



Introduction
Multiple sclerosis (MS) symptoms can have a significant effect on sleep. Poor sleep quality caused by sleep disturbances may lead to problems with mood, energy, and even an increase in MS symptoms (Sakkas, Giannaki, Karatzaferi & Manconi, Reference Sakkas, Giannaki, Karatzaferi and Manconi2019). Sleep disturbances are three times more common in people with MS as compared to the general population (Lobentanz et al., Reference Lobentanz, Asenbaum, Vass, Sauter, Klösch, Kollegger, Kristoferitsch and Zeitlhofer2004) and can be subdivided into primary and secondary sleep disorders. One of the most prevalent primary sleep disorders seen in patients with MS is insomnia (Alhazzani et al., Reference Alhazzani, Alshahrani, Alqahtani, Alamri, Alqahtani, Alqahtani and Alahmarii2018; Bøe Lunde et al., Reference Bøe Lunde, Aae, Indrevåg, Aarseth, Bjorvatn, Myhr and Bø2012; Uhlig, Sand, Ødegård & Hagen, Reference Uhlig, Sand, Ødegård and Hagen2014; Vitkova et al., Reference Vitkova, Rosenberger, Gdovinova, Szilasiova, Mikula, Groothoff and van Dijk2016;). It is accompanied by significant psychological distress and/or impairment in daytime functioning (Sateia, Reference Sateia2014), and correlates significantly with quality of life (QOL) in patients with MS (Schellaert et al., Reference Schellaert, Labauge, Lebrun, Maudarbocus, Bernard, Blache and Bayard2018; Vries, Reference Vries, Verster, Pandi-Perumal and Streiner2008).
Sleep disorders can be complicated with respiratory muscle weakness (Howard et al., Reference Howard, Wiles, Hirsch, Loh, Spencer and Newsom-Davis1992), which frequently occurs in patients with advanced MS. Recognition of MS patients at risk for respiratory complications allows for the timely implementation of care and measures to decrease disease-associated morbidity and mortality (Tzelepis & McCool, Reference Tzelepis and McCool2015). Nevertheless, recent studies suggest that respiratory muscles can be trained for both strength and endurance in patients with MS (Grubić Kezele, Babić & Štimac, Reference Grubić Kezele, Babić and Štimac2019; Grubić Kezele, Babić, Kauzlarić-Živković & Gulić, Reference Grubić Kezele, Babić, Kauzlarić-Živković and Gulić2020; Ray, Udhoji, Mashtare & Fisher, Reference Ray, Udhoji, Mashtare and Fisher2013).
Sleep disturbances are the largest contributor to fatigue, followed by depression and disease severity (Strober & Arnett, Reference Strober and Arnett2005, Vries, Reference Vries, Verster, Pandi-Perumal and Streiner2008). Sleep disturbances, psychological distress and fatigue are often co-existing in MS and thereby influence and intensify each other (Vries, Reference Vries, Verster, Pandi-Perumal and Streiner2008). However, fatigue and psychological distress are usually direct effects of MS regardless of sleep quality (Grubić Kezele, Babić & Štimac, Reference Grubić Kezele, Babić and Štimac2019; Grubić Kezele, Babić, Kauzlarić-Živković & Gulić, Reference Grubić Kezele, Babić, Kauzlarić-Živković and Gulić2020), and they belong to secondary sleep disorders.
Secondary sleep disorders can result from a clinical variety of symptoms seen in MS (Nicholas & Rashid, Reference Nicholas and Rashid2013), like pain, muscle spasticity, unpleasant tingling sensations, frequent nighttime urination, which usually lead not only to less sleep but also reduce the time spent in deep sleep. Medications and a lack of exercise (Grubić Kezele, Babić, Kauzlarić-Živković & Gulić, Reference Grubić Kezele, Babić, Kauzlarić-Živković and Gulić2020; Grubić Kezele, Babić & Štimac, Reference Grubić Kezele, Babić and Štimac2019) due to MS-related disabilities also harm sleep.
To improve sleep and possibly prevent long-term health consequences of poor sleep in MS, exercise could be a non-pharmacological, inexpensive and safe method (Al-Sharman, Khalil, El-Salem, Aldughmi & Aburub, Reference Al-Sharman, Khalil, El-Salem, Aldughmi and Aburub2019). Siengsukon and coworkers (Siengsukon et al., Reference Siengsukon, Aldughmi, Kahya, Bruce, Lynch, Ness Norouzinia and Billinger2016) have compared two different exercise programs on individuals with MS, i.e., moderate-intensity aerobic exercise and low-intensity walking and stretching in a 12-week exercise study, where only a low-intensity program showed a significant effect on sleep quality, and moderate-intensity program showed a significant effect on daytime sleepiness.
Here, we wanted to examine the feasibility and possible effect of a mild 8-week exercise program including breathing exercise on sleep quality, insomnia, psychological distress and fatigue in individuals suffering from MS with the Expanded Disability Status Scale (EDSS) score ranging from 1 to 7.5 and compare to individuals with MS who didn’t exercise. We hypothesize that 8 weeks of a continuous upper limb-lower limb (UL-LL) exercise program with an emphasis on breathing can efficiently attenuate psychological distress, insomnia and fatigue and improve the quality of sleep in individuals with MS.
Methods
Participants
The patients with diagnosed MS (by a neurologist in Clinical Hospital Center Rijeka, Croatia) were randomly selected from the MSSC register Primorje-Gorski Kotar County in Croatia using the code numbers of registered members. To determine the participants’ interest in the research, the first contact was established by phone by a blinded researcher. From 34 potential participants, 24 individuals with MS were recruited from the MSSC. Participant flow through enrolment is included in the Consolidated Standards of Reporting Trials (CONSORT) diagram (Fig. 1).
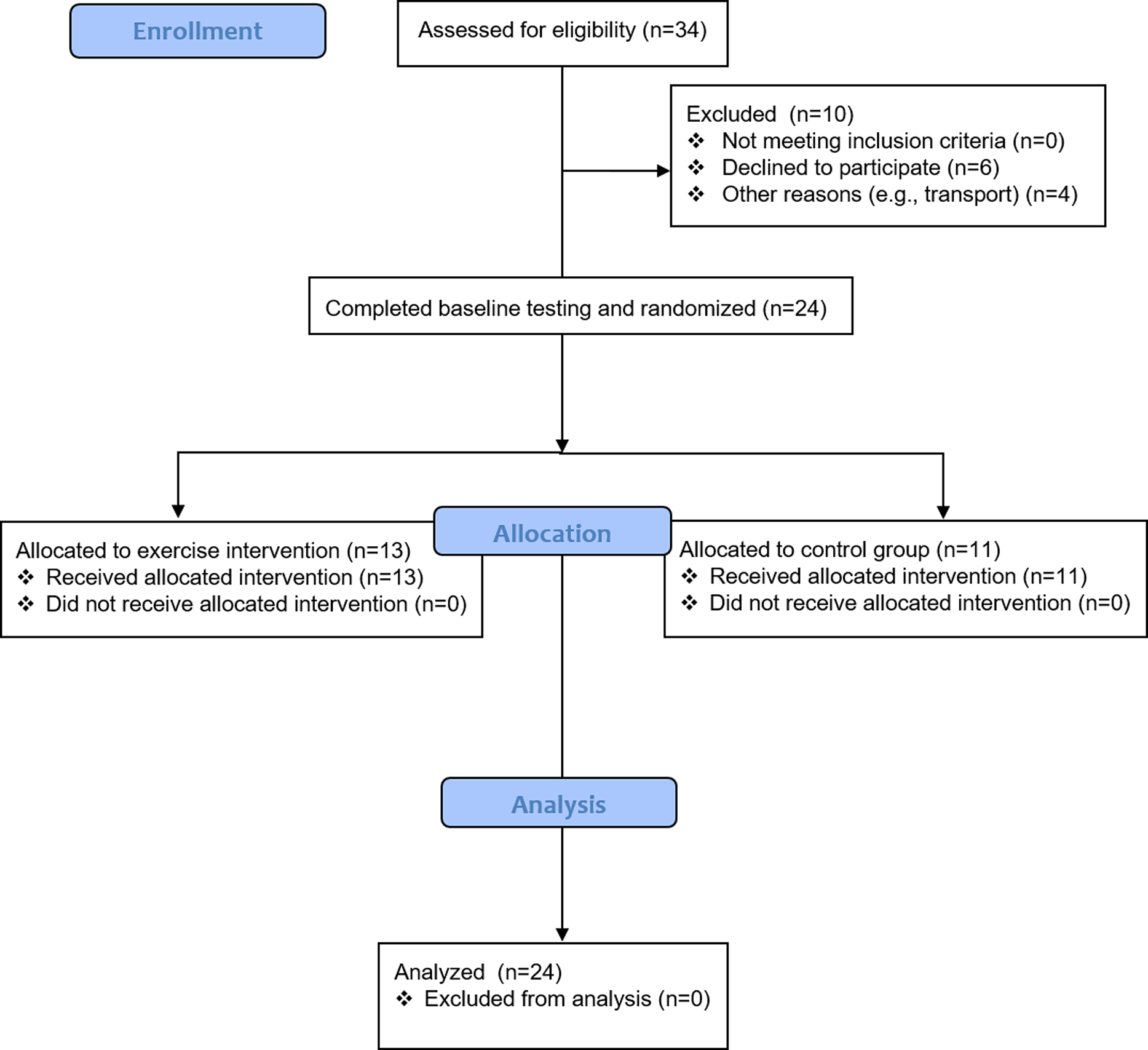
Figure 1. Participants’ flow chart.
Before being included in the study, all 24 individuals were invited to the MSSC to determine if they met the study inclusion and exclusion criteria checked by two different physicians.
One physician (A.F.S.) assessed the participants’ characteristics (sex, age, medications) and the other one (T.G.K.), who was trained to assess EDSS status, as well the type of MS based on standard diagnostic criteria (McDonald et al., Reference McDonald, Compston, Edan, Goodkin, Hartung, Lublin and Wolinsky2001) (Table 1), confirmed EDSS scores.
Table 1. Characteristics of the subjects and medications
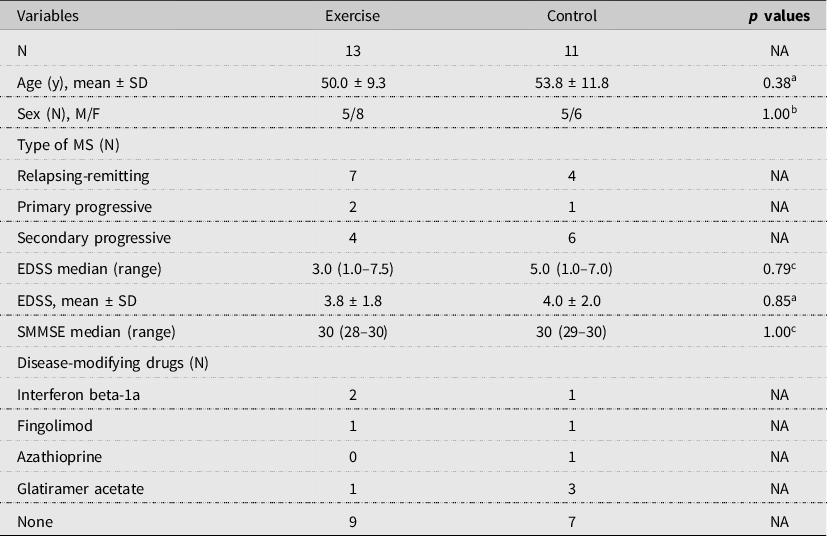
Note. Noncategoric values are expressed as mean ± SD. Categoric values are expressed as median (range).
Abbreviations: EDSS, expanded disability status scale; F, female; M, male; SMMSE, standardized mini-mental state examination.
a Student’s t-test.
b Chi-square.
c Mann-Whitney test.
P < 0.05 is significant. NA, not applicable.
The inclusion criteria were: a diagnosis of MS with mild to severe disability (EDSS score between 0.0 [normal neurological exam] and 7.5 [unable to take more than a few steps. Restricted to a wheelchair], presence of any kind of sleep disturbance determined by the interview, adults between the age of 18 and 80 years, patients with Standardized Mini-Mental State Examination (Vertesi et al., Reference Vertesi, Lever, Molloy, Sanderson, Tuttle, Pokoradi and Principi2001) >24 and with no contraindications for performing breathing and UL-LL exercises.
The exclusion criteria were: an exacerbation of MS or corticosteroid treatment within the past 8 weeks, presence of concomitant neurological and musculoskeletal disorders affecting arms and/or legs, acute or chronic lung pathologies, breathing difficulties or any other serious illness that might interfere with the intervention, untreated known sleep disorder (as sleep apnea, etc.), a history of schizophrenia spectrum or other psychotic disorders, substance-related and addictive disorders. Participants using MS disease-modifying drugs and psychotropic medications were not excluded, as well those with current anxiety and mood disorders.
All subjects signed a written informed consent and the study was approved by the Ethics Committee of Faculty of Health Studies in Rijeka (003-08/18-01/05), and registered with ClinicalTrials.gov (NCT03768830). Subject characteristics and medications are presented in Table 1.
Study design
This study has a randomized controlled parallel-group design and was performed in the MS Society Center (MSSC) of Primorje-Gorski Kotar County in Croatia.
The MSSC is the official but familiar meeting place (counting about 213 members till now) with enough space for performing exercises. The sample size was not determined based on power analysis given the pilot nature of the study (Abbott, Reference Abbott2014). It was designed to verify the feasibility of a UL-LL and breathing exercise and to explore possible effects on sleep quality, insomnia, psychological distress and fatigue in a group of individuals with MS for the future larger trial.
All 24 participants, who met the criteria after clinical and neurological examinations, were randomly assigned into two groups based on the EDSS score (Table 1) (Kurtzke, Reference Kurtzke1983), so each group could include participants with a similar range of the EDSS scores. The EDSS score was chosen by the researcher (A.F.S.) without knowing any other information about the participant, i.e., name, surname, MS type, disease duration, etc., using the coded cards. The physician (T.G.K.) who assessed the participants EDSS scores, coded each participant on a card so each card included only an EDSS score and number for the certain participant. The baseline testing (pre-testing) was performed during five days by an independent researcher who was blinded to the allocation group of the patients in the MSSC.
The exercise group exercised under physiotherapist guidance (Z.T., V.A. and N.R.) and the control group performed no exercise. The exercise group exercised 8 weeks, 2d/week and 60 min/session in the MSSC.
The control group performed no exercise during the investigation but they were required to visit the MSSC for 8 weeks, 2d/week (≤60 min), where they could freely socialize, having thereby approximately the same contact with the investigators as the exercise group. The control group was offered the exercise program at the end of the study, which everyone accepted.
At the end of the study (the day after the last session), outcome measures (post-testing) were collected by the same independent researcher blinded to allocation, who performed the baseline testing. In addition, participants from the intervention group completed a questionnaire composed of questions related to their motivation during the study. The blind assessor helped participants with all questionnaires, readout and explained each question. Scoring of all tests was performed by physicians, regardless of whether they are self- or physician-rated (H.O. and L.Đ).
Outcome measures
Sleep quality
The sleep quality was measured using the Pittsburgh Sleep Quality Index (PSQI). The PSQI is a self-rated questionnaire that assesses sleep quality and disturbances over a 1-month time interval (Buysse, Reynolds, Monk, Berman, & Kupfer, Reference Buysse, Reynolds, Monk, Berman and Kupfer1989). The test distinguishes poor quality from good quality sleep by measuring seven components that include: subjective sleep quality, sleep duration, sleep disorders, use of sleep medications, and daily disorders that have occurred in the past month. Test results are obtained by adding the points for each component and the total. The global PSQI score is the sum of all components scores (range: 0–21); a score ≥5 represents poor sleepers; <5 represents patients with normal sleep quality. In our sample Cronbach’s alpha was 0.81 for the general score and subscales in the following order; 0.72 for the sleep quality, 0.79 for the sleep latency, 0.87 for the sleep duration, 0.78 for the sleep efficiency, 0.64 for the sleep disturbances, 0.76 for the sleep medications and 0.91 for the daytime sleep dysfunction.
Insomnia severity
The insomnia severity was measured using the Insomnia Severity Index (ISI). The questionnaire is a reliable, valid self-rated measurement tool used to assess the nature, severity, and impact of insomnia on the QOL in adults (Alhazzani et al., Reference Alhazzani, Alshahrani, Alqahtani, Alamri, Alqahtani, Alqahtani and Alahmarii2018; Bastien, Vallières & Morin, Reference Bastien, Vallières and Morin2001; Morin, Belleville, Bélanger & Ivers, Reference Morin, Belleville, Bélanger and Ivers2011). The ISI comprises seven items assessing the perceived severity of difficulties initiating sleep, staying asleep, and early morning awakenings, satisfaction with current sleep pattern, interference with daily functioning, noticeability of impairment attributed to the sleep problem, and degree of distress or concern caused by the sleep problem. Each item is rated on a scale from 0 to 4 from less to more severe. The total score is the sum of each item and can range from 0 to 28 (28 = most severe insomnia). According to the total sum, the severity of insomnia or sleep disorders is categorized: a score of 0–7 represents ‘clinically unknown insomnia’, 8–14 ‘mild subclinical insomnia’, 15–21 ‘moderate clinical insomnia’, while a sum of 22–28 represents ‘severe clinical insomnia’. The ISI assesses insomnia severity over the last 2-week time interval. Cronbach’s alpha was 0.94 in our sample.
Psychological distress
The psychological distress in the last two weeks was measured using the Clinical Outcomes in Routine Evaluation (CORE-OM). The CORE-OM is a scale designed as a multi-theoretical and multi-diagnostic measure of general psychological distress used by the therapist before and after therapy. It is a reliable and valid self-report 34-item instrument with domains of subjective well-being, problems/symptoms, life functioning and risk/harm (Evans et al., Reference Evans, Connell, Barkham, Margison, McGrath, Mellor-Clark and Audin2002; Jokić-Begić, Lauri Korajlija & Jurin, Reference Jokić-Begić, Lauri Korajlija and Jurin2014). Higher total raw scores total (range 0–136) represent poorer overall functioning. Scores are presented as 1–20 healthy, 21–33 low level of psychological distress, 34–50 mild, 51–67 moderate, 68–84 moderate to severe and 85–136 severe psychological distress. Cronbach’s alpha was 0.86 in our sample.
Fatigue
Fatigue was measured using the Modified Fatigue Impact Scale (MFIS). It is a reliable, valid self-report measurement tool used to assess the impact of fatigue on physical, cognitive and psychosocial functioning within the past 4 weeks (Fisk et al., Reference Fisk, Ritvo, Ross, Haase, Marrie and Schlech1994; Larson, Reference Larson2013; Pekić, Kragujević, Kampić & Ukić, Reference Pekić, Kragujević, Kampić and Ukić2017; Pilutti, Greenlee, Motl, Nickrent & Petruzzello, Reference Pilutti, Greenlee, Motl, Nickrent and Petruzzello2013). The MFIS contains 9 ‘physical’ items, 10 ‘cognitive’ items, and 2 ‘psychosocial’ items. Each item is rated on a scale from 0 to 4 from never to always. The maximum possible score is 84, with higher scores indicating a greater impact on quality of life. In our sample, Cronbach’s alpha was 0.93 for the general score, 0.89 for the physical, 0.95 for the cognitive and 0.19 for the psychosocial subscale.
Exercise protocol
The physiotherapist first demonstrated and explained each exercise. The exercise program was performed with both visual feedback (the physiotherapist exercised together with the participants) and continuous verbal orders from the physiotherapist. Adherence was monitored every week by registering the number of completed sessions at the MSSC. During the exercise, the participants were sitting on a chair. The exercise program (the range of motions, resistance of elastic bands, exercise speed) was individually adapted to each patient. The participants were told to stop exercising if they felt tired, weak, pain or any other discomfort. After each exercise, there was a 30–60 sec pause. Each exercise began with 15 min of warm-up divided into 2 parts: diaphragmatic and thoracic breathing (5 min) and active mobility of the ULs and LLs (10 min; 5 min each).
For the breathing exercises, the basic principle was to inhale and exhale as completely as possible, but slowly to prevent hyperventilation and dizziness. Diaphragmatic or abdominal breathing (1.5 min) was performed for the strengthening of the abdominal muscles and the diaphragm, and _ thoracic breathing (1.5 min) for strengthening the intercostal muscles (3×-20 sec pause-3×). After warming up, each UL exercise was divided into 3 parts: range movement (5 min), coordination (5 min) and strengthening exercises with minimal resistance (5 min). LL exercise included range movement (10 min) and strengthening exercises (10 min). Slow deep breathing through the nose followed every movement. The exercises were performed bilaterally, one arm after another (10× if tolerated), and then simultaneously (5×) with a 30–60 sec pause in between. If the participants could not perform 10× each arm separately, they stopped at 5 or less and had a long pause. Exercises for coordination and arm strengthening started from the proximal to the distal joints. Range movement exercises for the UL included arm elevations, elbow flexion-extension, elbow flexion in combination with shoulder abduction and wrist flexion-extension. Coordination exercises for the UL included open and closed eyes with elbow flexion with touching the ipsilateral shoulder/ear, or contralateral shoulder/ear. Strengthening exercises for the UL were performed with dumbbells (0.5 kg) or elastic straps (Elastic bands, TheraBand; The Hygenic Corporation), and only with elastic straps for the LL. Exercise with dumbbells included arm elevation, internal shoulder rotation, elbow flexion-extension and wrist flexion-extension. Exercise with elastic straps included arm elevation, a diagonal combination of shoulder external rotation, elbow flexion-extension, and for the LL parallel lateral hip abduction in a sitting position with knee flexion, hip abduction with extended knee or hip extension in a standing position withholding for a chair. Range movement exercises for the LL included hip flexion in combination with knee flexion, knee flexion-extension, hip abduction and adduction in a sitting position, and with an extended knee in a standing position.
At the end of the training session, the last 10 min were devoted to static stretching of the muscle groups, which were used during exercising. After each exercise session, the participants were asked if they have felt any psychological or physical discomfort during or after the exercise, including fatigue or else.
Data analysis
Data were analyzed using the software program Statistica, Version 13.3. Descriptive statistics examined the demographic and clinical measures within the 2 groups at the start of treatment and Student’s t-test, Mann-Whitney test and Chi-square were used to confirm the 2 groups were comparable (Table 1). These data are presented by mean and standard deviations (SD) (e.g., age, EDSS), median and range (e.g., EDSS, SMMSE) and as total number (e.g., sex, MS type, medications).
The outcome data (PSQI, ISI, CORE-OM and MFIS) were analyzed within and between intervention and control groups (Tables 2 and 3). The distribution of data was normal according to Kolmogorov-Smirnov test (PSQI, ISI, CORE-OM and MFIS). To compare pre- with post-exercise data in exercise and control groups, Student’s t-test for dependent variables was used (Tables 2 and 3) (Ray et al., Reference Ray, Udhoji, Mashtare and Fisher2013).
Table 2. Quality of sleep and psychological distress status
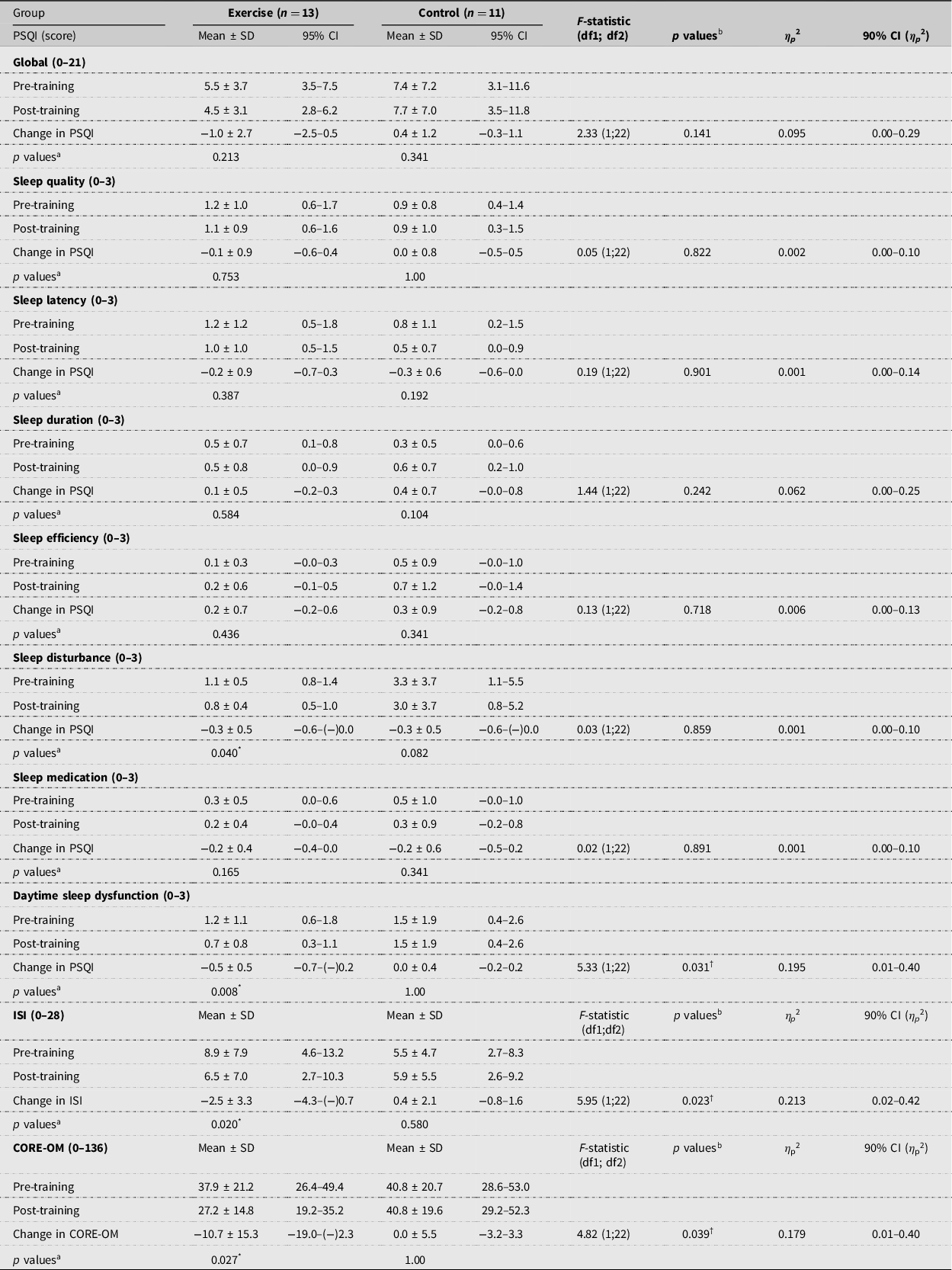
Abbreviations: CI, confidence interval; CORE-OM, clinical outcomes in routine evaluation – outcome measure; ISI, insomnia severity index; PSQI, pittsburgh sleep quality index. F-statistic is presented for group-by-time interaction. df1, degree of freedom for group-by-time interaction; df2, degree of freedom for Error. Effect size shown as Partial Eta Squered (η p2).
* Significance between pre- and post-data within group.
a Student’s t-test.
b ANOVA.
Values are expressed as mean ± SD. P < 0.05 is significant.
† Significance between changes in each group.
Table 3. Fatigue measures (physical, cognitive, psychosocial and total)
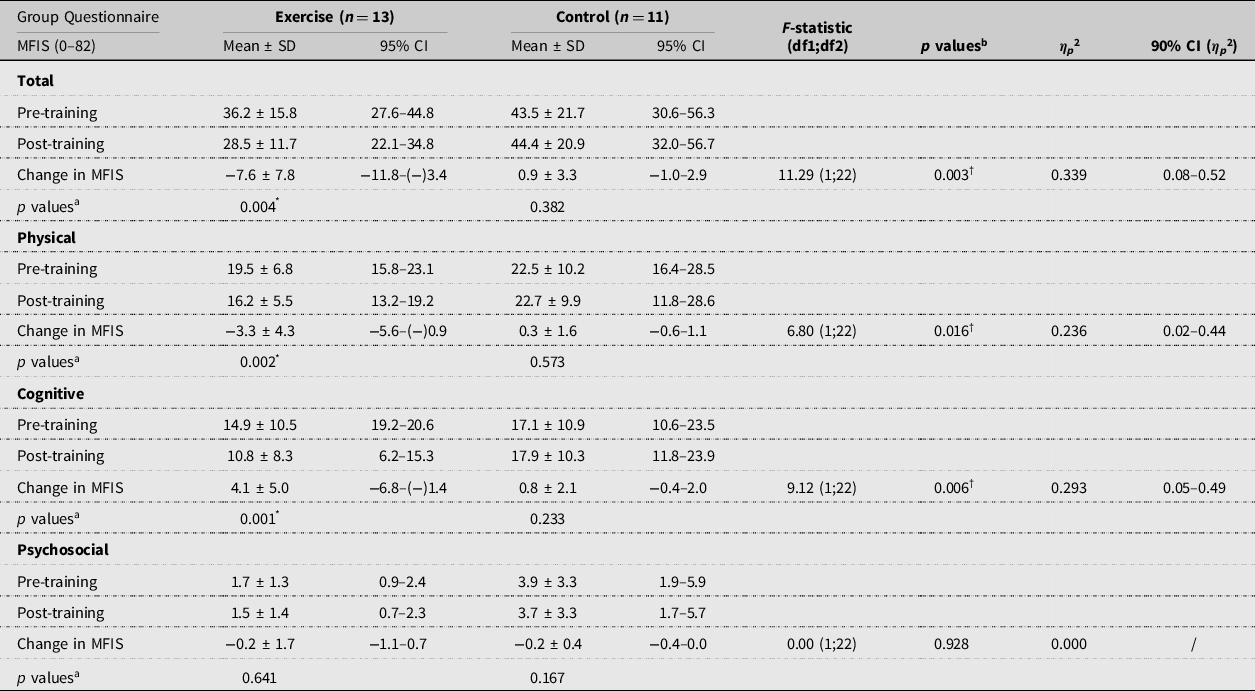
Abbreviations: CI, confidence interval; MFIS, modified fatigue impact scale. F-statistic is presented for group-by-time interaction. df1, degree of freedom for group-by-time interaction; df2, degree of freedom for Error. Effect size shown as Partial Eta Squered (η p2).
a Student’s t-test.
b ANOVA.
Values are expressed as mean ± SD. P < 0.05 is significant.
* Significance between pre- and post-data within group.
† Significance between changes in each group.
The analytic model that involved a 2-way mixed-model, repeated-measures analyses of variance (ANOVA) on the outcome measures, with time (pre and post) included as a within-subjects factor, and group (exercise or control) included as a between-subjects factor, provided the same interaction p values (group-by-time) as Student’s t-test for comparing between groups pre- to post-intervention changes (Tables 2 and 3). A nominal significance level of 0.05 was used in all testing.
Given that the current study involved a small sample, reaching statistical significance in many measures was unlikely. Also, since p values alone don’t indicate the size of an effect, or that non-statistically significant effects can have important clinical significance, we computed effect sizes for the F-statistic (partial eta squared; η p 2) and they were reported and interpreted as criteria: small (0.01), moderate (0.06), and large (0.14) (Cohen, Reference Cohen1988). We further report the Pearson correlations coefficient (r) among values in the CORE-OM, ISI, PSQI and MFIS (Table 4).
Table 4. Pearson correlations (r) among values in CORE-OM, ISI, PSQI and MFIS in all 24 individuals with MS

Abbreviations: CORE-OM, clinical outcomes in routine evaluation – outcome measure; ISI, insomnia severity index; PSQI, Pittsburgh sleep quality index; MFIS, modified fatigue impact scale.
* Denotes statistical significance at P < 0.05.
Results
Compliance
The 8-week upper-lower limb and breathing exercise training intervention was well-tolerated. Compliance with exercise sessions were recorded in weekly exercise logs for each participant. Overall compliance (i.e., percentage of exercise sessions attended over the 8-week intervention) was 94%. All 13 participants completed at least 88% of sessions (i.e., 14 of 16 possible sessions guided by a physiotherapist) and complied with the prescribed intensity and duration of each exercise session.
All 24 participants completed the assessments. The participants recorded no harm or discomfort during the exercise sessions and subjectively stated they had no lack of energy, no increased sensory symptoms nor increased fatigue after each exercise training. In our study muscle weakness partly influenced the feasibility of the exercise in some participants. However, the repetition of individual exercises was carried out to their limits or when they felt weakness or discomfort, especially during exercise with elastic straps, which were the hardest for them. Most important, they did not feel pain. Therefore, 60 min of continuous exercising with the upper and lower limbs, including breathing exercises and stretching, was successfully carried out. Tables 2 and 3 show the outcome measures at baseline and post-exercise program, pre- to post-intervention mean differences, and within- and between-group comparisons for the subject with MS. Table 2 shows the PSQI, ISI and CORE-OM variables, and Table 3 shows the MFIS variables.
Outcome measures
Post-intervention values of the outcomes, pre- to post-intervention mean differences, and within- and between-group (group-by-time interaction) comparisons are shown in Table 2 and 3.
Sleep quality and insomnia
There was a small non-significant improvement in most of PSQI subcategories within the exercise group (Table 2), but the statistical significance showed only subcategories of daytime sleep dysfunction (95% CI = −0.7–(−)0.2, p = 0.008) and sleep disturbance (95% CI = −0.6–(−)0.0, p = 0.040). However, there was only a statistically significant between-group difference on the PSQI daytime sleep dysfunction scores (F(1;22)=5.33, p = 0.031) with large effect score (η p 2 = 0.195, 90% CI = 0.01–0.40) (Table 2).
There was a statistically significant between-group difference on the ISI scores (F(1;22)=5.95, p = 0.023) with a large effect score (η p 2 = 0.213, 90% CI = 0.02–0.42) (Table 2). Within-group analysis showed a significant improvement on ISI scores in the exercise group (95% CI = −4.3–(−)0.7, p = 0.020). However, non-significant within-group differences were found in the control group.
Psychological distress
There was a statistically between-group difference on the CORE-OM scores (F(1;22)=4.82, p = 0.039) with a large effect score (η p 2 = 0.179, 90% CI = 0.01–0.40). Within-group analysis showed a significant improvement on CORE-OM scores in the exercise group (95% CI = −19.0–(−)2.3, p = 0.027). No significant change was found in the control group.
Fatigue
There was a statistically significant between-group difference on the MFIS scores: physical: F(1;22)=6.80, p = 0.016; cognitive: F(1;22)=9.12, p = 0.006; and total: F(1;22)=11.29, p = 0.003, with overall large effect scores (physical: η p 2 = 0.236, 90% CI = 0.02–0.44; cognitive: η p 2 = 0.293, 90% CI = 0.05–0.49 and total: η p 2 = 0.339, 90% CI = 0.08–0.52) (Table 2). Within-group analysis showed a significant improvement on MFIS scores in the exercise group (physical: 95% CI = −5.6–(−)0.9, p = 0.002; cognitive: 95% CI = −6.8–(−)1.4, p = 0.001; and total: 95% CI = −11.8–(−)3.4, p = 0.004). These variables did not change significantly for the subjects in the control group.
Correlations among outcome measures
The PSQI was in correlation with the ISI (r = 0.85, p < 0.001), with the CORE-OM (r = 0.59, p = 0.001) and with the MFIS (r = 0.73, p < 0.001) scores. In addition, the ISI was in correlation with the CORE-OM (r = 0.53, p = 0.003) and with the MFIS (r = 0.71, p < 0.001) scores. Furthermore, the CORE-OM was also in correlation with the MFIS scores (r = 0.75, p < 0.001) (Table 4).
Discussion
Our research has shown that an exercise program with an emphasis on breathing could be beneficial for attenuating insomnia severity and improving the sleep quality and psychological status in individuals with MS. Namely, the sleep quality was significantly improved only in two subcategories of PSQI within the exercise group, i.e., sleep disturbance and daytime sleepiness (Tables 2). Furthermore, the only variable which has shown a statistically significant group by time interaction was daytime sleepiness (Table 2), indicating there was a difference in change in daytime sleepiness between groups. This is interesting since, in a study by Siengsukon et al. (Reference Siengsukon, Aldughmi, Kahya, Bruce, Lynch, Ness Norouzinia and Billinger2016), this is the only variable (assessed by the Epworth Sleepiness Scale) on which their supervised moderate-intensity aerobic exercise program had a significant effect, unlike the low-intensity walking and stretching program. Both their programs had a moderate non-significant impact on the global PSQI score as our program, but only their low-intensity walking and stretching program had a statistically significant impact on the global PSQI (Siengsukon et al., Reference Siengsukon, Aldughmi, Kahya, Bruce, Lynch, Ness Norouzinia and Billinger2016). This proves that program design is a very important part of the investigation that includes people with MS. It has been already shown, as well as in our previous research, that physiotherapy exercise involving the upper limbs has a beneficial impact on final pulmonary function, exercise capacity and QOL (Grubić Kezele et al., Reference Grubić Kezele, Babić and Štimac2019, Reference Grubić Kezele, Babić, Kauzlarić-Živković and Gulić2020; Grubić Kezele, Medjimurec, Bukarica, Čorapović & Fužinac-Smojver, Reference Grubić Kezele, Medjimurec, Bukarica, Čorapović and Fužinac-Smojver2019; Kaymaz et al., Reference Kaymaz, Candemir, Ergün, Demir, Taşdemir and Demir2018). Thus, it is likely that UL-LL and breathing exercise in our 8-week study contributed to the strengthening of the UL and LL and respiratory muscles (see limitations) and increased the exercise capacity, thus reduced fatigue, psychological distress and insomnia, and consequently increased the quality of sleep (Table 2, 3) (Cramer, Lauche, Azizi, Dobos & Langhorst, Reference Cramer, Lauche, Azizi, Dobos and Langhorst2014; Sadeghi Bahmani et al., Reference Sadeghi Bahmani, Kesselring, Papadimitriou, Bansi, Pühse, Gerber and Brand2019; Siengsukon et al., Reference Siengsukon, Aldughmi, Kahya, Bruce, Lynch, Ness Norouzinia and Billinger2016).
Furthermore, our exercise program reduced total, physical, and cognitive fatigue in subjects with MS as well (Table 3). Indeed, regular exercise, in general, can prevent the lung volume decrease and the development of various disorders including deconditioning (Cramer, Lauche, Azizi, Dobos & Langhorst, Reference Cramer, Lauche, Azizi, Dobos and Langhorst2014). In addition, in our study we found moderate and significant correlations of MFIS and CORE-OM scores with ISI and PSQI scores (Table 4), indicating their causal-consequence relationships. In other words, fatigue and psychological distress were related to insomnia severity and sleep quality either at baseline or at study end. Although it is hard to assume, which of these symptoms improved first during the exercise program, at the end, that is less important, if we know these symptoms are connected, especially in MS (Vries, Reference Vries, Verster, Pandi-Perumal and Streiner2008). We assume that the exercise program helped to reduce psychological distress, fatigue and pain (data not shown) and thus improved the perception of sleep quality.
Besides the exercise itself, deep breathing exercise contributed as a relaxation technique (Cramer et al., Reference Cramer, Lauche, Azizi, Dobos and Langhorst2014; Perciavalle et al., Reference Perciavalle, Blandini, Fecarotta, Buscemi, Di Corrado, Bertolo and Coco2017) to reducing the psychological distress that has a great negative impact on sleep quality (Schellaert et al., Reference Schellaert, Labauge, Lebrun, Maudarbocus, Bernard, Blache and Bayard2018). In the study by Bahmani and coworkers, the regular 3-week exercise program accomplished a reduction of symptoms of sleep complaints, depression, fatigue, and paresthesia, and improvement of both objective and subjective sleep (Sadeghi Bahmani et al., Reference Sadeghi Bahmani, Kesselring, Papadimitriou, Bansi, Pühse, Gerber and Brand2019), which is consistent with our results.
However, the upper limit of EDSS scores in Bahmani’s study was 6.0, unlike in our study, with the upper limit of 7.5. That is to say how a greater EDSS score can be a limiting factor for performing physical activity and accomplishing better results.
In addition, the participants in our research subjectively stated in the questionnaire upon completion of the exercise, that this exercise program in the group motivated them a lot and helped them accomplish more during the day, in a physical manner. Thus, we cannot rule out the impact of a social-supportive familiar and less stressful surrounding with other MS individuals on motivation during the exercise as well.
Despite its high prevalence, sleep disorders and poor sleep quality surprisingly remain underdiagnosed and, therefore, undertreated in MS (Brass, Li & Auerbach, Reference Brass, Li and Auerbach2014). Investigating factors that co-exist with sleep disorders and poor sleep quality, such as psychological distress and fatigue in patients with MS, may provide clues for an increased understanding of underlying pathophysiology and contribute to developing targeted therapeutic interventions.
To our knowledge, no other reports are examining the effects of an 8-week combined UL-LL and breathing exercise on sleep quality, insomnia, psychological distress and fatigue in subjects with MS with the EDSS between 1.0 and 7.5. Furthermore, this early-phase randomized controlled trial in a small sample is important for promoting innovation, reducing Type II error, and providing evidence against the premature dismissal of a possibly beneficial intervention (Grubić Kezele, et al., Reference Grubić Kezele, Babić and Štimac2019, Reference Grubić Kezele, Babić, Kauzlarić-Živković and Gulić2020; Sandroff et al., Reference Sandroff, Balto, Klaren, Sommer, DeLuca and Motl2016). It represents a minimal equipment exercise program in a sitting position that may be recommended to patients having an EDSS score between 1.0 and 7.5 as a home base program but needs further larger trials to confirm it.
Study limitations
There are several limitations of the current investigation, which need to be mentioned. Firstly, owing to the small sample size, our results cannot be generalized to all individuals with MS. The current study may have been underpowered for detecting statistically significant effects on the quality of sleep since it involved a small convenience sample (N = 24). Therefore, there is undoubtedly a need for repeating this investigation in a larger group of participants.
Those improvements could also be a result of a group-based exercise that could have caused more motivation for exercise regarding social interaction (Clarke & Coote, Reference Clarke and Coote2015). Recruitment involved participants only from one country region, so in further investigation, different country regions should be involved. Due to the nature of the disease, we could not make a total restriction of everyday physical activities nor regular physical therapy for individuals with MS. We didn’t measure the respiratory functions including spirometric (FVC, FEV1, FEV1/FVC), maximal inspiratory (MIP) and expiratory (MEP) mouth pressure measurements. In future investigations, it is necessary to perform breathing resistance exercises, e.g. by using a positive expiratory pressure (PEP) system.
Furthermore, this small sample size did not allow us to examine the complex relationships between psychological processes and insomnia disorder in MS, nor to explore the causal pathways between insomnia disorder comorbid to MS and psychological processes involved in the maintenance of insomnia. We also didn’t extensively assess physical symptoms related to MS (e.g. nocturia, spasticity, pain, etc.) that may negatively affect sleep and lead to chronic insomnia.
Conclusions
The present pilot randomized control trial provides novel, preliminary results that insomnia severity, fatigue and psychological distress, and daytime sleepiness may be reduced in persons with MS following 8-week combined UL-LL and breathing exercise intervention. Thus, these preliminary results are encouraging and warrant further investigation via a larger trial. Appropriate treatment of sleep disturbance, psychological distress, and fatigue is very important to reduce disability and provide a better QOL in patients with MS.
Acknowledgements
We want to thank the volunteers and the Multiple Sclerosis Society in Rijeka, Croatia, for the accomplished results, Dijana Ivanišević, BEcon for the assistance and support with recruiting participants.
Financial support
This work has been supported in part by the University of Rijeka (grant number: uniri-biomed-18-41).
Conflict of interest
Tanja Grubić Kezele has no conflicts of interest to disclose. Zrinka Trope has no conflicts of interest to disclose. Valentina Ahel has no conflicts of interest to disclose. Natali Ružić has no conflicts of interest to disclose. Hrvoje Omrčen has no conflicts of interest to disclose. Luka Đudarić has no conflicts of interest to disclose and Ariana Fužinac-Smojver has no conflicts of interest to disclose.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Trial registration
Name of the registry: Impact of Exercise on ‘Invisible’ Symptoms and Quality of Life in Multiple Sclerosis Individuals.
Registration: the study was registered at www.clinicaltrial.gov on October 1, 2018
First participant enrollment: December 07, 2018
URL: 003-08/18-01/05; TRIAL REGISTRATION ID: NCT03768830.





