence of overweight and obesity was found in children living in rural areas when comparing the combined prevalence of overweight and obesity by residential location (urban, rural, mountainous). The highest prevalence of overweight and obesity in rural areas has been described by other authorsReference Plotnikoff, Bercovitz and Loucaides25, 26; in particular, it was identified for Italian adults.
Differences in overweight and obesity prevalence are related to many variables such as dietary intake, physical activity, family history of obesity and social class; these factors were not investigated in the present study, making it inappropriate to discuss possible causes of overweight and obesity in this populationReference De Spiegaelere, Dramaix and Hennart27–Reference Haas, Lee, Kaplan, Sonneborn, Phillips and Liang29. In particular, the reason for the geographical differences is not entirely clear at present.
Conclusion
This is the first time that the prevalences of overweight and obesity have been estimated in children in Veneto Region. These data are essential in order to monitor trends in prevalence and will form the basis for public health initiatives designed to increase children’s health. The strength of the study lies in the large sample size. More research is needed to determine the origin of differences observed by geographical area.
Acknowledgements
The authors wish to thank all co-workers, teachers, parents and children. They are grateful to the clinical and administrative staff of the Veneto Region’s health authorities. Thanks also to the Veneto Region Administration for financial support.



