



Introduction
Schools and workplaces are inherently social environments. It is well established that childhood and adolescent social skills and prosocial behaviors – often referred to broadly as social competence – are key predictors of positive objective outcomes in adulthood (Burt et al., Reference Burt, Obradović, Long and Masten2008; Romppanen et al., Reference Romppanen, Korhonen, Salmelin, Puura and Luoma2021). Social competence in childhood and adolescence promotes positive developmental cascades that increase the likelihood of normative success (i.e., full-time employment, independent residential status, friends, and romantic relationships) in adulthood (Masten et al., Reference Masten, Desjardins, McCormick, Kuo and Long2010).
Social competence is not a static construct; rather, it changes across development (Masten & Cicchetti, Reference Masten and Cicchetti2010). Attachment forms the earliest foundation for social competence; secure attachment is associated with increased peer acceptance and social reasoning skills in childhood (Groh et al., Reference Groh, Fearon, Bakermans-Kranenburg, van IJzendoorn, Steele and Roisman2014; Veríssimo et al., Reference Veríssimo, Santos, Fernandes, Shin and Vaughn2014). In school-age children, social competence is typically conceptualized as encompassing friendship quantity and quality, peer relationships, and prosocial behavior (Eisenberg et al., Reference Eisenberg, Carlo, Murphy and van Court1995; Obradović & Hipwell, Reference Obradović and Hipwell2010), but the relative importance of each of these elements may shift with age (Masten et al., Reference Masten, Desjardins, McCormick, Kuo and Long2010). Many studies of social competence in childhood include peer nomination or classroom reputation measures (Masten et al., Reference Masten, Burt, Roisman, Obradovic, Long and Tellegen2004); in contrast, studies of social competence in adolescence prioritize friendship quality (Kamis & Copeland, Reference Kamis and Copeland2020; Obradović & Hipwell, Reference Obradović and Hipwell2010), and studies of social competence in young adults often emphasize the presence and quality of romantic relationships (Schulenberg, Sameroff, et al., Reference Schulenberg, Sameroff and Cicchetti2004). There is also recognition that competence is comprised of culturally specific skills, reflecting the norms of an individual’s society and community (Arnold & Lindner-Müller, Reference Arnold and Lindner-Müller2013). In other words, a holistic conceptualization of social competence should consider individual variation accounting for person-level factors. Developmental history is one such factor.
Efforts to define social competence in autism spectrum disorder (ASD) have been limited primarily to young children and specific contexts (e.g., the school-based intervention Re-making Recess; Kretzmann et al., Reference Kretzmann, Shih and Kasari2015; Shih et al., Reference Shih, Dean, Kretzmann, Locke, Senturk, Mandell, Smith and Kasari2019). These efforts have not provided much information about the relationships between social competence and adult outcomes in this population. Autism is characterized by major deficits in social communication as well as the presence of sensory or restricted, repetitive interests (American Psychiatric Association, 2014). Social communication impairments in ASD can include deficits in eye contact, limited use of facial expressions and gestures, and difficulty maintaining relationships (APA, 2014). Autism is typically diagnosed in childhood; however, it is a lifelong condition. Currently, about 1 in 36 children in the USA have a diagnosis of autism (Maenner, Reference Maenner2023), though the worldwide prevalence of the disorder is thought to be closer to 1 in 100 children (Zeidan et al., Reference Zeidan, Fombonne, Scorah, Ibrahim, Durkin, Saxena, Yusuf, Shih and Elsabbagh2022). The behavioral phenotype of ASD is not static; symptoms of ASD may change considerably across development (Bal et al., Reference Bal, Kim, Fok and Lord2019). In recognition of mixed preferences for person-first vs. identity-first terminology, we refer to this population interchangeably as “individuals with autism” and “autistic individuals.”
Though ASD is defined in large part by impairments in social development, an autism diagnosis does not preclude the ability to engage in meaningful, adaptive social behaviors. Importantly, the social impairments associated with ASD do not necessarily impact all realms of social functioning, or at least, do not impact all realms of social functioning equally (Anderson et al., Reference Anderson, Oti, Lord and Welch2009; McChesney & Toseeb, Reference McChesney and Toseeb2018). Though some socially-impairing aspects of ASD – such as narrative skills, prosody, and eye contact – may often be resistant to change, individuals with autism can display social competence through other behaviors such as sharing, cooperation, and use of emotional coping skills. Thus, some aspects of social competence could promote positive developmental cascades for autistic individuals.
Social competence & adult outcomes in ASD
Given the impressive body of work typifying social difficulties in ASD (Lord et al., Reference Lord, Charman, Havdahl, Carbone, Anagnostou, Boyd, Carr, Vries, Dissanayake, Divan, Freitag, Gotelli, Kasari, Knapp, Mundy, Plank, Scahill, Servili, Shattuck and McCauley2022) and investigating methods for improving social skills in autistic individuals (Gates et al., Reference Gates, Kang and Lerner2017), the lack of literature on social competence in autism is surprising. Few studies characterize longitudinal change in social skills from childhood to adulthood in autism, and little work has attempted to replicate findings from typical development that adolescent social competence predicts positive adult outcomes in autistic samples. Many adults with ASD experience difficulty achieving normative outcomes (Howlin & Magiati, Reference Howlin and Magiati2017). Specifically, autistic adults have difficulty securing employment and living independently, and experience increased rates of social isolation, including fewer friendships and romantic relationships, compared to typical peers (Orsmond et al., Reference Orsmond, Shattuck, Cooper, Sterzing and Anderson2013; Taylor, Center, et al., Reference Taylor, Center and Mailick2014). Characterizing social competence in ASD and examining longitudinal relationships between social competence and adult outcomes has important implications for understanding and improving well-being in autistic adults.
Historically, empirical investigations of young adulthood in the general population have emphasized outcomes in five distinct areas: post-secondary education, employment, residential and/or financial independence, romantic relationships, and parenthood (Furstenberg et al., Reference Furstenberg, Kennedy, McCloyd, Rumbaut and Settersten2003; Settersten & Ray, Reference Settersten and Ray2010; see Schulenberg, Bryant, et al., Reference Schulenberg, Bryant and O’Malley2004 for a somewhat different conceptualization of adult outcomes). Through this lens, finishing school and/or vocational training, obtaining full-time employment, leaving the family home, and finding a life partner are integral components of establishing oneself as an adult. Though many autistic young adults and their caregivers identify similar goals for adult success as their peers in the general population (Lord et al., Reference Lord, Charman, Havdahl, Carbone, Anagnostou, Boyd, Carr, Vries, Dissanayake, Divan, Freitag, Gotelli, Kasari, Knapp, Mundy, Plank, Scahill, Servili, Shattuck and McCauley2022; McCauley, Pickles, et al., Reference McCauley, Pickles, Huerta and Lord2020; Umagami et al., Reference Umagami, Remington, Lloyd-Evans, Davies and Crane2022), the social-communication differences associated with autism may make achievement of such goals uniquely challenging. Additionally, many young adults with autism and other developmental conditions experience an abrupt loss of educational and therapeutic services immediately after completing high school (often referred to as the “services cliff”; Shattuck et al., Reference Shattuck, Wagner, Narendorf, Sterzing and Hensley2011). This services cliff and the subsequent lack of adult services may exacerbate autistic youths’ challenges in obtaining positive adult outcomes (Anderson et al., Reference Anderson, Lupfer and Shattuck2018; Clarke, McCauley, et al., Reference Clarke, McCauley and Lord2021).
Further, given the heterogeneity of the autism spectrum, traditional markers of adult achievement may be irrelevant or inapplicable for some individuals with ASD. For example, for autistic young adults who have comorbid intellectual disability, are minimally/nonverbal, or both, graduating from college and having a full-time job may not be meaningful benchmarks of adult success. However, part-time employment in a supported setting or in the community with a job coach may be a useful benchmarks. In an effort to accurately reflect the heterogeneity of autism while attempting to replicate findings on the importance of social competence to adult outcomes in the general population, this study uses a modified version of the Vocational Index (VDI; Taylor & Seltzer, Reference Taylor and Seltzer2012), a rating scale specifically designed to assess employment and, for those capable, post-secondary education outcomes in adults with autism and other developmental conditions (Clarke, Sterrett, et al., Reference Clarke, Sterrett and Lord2021; Taylor, Center, et al., Reference Taylor, Center and Mailick2014).
Prior work examining normative outcomes in adults with ASD found relatively high IQ, low autism symptom severity, and few to no symptoms of psychopathology are positively associated with the likelihood of working, living independently, and having friends (Bal et al., Reference Bal, Kim, Fok and Lord2019; Clarke, Sterrett, et al., Reference Clarke, Sterrett and Lord2021; McCauley, Pickles, et al., Reference McCauley, Pickles, Huerta and Lord2020; Taylor, Center, et al., Reference Taylor, Center and Mailick2014). However, in relation to adult outcomes, there have been few attempts to measure more detailed aspects of social functioning that may not be key features of autism. The current project strives to quantify social competence in ASD and replicate findings from typical development that adolescent social competence predicts adult outcomes, specifically employment, independent living, and the presence of friendships and romantic relationships.
Studies of social competence in the general population have found positive associations between adolescent social competence and many adult outcomes, including employment (Collins & van Dulmen, Reference Collins, van Dulmen, Arnett and Tanner2006; Masten et al., Reference Masten, Desjardins, McCormick, Kuo and Long2010), friendship and romantic relationships (Romppanen et al. Reference Romppanen, Korhonen, Salmelin, Puura and Luoma2021; Schulenberg, Bryant, et al., Reference Schulenberg, Bryant and O’Malley2004), and good mental health (Kamis & Copeland, Reference Kamis and Copeland2020; Obradović & Hipwell, Reference Obradović and Hipwell2010). Some similar associations appear to exist for young adults with ASD. One study of a separate longitudinal sample of ASD indicated that high adolescent internalizing was associated with increased adult social isolation (Lounds Taylor et al., Reference Lounds Taylor, Adams and Bishop2017). Similarly, prior work in the sample considered in this paper indicated a trajectory of high depressive symptoms from mid-childhood through early adulthood was associated with greater autism symptom severity in mid-childhood and decreased likelihood of living independently, having friends, and being employed at age 26 (McCauley, Elias, et al., Reference McCauley, Elias and Lord2020).
In the general population, having a job is closely tied to success in many areas of adult life (Blustein, Reference Blustein2008); conversely, lack of employment is related to a variety of negative adult outcomes (Paul & Moser, Reference Paul and Moser2009). Similarly, recent work in our sample found that participation in independent work activities was associated with greater subjective well-being for adults with autism (Clarke, Sterrett, et al., Reference Clarke, Sterrett and Lord2021). However, despite a sizeable increase in the number autistic individuals attending post-secondary education (Elias & White, Reference Elias and White2018), adults with autism are employed at much a lower rate than their neurotypical peers (Burgess & Cimera, Reference Burgess and Cimera2014; Schall et al., Reference Schall, Wehman, Avellone and Taylor2020).
In addition, autistic individuals report high rates of loneliness. Prior evidence from this sample (McCauley, Pickles, et al., Reference McCauley, Pickles, Huerta and Lord2020) and others (Kuo et al., Reference Kuo, Orsmond, Cohn and Coster2013; Orsmond et al., Reference Orsmond, Shattuck, Cooper, Sterzing and Anderson2013) suggests many adults with autism have few or no social contacts outside of immediate family and care workers/staff. Adults with autism are also less likely to be in a committed romantic relationship than same-aged typically developing peers (Dewinter et al., Reference Dewinter, De Graaf and Begeer2017). The current project focuses on associations between social competence in adolescence (as measured by the Vineland, SSQ, and SDQ) and work, living status, friendship, and romantic outcomes in young adulthood in a longitudinal sample of individuals first referred for autism evaluations in early childhood, between ages 2 and 3 years.
Measuring social competence in ASD
In studies of typical development, there is consensus that social competence should be quantified via multiple measures and informants, both to capture as many aspects of the construct as possible (Burt et al., Reference Burt, Obradović, Long and Masten2008), and because peer and teacher or caregiver perceptions of social ability are meaningful components of social competence (Nowicki, Reference Nowicki2003). However, there is little consensus as to which measures are most effective in capturing social competence for various reporters and age groups (Arnold & Lindner-Müller, Reference Arnold and Lindner-Müller2013). Though the use of different measures completed by different reporters across different periods of development allows for a broad conceptualization of social competence, the consistent use of a measure over many years allows for meaningful comparison of scores across distinct developmental periods.
The Vineland Adaptive Behavior Scales (Sparrow et al., Reference Sparrow, Cicchetti and Balla2005) is the gold-standard measure of adaptive functioning, including social capabilities, in ASD and related developmental conditions. It is frequently used in clinical and research settings to assess an individual’s capability for independent functioning and to monitor progress over time. As a clinician administered, caregiver-report interview, the Vineland integrates multiple perspectives on an individual’s functioning. Vinelands were administered to participants in the present study at eight points from early childhood to adulthood: ages 2, 3, 5, 9, 14, 18, 21, and 26, allowing us to describe social competence in ASD across the life course. Additionally, we asked participants, caregivers, and teachers to complete two additional measures of social competence about the participants at approximately age 14, the Social Skills Questionnaire (SSQ) and the prosocial domain of the Strength and Difficulties Questionnaire (SDQ). Considered in tandem, these three measures provide a unique opportunity to examine concordance between differing social competence assessments and informants during adolescence.
Study aims
-
1. Characterize Vineland social age equivalence (AE) trajectories in our sample from ages 2 to 26.
Previous results in this sample from ages 2 to 9 years found social-AE scores followed a positive linear trajectory, with children with high verbal abilities and non-ASD developmental delays experiencing the steepest growth (Anderson et al., Reference Anderson, Oti, Lord and Welch2009). Given the increasingly sophisticated social norms of late childhood and adolescence, individuals with ASD may experience a slowing in Vineland Social-AE scores after age 9. We expected to replicate the trajectories described by Anderson and colleagues, and, in line with prior findings on Vineland daily living skills-AE trajectories (Clarke, McCauley, et al., Reference Clarke, McCauley and Lord2021; Smith et al., Reference Smith, Maenner and Seltzer2012), anticipated a plateau in social-AE trajectories in early adulthood.
-
2. Examine the convergence of our Vineland social-AE trajectories with two other measures of social competence from adolescence – the Social Skills Questionnaire (SSQ), and the prosocial domain of the Strengths and Difficulties Questionnaire (SDQ).
We predicted that, controlling for salient covariates (e.g. IQ, autism symptom severity), higher teacher-report SDQ prosocial scores and SSQ caregiver or self-report scores in early adolescence would be associated with higher social-AE scores across development, as well as a steeper rate of growth in social-AE trajectories.
-
3. Replicate findings from typical development (Burt et al., Reference Burt, Obradović, Long and Masten2008; Masten et al., Reference Masten, Desjardins, McCormick, Kuo and Long2010) that adolescent social competence predicts positive outcomes in adulthood for autistic individuals.
Controlling for salient covariates, we expected high Vineland social-AE, SSQ total, and SDQ prosocial scores collected in adolescence would predict normative friendship, romance, work, and living status outcomes in early adulthood.
Method
Participants
Two hundred and thirteen consecutive referrals under 37 months old at clinics in North Carolina and Chicago initially enrolled in a longitudinal study of ASD. One hundred and ninety-two participants were referred for autism and 21 participants were referred for nonspectrum developmental delays. Forty children of similar age and diagnostic characteristics from Michigan joined the study at age 9 and were subsequently seen at the same times, for a total of 253 participants. Of these 253 individuals, 55 participants in this cohort have never received an ASD diagnosis despite repeated blinded assessments as part of this project. These individuals were retained in the current analyses for two reasons. First, considerable evidence from this sample (Lord et al., Reference Lord, McCauley, Pepa, Huerta and Pickles2020) as well as other longitudinal (DaWalt et al., Reference DaWalt, Usher, Greenberg and Mailick2019; Hong et al., Reference Hong, Greenberg, Floyd, Pettee and Mailick Seltzer2003) and cross-sectional (Esbensen et al., Reference Esbensen, Bishop, Seltzer, Greenberg and Taylor2010) samples of autism and other developmental conditions suggest there are more similarities than differences in the lifespan experiences of these groups. Second, though autism is unique in its diagnostic emphasis on social communication deficits, many developmental conditions, including intellectual disability, language delay, and specific learning disorders and ADHD are associated with increased social challenges compared to the general population (Kushki et al., Reference Kushki, Anagnostou, Hammill, Duez, Brian, Iaboni, Schachar, Crosbie, Arnold and Lerch2019; Thapar et al., Reference Thapar, Cooper and Rutter2017; Thurm et al., Reference Thurm, Farmer, Salzman, Lord and Bishop2019). In-person assessments were completed at ages 2, 3, 5, 9, 18, 21, and 26. Additional parent interviews were completed at age 14. Prior work has described this sample in detail (Anderson et al., Reference Anderson, Liang and Lord2014; Lord et al., Reference Lord, Risi, DiLavore, Shulman, Thurm and Pickles2006; Pickles et al., Reference Pickles, McCauley, Pepa, Huerta and Lord2020). Descriptive characteristics of the total sample and the subsample analyzed for Aims 2 and 3 are displayed in Table 1.
Table 1. Total sample and Aims 2 and 3 subsample demographic characteristics
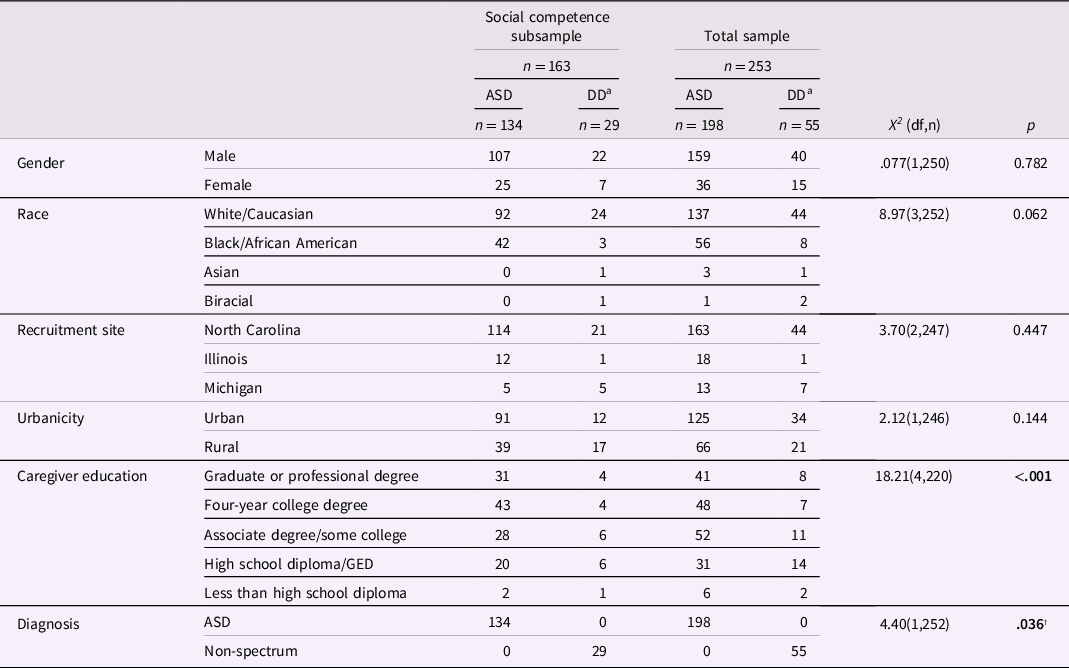
Bolded results indicate p ≤ .05.
a Nonspectrum developmental disabilities.
† Does not survive Bonferroni corrections.
Procedures
Questionnaires and direct testing, including the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., Reference Lord, Rutter, DiLavore, Risi, Gotham and Bishop2012), IQ tests chosen from a standard hierarchy (Anderson et al., Reference Anderson, Liang and Lord2014) and parent interviews conducted by a trained research assistant, specifically the Vineland Adaptive Behavior Scales, Second Edition (VABS-II; Sparrow et al., Reference Sparrow, Cicchetti and Balla2005), and the Social Emotional Functioning Interview (SEF-S & SEF-I; Rutter et al., Reference Rutter, LeCouteur, Lord, Macdonald, Rios and Folstein1988), were completed at participants’ homes. For the teacher-report SDQ, parents were asked to identify and provide contact information for the teacher or teacher’s aide who worked with their child most closely. Teachers were then contacted by study staff and mailed physical copies of assessments. Parents and participants over 18 who were their own legal guardians gave written consent as required by the relevant institutional review board(s) prior to all visits.
Measures
Social competence
Vineland adaptive behavior scales
The Vineland Adaptive Behavior Scales, First and Second Editions (VABS and VABS II; Sparrow et al., Reference Sparrow, Cicchetti and Balla2005) were used to assess adaptive social behavior during in-person visits and a phone interview at age 14. The VABS is a caregiver-interview assessment of adaptive behavior composed of three domains: communication, daily living skills, and socialization. Socialization is divided into three subdomains – play, interpersonal relationships, and coping skills – which each produce an age equivalence (AE) score approximating the chronological age of typical development that matches an individual’s abilities. Similarly, daily living skills (DLS) is divided into three subdomains – personal, domestic, and community – which each produce an age equivalent (AE) score. For this study, subdomain AEs were averaged into overall social age equivalence (Social-AE) and daily living skills equivalence (DLS-AE) scores.
Social skills questionnaire
The SSQ (Gresham & Elliott, Reference Gresham and Elliott1990) consists of 38 items in four skill areas: cooperation, assertion, responsibility, and self-control. Each item is rated by a caregiver on a scale from 0 to 2, with 0 indicating the item is Never true, 1 indicating it is Sometimes true, and 2 indicating the item is Always true. The SSQ was initially standardized using a sample of 4,000 typically developing students from preschool to Grade 12, with an equal number of boys and girls. The secondary-school version of the SSQ has acceptable internal consistency, with Cronbach’s alpha = .83 for the total scale (Gresham & Elliott, Reference Gresham and Elliott1990).
Strengths and difficulties questionnaire
The teacher-report SDQ (Goodman, Reference Goodman1997) prosocial subscale was used to measure prosocial in early adolescence. The teachers were asked to rate accuracy of five statements in relation to the student’s behavior using a scale from 0 to 2, where 0 indicated the statement was Not True, 1 indicated the statement was Somewhat True, and 2 indicate the statement was Certainly True. Statements comprising the SDQ prosocial subscale include, “considerate of other peoples’ feelings,” “helpful if someone is hurt, upset, or feeling ill,” and “kind to younger children.” Prior work assessing prosocial skills in ASD in a community-based sample found the SDQ prosocial subscale had acceptable internal consistency, with Cronbach’s alpha = 0.79 (McChesney & Toseeb, Reference McChesney and Toseeb2018).
IQ
The Mullen Scales of Early Learning (Mullen, Reference Mullen1995) were administered at age 2. Later cognitive assessments were chosen from a standard hierarchy including the Weschler Intelligence Scale for Children (WISC; Wechsler, Reference Wechsler2003), Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, Reference Wechsler2011), Differential Abilities Scale (DAS; Elliott, Reference Elliott2007), and Mullen (Anderson et al., Reference Anderson, Liang and Lord2014; Lord et al., Reference Lord, Risi, DiLavore, Shulman, Thurm and Pickles2006). Ratio IQs were calculated when raw scores fell outside deviation score ranges. Due to the wide range of our participants’ verbal abilities, nonverbal IQ was used as a covariate rather than verbal or full-scale IQ. To approximate participant IQ in early adolescence (i.e., when the social competence measures were collected), nonverbal IQ at age 9, the closest available timepoint, was used in all current analyses.
Adult outcomes
Vocational index
Data from caregiver-report demographic forms were used to determine participants’ vocational activities in early adulthood (m = 20.01, SD = 2.07). Vocational data were coded using a measure of independence in employment and post-secondary education activities in adults with ASD and other developmental conditions developed by Taylor and Seltzer (Reference Taylor and Seltzer2012), the Vocational Index (VDI). The VDI has been used previously to measure change in vocational trajectories both in the current sample (Clarke, Sterrett, et al., Reference Clarke, Sterrett and Lord2021) and in a separate longitudinal sample of adults with ASD (Taylor and Mailick, Reference Taylor and Mailick2014; Taylor, Smith, et al., Reference Taylor, Smith and Mailick2014). The VDI includes scores specifically for individuals pursuing post-secondary education to improve their employment prospects, as well as scores for individuals in volunteer, sheltered workshop and supported employment settings. These characteristics make the VDI a uniquely effective measure for understanding employment and post-secondary education outcomes in ASD amongst individuals of varying language and IQ levels. For the current analyses, a modified version of the VDI was used, with scores ranging from 1 to 10 (Clarke, Sterrett, et al., Reference Clarke, Sterrett and Lord2021). A VDI score of 1 indicates no participation in vocational activities, and a score of 10 indicates participation in competitive employment for 20 hr/week or more without supports.
Residential status
Data from caregiver-report demographic forms were used to determine participants’ residential status when participants were approximately age 25. This information was collapsed into a binary variable, with 1 indicating the participant currently lived independently outside of the family home (this included living with roommates or romantic partners) and 0 indicating the participant currently lived in the family home or in a supported residential setting (e.g., group home, or a facility with designated residential support staff).
Friendships
The presence of friendships in adulthood was assessed via raw scores on item 65, Friendships, of the Autism Diagnostic Interview, Revised (ADI-R; Le Couteur et al., Reference Le Couteur, Lord and Rutter2003) a clinician-administered caregiver interview. The ADI-R was administered when participants were approximately age 19 (m = 18.93, SD = 1.33). For the current analyses, a binary score on this item was generated, with 1 indicating one or more mutual, reciprocal friendships and 0 indicating no mutual, reciprocal friendships.
Romantic relationships
The Social Emotional Functioning Interview (SEF-S & SEF-I; Rutter et al., 1988) was used to determine whether participants had ever been involved in a romantic relationship. Caregivers and participants were completed during in-person interviews at approximate age 25 (m = 24.97, SD = 3.23). The interview consists of a series of open-ended questions about social and romantic relationships, living status, and interests that has been previously employed in samples of autistic adults (Howlin, Reference Howlin2000). For the current analyses, a binary score for the love relationships item of the SEF was created, with 1 indicating the individual was currently or had previously been involved in a mutual romantic relationship and 0 indicating the individual had never been involved in a mutual romantic relationship.
Autism symptomology
Autism Diagnostic Observation Schedule (ADOS; Lord et al., Reference Lord, Rutter, DiLavore, Risi, Gotham and Bishop2012) clinical symptom severity (CSS) scores were used to measure autism symptomology. The ADOS is a semi-structured, clinician-administered observational measure and is widely considered the “gold standard” for autism diagnosis. To approximate participant autism symptom severity in early adolescence (i.e., when the social competence measures were collected), CSS scores at age 9, the closest available timepoint, were used as a covariate in all current analyses.
Clinicians made best-estimate diagnoses of ASD, other developmental disabilities, or typical development at each in-person visit, except age 3. Despite multiple assessments, 55 individuals in this sample have never received an ASD diagnosis. These individuals did not differ from participants with ASD in nonverbal IQ at age two (t(1, 185) = .249, p = .63), nonverbal IQ at age nine (t(1, 190) = .09, p = .51), VDI scores (t(1, 148) = 2.18, p = .07), or likelihood of ever working full time in adulthood (X 2 (1, 161) = .68, p = .40). Given considerable overlap in the challenges faced during young adulthood for all individuals with developmental disabilities (Lord et al., Reference Lord, McCauley, Pepa, Huerta and Pickles2020), participants with nonspectrum delays were retained in the current analyses.
Data analysis
Descriptive analyses and significance testing
For Aim 1, chi-square analyses were used to compare the composition of Vineland Social-AE trajectory groups by diagnostic status (Ever or Never ASD), gender, race, and caregiver education (Table 2). Independent t-tests were used to compare Social-AE trajectory groups by ADOS CSS scores, IQ scores, and VDI scores (Table 3). For all three aims, given the considerable number of analyses, Bonferroni corrections to adjust for multiple tests are reported throughout.
Table 2. Demographic characteristics by social-AE trajectory groups
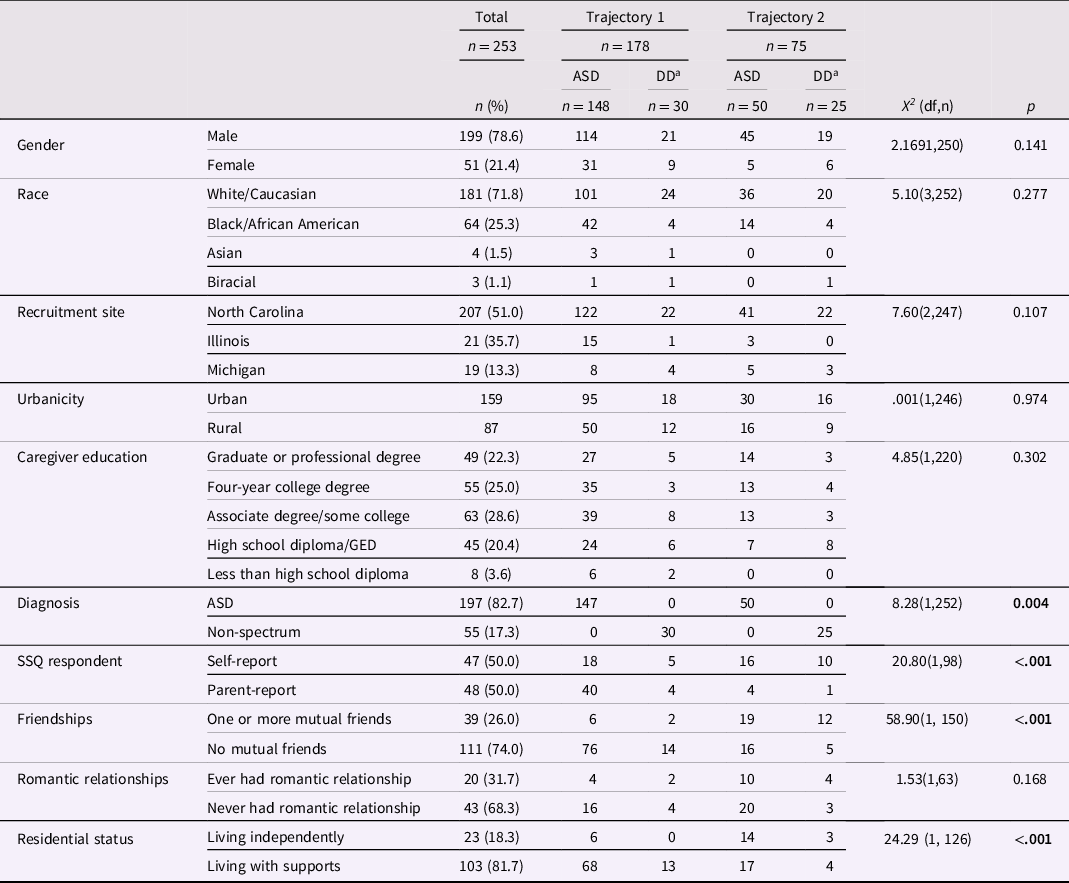
Bolded results indicate p ≤ .05.
a Nonspectrum developmental disabilities.
Table 3. IQ, autism severity, social competence, and vocational measures scores by social-AE trajectory groups
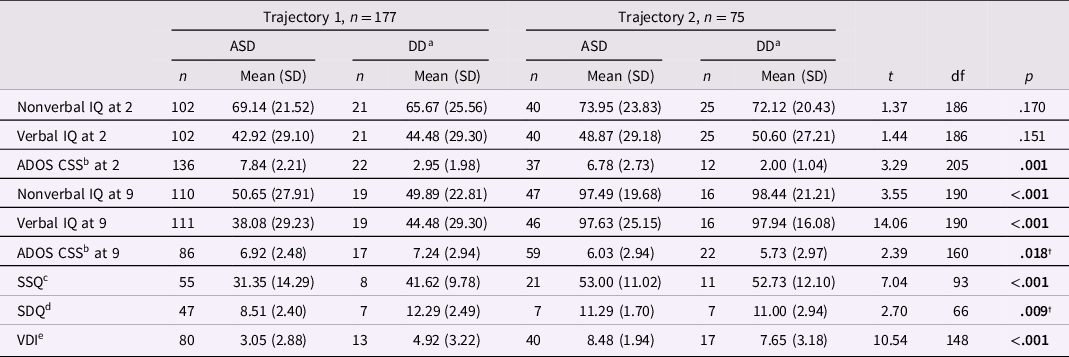
Bolded results indicate p ≤ .05.
a Nonspectrum developmental disabilities.
b Calibrated severity score.
c Social skills questionnaire
d Strengths and difficulties questionnaire – prosocial subscale.
e Vocational index
† Does not survive Bonferroni corrections.
Missing data and attrition
For Aim 1, analyses included 1,206 assessments from all 253 individuals in the longitudinal cohort. On average, participants’ caregivers completed the Vineland 4.8 times from ages 2 to 26, with a range of 1–9 Vineland assessments. For Aims 2 and 3, analyses were completed using participants with available scores on at least one social competence measure (the Vineland, SSQ, or SDQ) at age 14 (n = 163). Participants in the social competence subsample were more likely to have a caregiver with a college degree X 2 (4, 220) = 18.21, p = .001 than excluded participants (Table 1). Thus, caregiver education was tested as a covariate in all Aim 2 and Aim analyses. Participants with social competence data were also more likely to have been diagnosed with ASD X 2 (1, 246) = 2.12, p = .03. This diagnostic status difference did not survive Bonferroni corrections (Table 1), however, out of caution, we still tested participant diagnostic status as a covariate in all Aim 2 and Aim 3 analyses.
Attrition in this longitudinal cohort has been associated with both lower caregiver education and African American race. Importantly, attrition in this sample is not associated with gender or behavioral characteristics such as autism severity or IQ (Pickles et al., Reference Pickles, McCauley, Pepa, Huerta and Lord2020). Participants in the Aims 2 and 3 subsample did not significantly differ from participants without social competence data by gender X 2 (1, 250) = .07, p = .78, race X 2 (1, 252) = 8.97, p = .06, recruitment site X 2 (1, 247) = 3.70, p = .44, or urbanicity X 2 (1, 246) = 2.12, p = .14. See Table 5 for the sample size of each continuous predictor included in analyses for Aims 2 and 3.
Aim 1: Characterize Vineland social-AE trajectories from 2 to 26
To examine social AE trajectories and extend prior findings in this sample (Anderson et al., Reference Anderson, Oti, Lord and Welch2009), the traj plugin in Stata 16 was used to perform group-based trajectory modeling. This approach estimates developmental trajectories via maximum likelihood estimation using a general quasi-Newton procedure; missing data are handled by estimating the model using all available information. Eight timepoints of Vineland assessments were used as independent variables to analyze latent grouping of individuals in Social-AE trajectories. Unconditional 1, 2, and 3 class models were compared using Bayesian Information Criterion (BIC) and the smallest group membership percentage (Figure 1). After classes were determined, higher order effects were tested to establish whether cubic, quadratic, linear, or intercept modeling best explained variation over time.
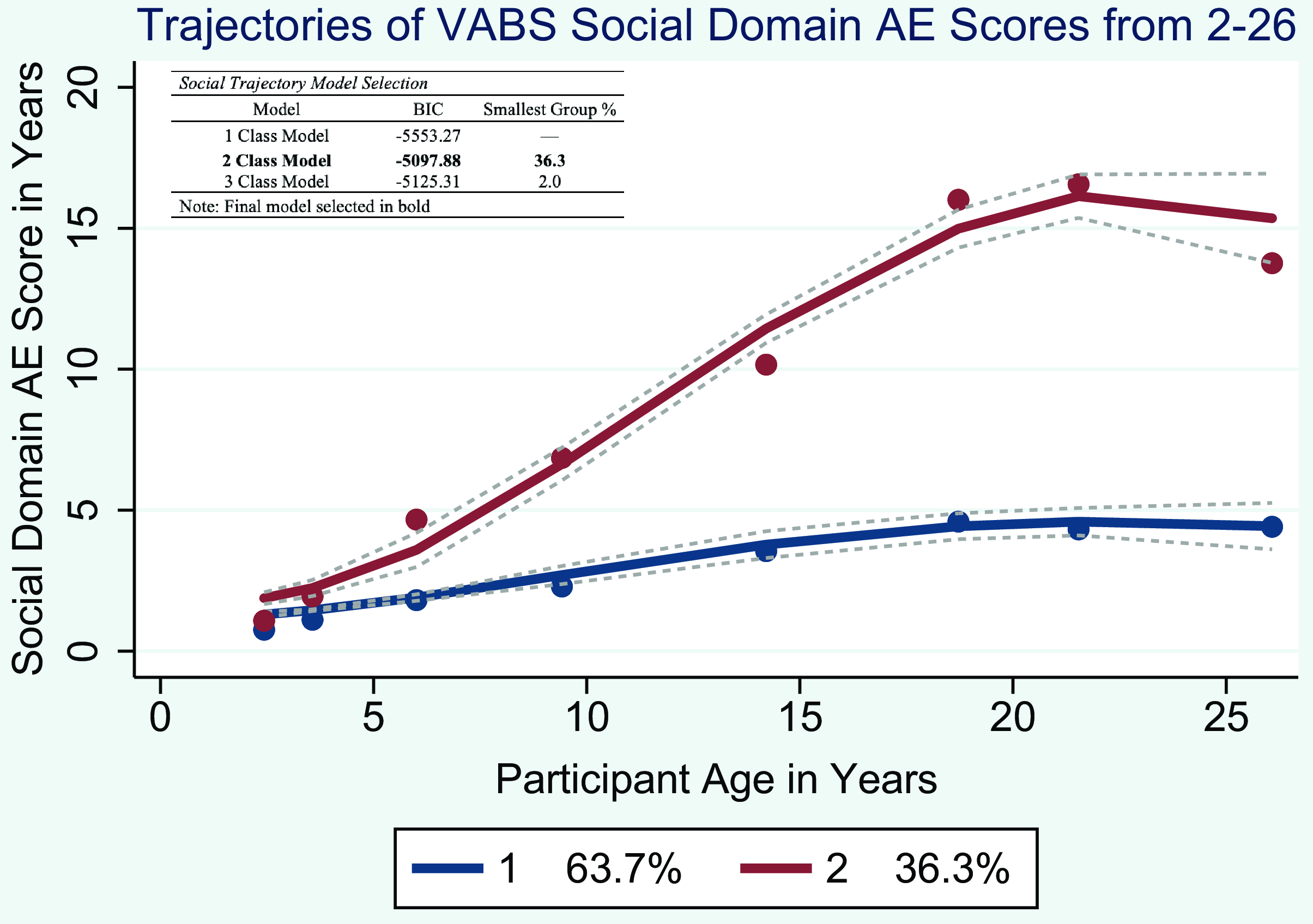
Figure 1. Trajectories of Vineland social domain age equivalence scores from 2 to 26.
Aim 2: Examine convergence between social-AE trajectories and SSQ and SDQ prosocial scores from adolescence
The mixed procedure in Stata 16 was used to investigate rates of change in Vineland social AE scores from ages 2 to 26, as well as associations between social AE trajectories and teacher-report SDQ prosocial and caregiver- and self-report SSQ scores from age 14. A multilevel modeling approach was selected because participants were nested across time points, thus multilevel modeling allowed us to account for the nonindependence of assessment observations. This approach also enabled us to evaluate the influence of the inclusion of a random slope on trajectory estimates and allowed for the differential examination of associations between the adolescent social competence measures and both the intercepts and slopes of Vineland social-AE trajectories.
There were three models of interest. The first and simplest model included fixed effects for trajectory group and an age × trajectory group interaction term, as well as a random subject level slope. To analyze the effects of salient demographic covariates on Social-AE trajectories, the second model also included fixed effects for caregiver education and participant diagnostic status (ever or never diagnosed with ASD), nonverbal IQ at age 9, ADOS CSS score at age 9, Vineland DLS AE scores at age 14, as well as covariate × age, covariate × trajectory group, and covariate × age × trajectory group interaction terms. Nonsignificant covariate main effects were identified and omitted before testing interaction terms, and nonsignificant interaction terms were removed from the final model. The third and most complex model also included fixed effects for SSQ score, SSQ respondent (parent- or participant-report), and SDQ prosocial score, as well as social competence measure × age, social competence measure × trajectory group, and social competence measure × age × trajectory group interaction terms. Again, nonsignificant covariates and interaction terms were identified and removed from the final model.
Aim 3: Examine the utility of Vineland social-AE, SSQ, and SDQ prosocial scores from adolescence in predicting adult outcomes
Multiple hierarchical regression and binary logistic regression were used to examine whether Vineland social-AE, SSQ, and SDQ prosocial scores in adolescence predicted VDI scores and the presence of friendships at age 19, and the likelihood of living independently or having ever had a romantic relationship by age 26. First, separate regressions for demographic variables associated with attrition (participant diagnostic status, caregiver education) and inclusion in the High Social-AE trajectory group (nonverbal IQ at 9, ADOS CSS score at 9) were run for each of the four outcomes of interest: VDI scores, residential status, ADI-R friendship item scores, and SEF-I romance item scores. Demographic variables identified as significant predictors were then included as covariates in all social competence regression models.
Results
Aim 1: Characterize Vineland social-AE trajectories from 2 to 26
A two-group model (Figure 1) was determined the best fit, based on the percentage of variance explained. The first trajectory group, Low Social-AE, comprised 63.7% of the sample. The second group, High Social-AE, comprised 36.3% of the sample. The Low Social-AE group followed a quadratic slope, and the High Social-AE group followed a cubic slope. Social-AE scores of both trajectory groups were similar in early childhood but diverged by age 5 and continued to diverge with age. The Low Social-AE trajectory was characterized by slow linear gains from early childhood through young adulthood, with a plateau in scores from ages 21 to 26 years. In contrast, the High Social-AE trajectory was characterized by steeper linear gains in Social-AE scores from early childhood through young adulthood, followed by a period of slower growth from ages 19 to 21 and a period of decline from ages 21 to 26.
T-tests and chi-squares indicated trajectory groups did not differ by race, gender, urbanicity, caregiver education, recruitment site, diagnostic status, nonverbal or verbal IQ at age 2, ADOS CSS scores at age 9, or SDQ prosocial scores. Participants in the High social-AE trajectory group were more likely to have completed the self-report version of the SSQ in adolescence (p < .001), had higher SSQ total scores (p < .001), lower ADOS CSS scores at age 2 (p = .001), and higher nonverbal and verbal IQ at age 9 (both p < .001). Participants in the High social-AE trajectory group were also more likely to have at least one mutual friendship at age 19 and were engaged in more independent vocational activities than participants in the Low social-AE trajectory group (both p < .001). However, participants in the two trajectory groups did not differ in their likelihood of ever having a romantic relationship in adulthood (p = .168). Descriptive characteristics of the Low and High trajectory groups are reported in Tables 2 and 3.
Aim 2: Examine convergence between social-AE trajectories and SSQ and SDQ prosocial scores from adolescence
Multilevel modeling was used to characterize the rate of change in social-AE trajectories, identify effects of demographic characteristics on trajectory change, and examine the convergence of SSQ and SDQ prosocial domain scores from early adolescence with participants’ social-AE trajectories. The first and simplest model included fixed effects for trajectory group, an age × trajectory group interaction term, and a subject-level random slope. There was a significant main effect of trajectory group (p < .001) and a significant age × trajectory group interaction (p < .001). The inclusion of the subject-level random slope also significantly contributed to the model (p < .05; Table 4) indicating individual participants’ Vineland Social-AE trajectories significantly differed from one another. The main effect of trajectory group, the trajectory group × age interaction term, and the subject-level random slope remained significant in the covariate and social competence models reported below (Table 4).
Table 4. Effects of demographic covariates and social competence measures on rates of change in social-AE trajectories
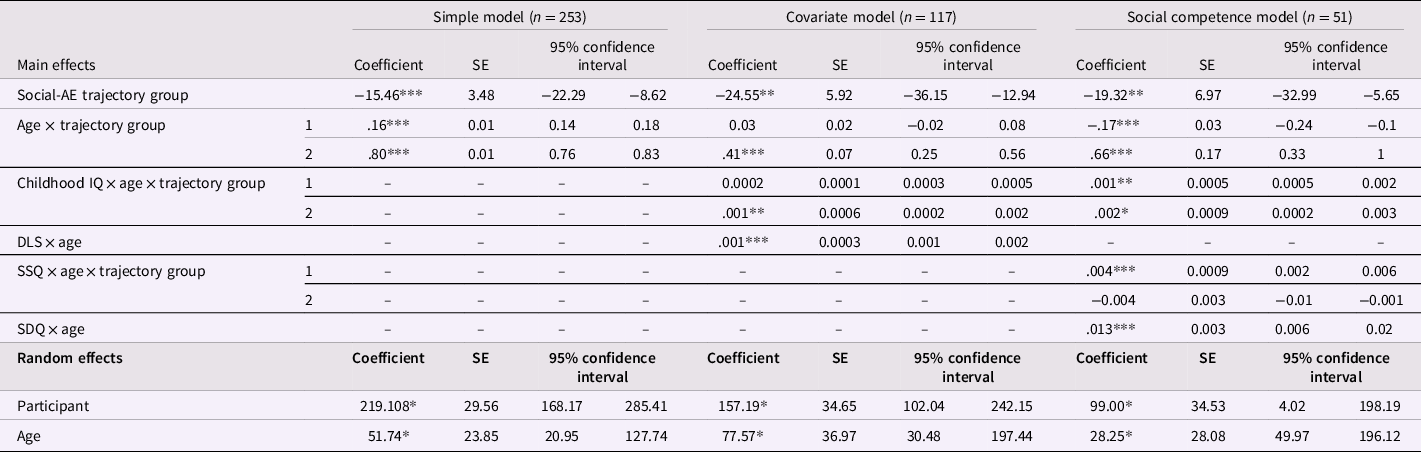
For brevity, only covariates and social competence measures with significant main effects and/or interaction terms are included in the table. All nonsignificant covariate main effects and interaction terms were dropped from the final models. The first and simplest model included fixed effects for trajectory group, and an age × trajectory group interaction term, as well as a random subject level slope. The second covariate model also included fixed effects for caregiver education, diagnostic status, nonverbal IQ at age 9, ADOS CSS score at age 9, and Vineland DLS AE scores at age 14, as well as interaction terms. The third and most complex model also included fixed effects for SSQ score, SSQ respondent (parent- or participant-report), and SDQ prosocial score, as well as interaction terms. For all three models, nonsignificant main effects were identified and omitted before testing interaction terms, and nonsignificant interaction terms were removed from the final models.
*p < .05, **p < .01, ***p ≤ .001.
Covariates model
The second model tested fixed effects for salient covariates, specifically nonverbal IQ at 9, ADOS CSS at 9, Vineland DLS-AE at 14, recruitment site, diagnostic status, gender, and caregiver education. First, nonsignificant covariate fixed effects were identified and removed. Next, interaction terms were tested for significant covariates only. Only significant covariate fixed effects and interaction terms were retained in the final covariate model.
The fixed effects for recruitment site, diagnostic status, gender, and caregiver education, were nonsignificant (all p > .05) and thus dropped from the covariate model. The fixed effects for nonverbal IQ at 9 and Vineland DLS-AE score at 14 were significant, thus interaction terms were tested. There was a significant nonverbal IQ at 9 × age × trajectory group interaction (p = .019) indicating participants within the High Social-AE trajectory group with relatively high nonverbal IQ at age 9 experienced significantly faster growth in their Vineland Social-AE scores than participants with relatively low nonverbal IQ at age 9 in the High Social-AE trajectory group. In contrast, nonverbal IQ at age 9 was not associated with growth in Social-AE scores for participants within the Low Social-AE trajectory group. There was also a significant Vineland DLS-AE score at 14 × age interaction (p < .001; Table 4). For participants in both trajectory groups, having relatively high daily living skills, as measured by Vineland DLS-AE scores in adolescence, was associated with faster growth in Social-AE scores across development.
Social competence measures model
In addition to the significant fixed effects, interaction terms, and subject-level random slope identified in the simple model and the covariates model, the third and final model tested effects for SSQ scores, SSQ respondent, and SDQ prosocial scores. As in the covariate model, nonsignificant fixed effects for social competence measures were identified and removed prior to testing interaction terms.
As in the covariate model, there was also a significant nonverbal IQ at 9 × age × trajectory group (p = .003) interaction. However, after including social competence measures in the model, the DLS-AE score at 14 × age interaction term identified in the covariates model was no longer significant and subsequently dropped. After accounting for variance explained by parent- and self-report SSQ and teacher-report SDQ prosocial scores, daily living skills at age 14 were no longer a significant predictor of growth in Vineland Social-AE trajectories.
There was no significant effect of SSQ respondent (p > .05), and this variable was dropped from the final social competence model. There were significant fixed effects for SDQ prosocial and SSQ scores thus, interaction terms for these measures were also tested. There was a significant SDQ prosocial score × age (p < .001) interaction, indicating participants in both trajectory groups with high teacher-rated prosocial scores on the SDQ in early adolescence had faster growth in Social-AE scores. There was also a significant SSQ score × age × trajectory group (p < .001) interaction, signifying those participants in the High Social-AE trajectory group with high SSQ scores experienced faster growth in Vineland Social-AE scores than participants in the High Social-AE trajectory group with low SSQ scores. In contrast, rates of growth did not significantly differ by SSQ scores in the Low Social-AE trajectory group.
In sum, not surprisingly, Vineland Social-AE scores increased with age. On average, participants in the high trajectory group had higher scores and experienced a faster rate of growth in Social-AE scores over time compared to participants in the low trajectory group. Individuals in the High Social-AE group with relatively high nonverbal IQs at age 9 experienced significantly faster growth in their Vineland Social-AE scores than participants in the High Social-AE group with relatively low nonverbal IQs at age 9. Similarly, those participants in the High Social-AE group with high SSQ scores experienced faster growth in Vineland Social-AE scores than participants in the High Social-AE group with low SSQ scores. In contrast, rates of growth amongst participants in the Low Social-AE trajectory group did not significantly differ by SSQ scores or nonverbal IQ at age 9. Participants in both trajectory groups with high teacher-rated prosocial scores on the SDQ at age 14 had faster growth in Social-AE scores.
Aim 3: Examine the utility of Vineland social-AE, SSQ, and SDQ prosocial scores from adolescence in predicting adult outcomes
Multiple hierarchical regressions and logistic regressions were performed to assess the ability of Vineland Social-AE, SSQ, and SDQ prosocial scores from age 14 to predict adult vocational, residential, and social outcomes. To account for the fact that (1) participants not included in these analyses due to missing data were significantly more likely to have caregivers with less than a college degree (p = .001) and to not have an ASD diagnosis (though this difference did not survive Bonferroni corrections, p = .03) and (2) participants in the High Social-AE trajectory had significantly lower ADOS CSS and higher nonverbal IQ scores at 9 than participants in the Low social-AE trajectory, separate regressions for caregiver education, diagnostic status, ADOS CSS, and IQ were run for each of the outcomes of interest: VDI scores, residential status, ADI-R friendship item scores, and SEF-I love relationship item scores. After Bonferroni corrections, ASD diagnostic status was a significant predictor of ADI-R friendship scores (p = .01), but not VDI scores (p = .03), residential status or SEF-I romance scores (both p > .05). After Bonferroni corrections, nonverbal IQ was a significant predictor of VDI scores, residential status and SEF-I romance scores (all p < .001) but not ADI-R friendship scores (p > .05). Maternal education and ADOS CSS at 9 did not significantly predict VDI, residential status, ADI-R friendship, nor SEF-I romance scores (all p > .05). Thus, diagnostic status was included as a covariate in all friendship models and nonverbal IQ at 9 was included in all VDI score, residential status, and romance models.
Adult work and residential status outcomes
Multiple hierarchical regressions were conducted to examine the utility of Vineland Social-AE, SSQ, and SDQ scores from adolescence to predict participants’ VDI scores in early adulthood. Nonverbal IQ at age 9 was entered in the first block of all vocational regression models. The social competence measure of interest (Vineland Social-AE, SSQ, SDQ) was entered in the second block of each hierarchical regression model.
Vineland Social-AE scores at age 14 were a significant predictor of VDI scores in early adulthood (p = .010). Nonverbal IQ at age 9 (p = .011) was also a significant predictor of VDI scores in the Vineland Social-AE vocational regression model. Having relatively high social competence in early adolescence as measured by the Vineland and childhood nonverbal IQ were both associated with an increased the likelihood of adult employment.
Despite being associated with faster growth in Vineland Social-AE trajectories, teacher SDQ prosocial scores were not a significant predictor of VDI scores in early adulthood (p = .130). Nonverbal IQ at age 9 was the only significant predictor (p = .004) of VDI scores in early adulthood in the SDQ model. Similarly, though parent- and self-report SSQ total scores were associated with faster growth in Vineland Social-AE trajectories, only SSQ respondent (parent- or self-report; p < .001) significantly predicted VDI scores in early adulthood. In contrast, SSQ total score (p = .563) and nonverbal IQ (p = .241) did not significantly contribute to the SSQ model. Completing the SSQ without assistance from a caregiver in adolescence was a better predictor of positive adult work outcomes than SSQ total score. Controlling for nonverbal IQ, participants who completed the SSQ themselves reported higher scores than participants whose caregiver completed the SSQ.
Binary logistic regressions were conducted to examine the predictive validity of adolescent Vineland Social-AE, SSQ, and SDQ scores on the likelihood of living independently by age 26. To control for salient covariates, nonverbal IQ at age 9 was included in the covariate block of all residential status models. The social competence measures of interest (Vineland Social-AE, SSQ, SDQ) were entered in the second block of each binary logistic regression model.
Vineland Social-AE scores at age 14 were a significant predictor of residential status at age 25 (p = .016). Nonverbal IQ at age 9 (p = .012) was also a significant predictor of residential status. Having relatively high social competence in early adolescence as measured by the Vineland and relatively high childhood nonverbal IQ were both associated with an increased likelihood of living independently at age 26.
Similar to employment outcomes, teacher SDQ prosocial scores were not a significant predictor of residential status (p = .332). In the SDQ prosocial residential status model, nonverbal IQ at age 9 was the only significant predictor of residential status at age 25 (p < .001). Likewise, nonverbal IQ at age 9 (p = .004) was the only significant predictor in the SSQ residential status model. Neither SSQ total score (p = .578) nor SSQ respondent (p = .349) significantly contributed to the SSQ model. After controlling for IQ, having relatively high social competence in early adolescence as measured by the SSQ and the SDQ prosocial domain was not predictive of residential status at age 25.
Adult friendship and romance outcomes
Binary logistic regressions were conducted to examine the predictive validity of adolescent Vineland Social-AE, SSQ, and SDQ scores on (1) the likelihood of having at least one friendship in early adulthood and (2) the likelihood of having ever been in a romantic relationship. To control for salient covariates, diagnostic status was included in the covariate block of all friendship models, and nonverbal IQ at 9 was included in the covariate block of all romance models. Diagnostic status did not significantly contribute to the SDQ and Vineland Social-AE friendship regression models (both p > .05).
Vineland Social-AE scores at age 14 were a significant predictor of having at least one friendship in adulthood (p = .004; Table 5). Participants with significantly higher Vineland Social-AE scores in adolescence were more likely to have at least one friendship in early adulthood, regardless of diagnostic status. After Bonferroni corrections, SDQ prosocial scores from adolescence were not a significant predictor of having at least one friendship in adulthood (p = .030). SSQ scores from adolescence were a significant predictor of having at least one friendship in adulthood (p = .010). Diagnostic status was also a significant predictor in the SSQ model (p = .007) though SSQ respondent (p = .647) was not. Participants with relatively high SSQ total scores and participants that had never received an ASD diagnosis were significantly more likely than their peers to have at least one friendship in early adulthood.
Table 5. Correlations between continuous social competence and behavioral phenotype variables
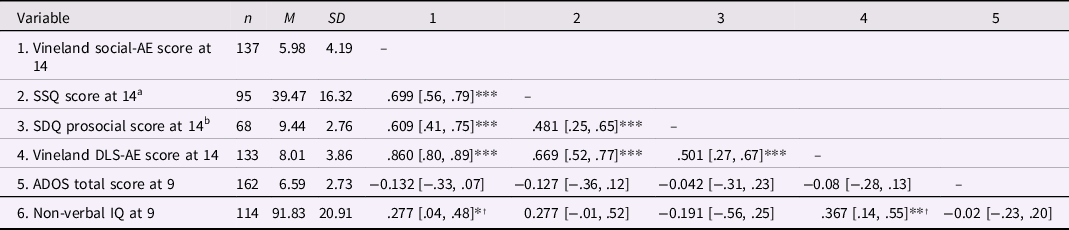
Values in square brackets indicate the 95% confidence interval for each correlation.
a SSQ data was either caregiver or self-report. At age 14, 48 participants had caregiver report SSQ data, and 47 had self-report data.
b SDQ data was teacher-report.
† Does not survive Bonferroni corrections.
*p < .05, **p < .01, ***p ≤ .001.
In contrast to the results with friendship, adolescent Vineland Social-AE scores (p = .823), SSQ total scores (p = .624), and SDQ prosocial scores (p = .322) did not significantly predict the likelihood of having ever been in a romantic relationship by age 25 (Table 5). However, nonverbal IQ at age 9 significantly contributed to the Vineland (p = .009) model, indicating childhood IQ was a better predictor of having had at least one romantic relationship by age 25 than Vineland Social-AE score at age 14. After Bonferroni corrections, nonverbal IQ at age 9 did not significantly contribute to the SSQ (p = .036), and SDQ (p = .030) romance regression models,
Discussion
This study investigated social competence in ASD and other developmental conditions and examined how clinician-, teacher-, caregiver-, and self-reports of social competence from adolescence related to work, friendship, and romantic outcomes in early adulthood. We identified two trajectories of growth in our primary social competence measure – clinician-rated Vineland Social-AE scores – from ages 2 to 26, a High Social-AE group and a Low Social-AE group. Both groups experienced positive linear growth in Social-AE scores from ages 2 to 19, though the High Social-AE group had a faster rate of growth. Both groups experienced a plateau or decline in Vineland Social-AE scores in early adulthood, between ages 21 and 26. This slowing or loss of adaptive social behaviors in young adulthood is consistent with prior findings in this sample (Clarke, McCauley, et al., Reference Clarke, McCauley and Lord2021) and in other longitudinal samples of autism (Smith et al., Reference Smith, Maenner and Seltzer2012) that many autistic individuals may stop making gains in adaptive behavior in the early years of adulthood. This stagnation in adaptive behavior growth appears to be tied to the transition out of the school system, which is often associated with considerable service loss for this population (Laxman et al., Reference Laxman, Taylor, DaWalt, Greenberg and Mailick2019; Shattuck et al., Reference Shattuck, Wagner, Narendorf, Sterzing and Hensley2011).
Multilevel modeling indicated convergence between clinician-rated Vineland scores, teacher-report SDQ prosocial scores, and caregiver- and self-report SSQ scores. Specifically, amongst participants in the High Social-AE trajectory group, caregiver-report and self-report SSQ scores from adolescence and nonverbal IQ at age 9 were associated with faster growth in Vineland Social-AE scores. In contrast, teacher-report SDQ prosocial scores from adolescence were associated with faster growth in Vineland Social-AE scores in all participants, regardless of trajectory group. After accounting for the variance explained by the SSQ and SDQ, nonverbal IQ at age 9 was the only participant characteristic that significantly contributed to growth in Vineland Social-AE scores across development. There were no significant effects of race, maternal education, autism symptom severity, daily living skills, gender, or recruitment site on growth in Vineland Social-AE trajectories.
Finally, regression models indicated Vineland Social-AE scores at age 14 were a significant predictor of participating in vocational activities, living independently, and of having at least one mutual and reciprocal friendship in early adulthood. SSQ scores from adolescence were also significant predictors of having at least one friendship in early adulthood but did not predict work or residential status outcomes. Teacher-report SDQ prosocial scores at age 14 did not predict any of the adult outcomes examined here. Nonverbal IQ at age 9 was the only significant predictor of having ever had a romantic relationship in this sample. Having relatively high nonverbal IQ at age 9 was also associated with an increased likelihood of employment and living independently.
We had data on romantic relationships for relatively few participants in our sample (n = 63). It is possible that we did not have sufficient power to detect whether any of our social competence measures could predict the likelihood of having ever been in a romantic relationship. Notably, by age 25, only 31% of those 63 participants had ever been in a romantic relationship. This reflects the continued struggle to form lasting and meaningful relationships that many adults with ASD experience. It is also indicative of the broad heterogeneity represented by this longitudinal cohort; for our more impacted participants, many of whom have high daily care needs and/or limited language, a romantic relationship may not be a realistic or meaningful positive outcome in adulthood. Though the present study focused on achievement of normative adult outcomes, additional work is needed to conceptualize positive and attainable adult outcomes for individuals with ASD with high support needs (McCauley, Pickles, et al., Reference McCauley, Pickles, Huerta and Lord2020).
In addition to the limited number of participants who had ever been in a romantic relationship, there were relatively few participants living independently at age 25. Of the subsample of participants with residential status data (n = 126), only 18.3% of those 126 participants were living independently at age 25. Anecdotally, only a handful of the participants in this sample who were living in their family home or in another supported residential setting at age 25 in this sample have ever lived independently. This is in contrast to young adults in the general population who may move back into their family home at intervals after periods of independence (Swartz, Reference Swartz2009).
Diagnostic status did not significantly contribute to growth in Vineland Social-AE trajectories; however, it was a significant predictor of having at least one friendship in early adulthood. Given the unique social challenges of ASD, it is not surprising that having a non-ASD developmental delay would be associated with more social connections in early adulthood. However, regardless of diagnostic category, adults with neurodevelopmental disorders encounter considerable difficulty, including social difficulties across the life course (Lord et al., Reference Lord, McCauley, Pepa, Huerta and Pickles2020). These adults also experience the services cliff, also have difficulty attaining normative adult outcomes, and also are likely to have limited and/or negative social experiences with peers in the general population in adolescence. This is reflected in our findings that having a non-ASD developmental delay was not predictive of adult work, residential status, or romantic outcomes. It is important to acknowledge that autism and other developmental conditions share important similarities to one another, frequently cooccur, and may impact young adult life in similar ways (Thapar et al., Reference Thapar, Cooper and Rutter2017).
Even after controlling for IQ, caregiver- and self-report total SSQ scores and teacher-report SDQ prosocial scores in adolescence explained a significant portion of variation in Vineland Social-AE trajectories across development. Though SSQ and SDQ prosocial subscale scores in adolescence were associated with faster growth in Vineland Social-AE scores across development, as well as an increased likelihood of having at least one reciprocal friendship in early adulthood, these measures were not significant predictors of work or residential status outcomes, and only the SSQ also predicted friendship outcomes. Nevertheless, given that Vineland Social-AE scores at age 14 predicted vocational activities in early adulthood, and that SSQ and SDQ prosocial scores were associated with growth in Vineland Social-AE scores, these two measures may be indirectly related to adult work outcomes. Unfortunately, our sample size did not allow us to test for possible mediation effects.
SSQ respondent – in other words, whether the participant completed the SSQ by themselves in adolescence or with assistance from a caregiver – predicted adult work outcomes. This also suggests that participants’ capacity to complete basic daily tasks (like filling out a questionnaire) independently in adolescence was more important to adult work outcomes then competence in social skills as assessed by the SSQ. In a similar vein, relatively high daily living skills at 14 were associated with faster growth in Vineland Social-AE scores from ages 2 to 26 in our covariate multilevel model (Table 4). However, after accounting for variance explained by SSQ and SDQ scores, the effect of daily living skills at 14 on Vineland Social-AE trajectories was no longer significant and was subsequently dropped from the final multilevel model. Though descriptive analyses indicated SSQ respondent and daily living skills were significantly positively correlated in this sample (Table 5), these variables are not colinear. Considered as a whole, these findings underscore that no single personal characteristic can predict success across the life course.
Our ability to examine information on social competence in adolescence from a variety of raters (clinician, caregiver or self, and teacher) as well as measures is a strength of the current study. Notably, teacher-report SDQ prosocial scores did not predict any of the adult outomes examined here, and caregiver and self-report SSQ scores predicted friendship outcomes only. In contrast, Vineland Social-AE scores predicted work, residential status, and friendship outcomes. For teacher ratings, experiences of the school context can be quite different for children with autism compared to their peers in the general population, particularly for autistic individuals who spend all or part of the school day in nonintegrated classroom settings. School experiences are no doubt critical to the later life success of children with ASD, but it remains unclear what the most critical elements of classroom experiences in predicting later life success are for autistic individuals. For example, placement in mainstream classrooms is associated with better outcomes of children with autism, but classroom placement is often confounded with IQ and language ability (Hess et al., Reference Hess, Morrier, Heflin and Ivey2008; Karanth & Chandhok, Reference Karanth and Chandhok2013). Our sample size did not allow us to compare the predictive utility of teacher-report SDQ prosocial scores for adult outcomes by classroom type – this would be an interesting area of investigation for future studies.
The SDQ and SSQ are much shorter measures and have been validated much less extensively in autistic individuals than the Vineland. Though the Vineland is more time and labor-intensive, both due to its length and its format as a semi-structured clinician interview, our results suggest the additional efforts required to administer the Vineland are worthwhile for a thorough understanding of social competence in autistic individuals. Unfortunately, the design of this study does not allow us to disentangle rater effects from measurement effects amongst our social competence assessments. It is possible that the clinician perspective afforded by the Vineland, rather than the Vineland itself, increased the predictive utility of this measure. Teacher and caregiver-report questionnaire versions of the Vineland exist, though the predictive utility of these distinct Vineland versions for predicting adult outcomes in individuals with ASD and other developmental conditions have not been examined. Further work is needed to identify the utility of various measures and reporters for conceptualizing social competence in autism and other developmental conditions.
This study partially replicates findings from Project Competence, a seminal study of the impacts of social competence on typical development (Masten et al., Reference Masten, Coatsworth, Neemann, Gest, Tellegen and Garmezy1995). Like Masten and colleagues, even after controlling for IQ, we found adolescent social competence predicted work success, residential status, and the likelihood of having friendships in adulthood for individuals with autism. Whereas childhood IQ was the only significant predictor of ever having had a romantic relationship by age 25 in this study, Masten and colleagues saw that childhood social competence also predicted romantic success in early adulthood for typically developing adults (Masten et al., Reference Masten, Burt, Roisman, Obradovic, Long and Tellegen2004).
Studies of autism and other developmental conditions are sometimes criticized as too niche to provide insight into issues relevant to development in the general population. Yet the similarities between the results of the present study and the results of Project Competence illustrate that there are at least as many parallels between typical and atypical development as there are differences. By focusing research efforts on understanding and helping individuals who are at increased risk of experiencing poor outcomes – regardless of the etiology of that risk – we can gain insight into approaches for fostering healthy development in individuals of all abilities.
Limitations
This sample, initially evaluated in the early 1990’s and followed longitudinally ever since, comprises a unique and relatively small group of adults with ASD. These participants’ families sought help very early in childhood during an era in which ASD services were much less available than they are today. Thus, the participants in this sample may be meaningfully different from individuals diagnosed later in development. Attrition has reduced the number of African American participants and participants with lower caregiver education in this longitudinal cohort. The rate of attrition in this sample is comparable to that observed in other population-based (Gustavson et al., Reference Gustavson, von Soest, Karevold and Røysamb2012) and autism specific (Song et al., Reference Song, Dembo, Smith DaWalt, Ryff and Mailick2023) longitudinal samples. Additionally, we have relatively few female participants in this sample. Though there were no significant gender differences identified in any of the current analyses, our limited number of female participants may have constrained our ability to test for gender differences analyses.
Our measure of work outcomes, the VDI, includes scores specifically for individuals in volunteer, sheltered workshop and supported employment settings, making it a uniquely effective measure for understanding vocational outcomes in ASD. However, it is important to note that high scores on the VDI confound work and post-secondary education. For example, an individual who is working independently for at least 10 hours/week and an individual who is actively enrolled in post-secondary education for at least 10 hours/week would both receive scores of 9 (see Taylor and Seltzer, Reference Taylor and Seltzer2012 for a detailed description of VDI scoring). Though the number of autistic adults pursuing post-secondary education has increased considerably in recent years, there has not been a corresponding increase in employment amongst autistic adults, and prior work in this sample suggests vocational activities are quite stable during the first decade of adulthood for individuals with autism and other developmental conditions (Clarke, Sterrett, et al., Reference Clarke, Sterrett and Lord2021). Thus, VDI scoring may obfuscate meaningful differences in adult work outcomes, particularly for individuals with average or better IQs who are intellectually capable of excelling in post-secondary education, but whose social struggles may limit opportunities for employment success.
Future directions
There is a relative lack of longitudinal samples, both in typical development and in autism, with sufficient data to examine both social competence in early life and outcomes in adulthood. Though expensive and time-consuming, continued longitudinal work is vital to understanding these developmental constructs and their importance across life trajectories. Understanding social competence at different stages of development could have particularly important implications for interventions to support social functioning in ASD. Developmental cascades theory would suggest that the timing of an intervention that improves social competence may be just as or even more important as its content in interrupting negative cascades in social development and promoting positive ones (Bradshaw et al., Reference Bradshaw, Schwichtenberg and Iverson2022; Cox et al., Reference Cox, Mills-Koonce, Propper and Gariépy2010).
Importantly, this study only examined adult outcomes in ASD up to age 26. Adulthood is a long and variable developmental stage. Though in the general population the first decade of adulthood is frequently associated with rapid and considerable change in vocational activities, residential status, and relationships, it is possible autistic adults experience comparable changes somewhat later in adulthood. It remains to be seen whether adults with ASD truly do not attain many traditional markers of adulthood, or rather, that they attain such markers on a delayed timeline compared to the general population. This possibility has not been adequately explored in the existing literature, in part because there is relatively little data, particularly longitudinal data, on autistic adults after the first decade of adulthood. Future work, including subsequent follow-up of the longitudinal cohort described here, should carefully examine outcome attainment in later decades of adult life for individuals with autism and other developmental conditions.
This study is not the first to find evidence that the core symptoms of ASD may be distinct from day-to-day social behavior. Earlier work in a sample of children with ASD and average or better IQ found weak associations between ASD symptomology and adaptive social behaviors (Klin et al., Reference Klin, Saulnier, Sparrow, Cicchetti, Volkmar and Lord2007). Further, a separate longitudinal study of adults with ASD found that the severity of autism symptoms decreased with increasing age; however, participants did not experience a corresponding increase in social connectedness as autism symptoms decreased (Seltzer et al., Reference Seltzer, Krauss, Shattuck, Orsmond, Swe and Lord2003, Reference Seltzer, Shattuck, Abbeduto and Greenberg2004). Additional research is needed to fully explore the potential distinctions (or lack thereof) between core autism symptoms and day-to-day social behaviors, and to examine the relative strength of associations between these constructs during different stages of development.
Defining and characterizing social competence in ASD is one potential avenue for addressing a larger issue in autism research and the study of psychopathology generally: the need for strengths-based approaches (Mottron, Reference Mottron2017; Szatmari et al., Reference Szatmari, Cost, Duku, Bennett, Elsabbagh, Georgiades, Kerns, Mirenda, Smith, Ungar, Vaillancourt, Waddell, Zaidman-Zait and Zwaigenbaum2021). Many studies have indicated higher autism symptom severity and lower IQs decrease the likelihood for positive outcomes in ASD (Lord et al., Reference Lord, McCauley, Pepa, Huerta and Pickles2020; Pickles et al., Reference Pickles, McCauley, Pepa, Huerta and Lord2020), but outside of the present study, few or no analyses have looked at the predictive strength of skills like sharing, being kind to peers, coping well with negative emotions, and similar aspects of social functioning (McChesney & Toseeb, Reference McChesney and Toseeb2018). This is somewhat surprising, as there are interventions for individuals with ASD that target these and related social skills – notably, for adolescents and adults, the Program for Education and Enrichment of Relational Skills (PEERS) program (Laugeson et al., Reference Laugeson, Frankel, Gantman, Dillon and Mogil2012, Reference Laugeson, Gantman, Kapp, Orenski and Ellingsen2015). Though PEERS is a notable exception, many interventions for young children with ASD focus on improving small, concrete aspects of social behavior (for example, joint attention) as opposed to improving social ability more broadly. This emphasis on concrete, molecular aspects of social behavior in many ASD interventions may contribute to the lack of prior work examining social competence as a broader construct in autism.
Arguably, strengths-based approaches – such as considering aspects of social ability that may be relative strengths as in the present study – are especially needed for studies of autism in adulthood (Lounds Taylor, Reference Lounds Taylor2017). Identifying characteristics relevant to quality of life and well-being for autistic adults is another strengths-based approach that has generated increased research interest in recent years (McCauley, Pickles, et al., Reference McCauley, Pickles, Huerta and Lord2020). There are innumerable ways to lead a happy, fulfilling life. Just like typical adults, autistic adults have diverse skill sets and abilities often honed over many years. It would be a disservice to this population not to quantify those strengths nor consider the potential utility of such strengths in promoting positive adult outcomes.
To increase replicability with the existing literature on typical development, this study focused on normative adult outcomes (work, residential status, friends, and romantic relationships). Some autistic self-advocates might argue that the achievement of one or more of these outcomes is not necessary to leading a fulfilling adult life (Pukki et al., Reference Pukki, Bettin, Outlaw, Hennessy, Brook, Dekker, Doherty, Shaw, Bervoets, Rudolph, Corneloup, Derwent, Lee, Rojas, Lawson, Gutierrez, Petek, Tsiakkirou, Suoninen and Yoon2022). There is some evidence that autistic adults do not derive as much satisfaction from employment as their typical peers (Black et al., Reference Black, Mahdi, Milbourn, Thompson, D’Angelo, Ström, Falkmer, Falkmer, Lerner, Halladay, Gerber, Esposito, Girdler and Bölte2019), and some autistic adults report little or no interest in having friends and/or romantic relationships. However, the financial stability associated with employment is an economic necessity for most adults, and many autistic individuals of all ages express a desire for more social connections (Bauminger & Kasari, Reference Bauminger and Kasari2000; Dewinter et al., Reference Dewinter, De Graaf and Begeer2017). Further, loneliness is a widespread concern for autistic individuals across the lifespan (Locke et al., Reference Locke, Ishijima, Kasari and London2010; Umagami et al., Reference Umagami, Remington, Lloyd-Evans, Davies and Crane2022). In short, though some members of the autism community might contest the validity of these outcome measures, employment and social connection are sensible benchmarks of success for the vast majority of adults – both with and without an ASD diagnosis.
Perhaps the largest challenge to future research in this area is conceptualizing what social competence means for individuals diagnosed with a disorder of social communication. Even in the typical literature, conceptualizations and measures of social competence vary both by participant age group and from study to study. Some common measures of typical social competence, such as peer nominations and other indicators of classroom popularity, may be less meaningful for understanding social competence in ASD, particularly for autistic children or adults who spend all or part of their day in segregated classrooms or other segregated settings. Instead, measures of distinct aspects of social functioning that may be less impacted by core features of autism – such as prosocial behavior, emotional coping, and cooperation – may be more informative indicators of social competence in autistic individuals. Future research is needed to confirm this.
Conclusions
This study attempted to characterize social competence in ASD by employing a longitudinal sample of individuals with ASD and related developmental conditions to replicate well-established findings from typical development that adolescent social competence predicts success in normative adult outcomes. We saw that individuals with ASD followed either a high or low trajectory of social competence development from ages 2 to 26. Both trajectories increased from early childhood to early adulthood, though social skills in the high trajectory group increased at a significantly faster rate. We also found that relatively high scores in adolescence on two measures – Vineland Social domain age equivalence scores and Social Skills Questionnaire total scores – predicted the likelihood of having friendships in early adulthood, and one measure, Vineland Social-AE scores, also predicted the likelihood of achieving employment and living independently. None of our social competence measures from adolescence predicted the likelihood of ever having a romantic relationship by age 25, however. Future studies should continue to move towards a worthwhile definition of social competence in ASD and should leverage strengths-based approaches to define and examine meaningful adult outcomes in this population.
Acknowledgements
The authors would like to acknowledge the time participants and families have given to this project and thank them for their efforts. The authors would also like to acknowledge Dr. Julie Lounds Taylor for her thoughtful input on early versions of this manuscript. This study was funded by the National Institute of Child Health and Human Development R01 HD081199 (PI: CL), the National Institute of Mental Health R01MH081873 (PI: CL), and Autism Speaks 12854 (PI: EC/CL)
Funding statement
This study was funded by the National Institute of Child Health and Human Development R01 HD081199 (PI: C.L.), the National Institute of Mental Health R01MH081873 (PI: C.L.), and Autism Speaks 12854 (PI: E.B.C./C.L.).
Competing interests
CL acknowledges the receipt of royalties from the sale of the Autism Diagnostic Observation Schedule-2 (ADOS-2) and the Autism Diagnostic Interview-Revised (ADI-R). Royalties generated from this study were donated to a not-for-profit agency, Have Dreams. E.B.C has no conflicts of interest to declare.







 Open access
Open access