



Inuit are Indigenous people residing primarily in Inuit Nunangat (homelands) in the Canadian Arctic. Diets of Inuit comprise a diverse range of traditional foods (typically called country foods (CF)), including marine and land mammals, fish, shellfish, birds, and local plants and berries(Reference Sharma, Hopping and Roache1). In the past several decades, however, Inuit have undergone a rapid dietary transition, characterised by a reduction of CF and rising consumption of a variety of market foods (MF), including an increasing amount of energy-dense and nutrient-poor products (also called non-nutrient dense foods (NNDF))(Reference Singer, Putulik Kidlapik and Martin2). This trend has translated into shifting intake patterns of various micro- and macronutrients, with wide-ranging potential implications for Inuit health(Reference Blanchet and Rochette3–Reference Gagne, Blanchet and Lauziere5). Indeed, the ongoing dietary transition has been paralleled by rising obesity and associated non-communicable diseases (e.g. cardiovascular disease, high cholesterol, high blood pressure and type 2 diabetes)(Reference Kellett, Poirier and Dewailly6). In the past decade, there has been growing research interest in this topic, with several overlapping studies examining the environmental, social and cultural determinants of the dietary transition and implications for food security and nutrition. Additionally, many studies have examined the continued importance of CF harvesting, preparation, sharing and consumption for food security and the cultural, spiritual, mental and physical health of Inuit(Reference Pufall, Jones and McEwen7,Reference Kuhnlein and Receveur8) . Finally, there exists a separate body of literature on the detrimental health impacts of exposure to environmental contaminants found in CF and weighing such concerns against the benefits of CF consumption(Reference Singh, Bjerregaard and Chan9). As of yet, there has been little effort to synthesise these disparate literatures and assess the drivers and wide-ranging health implications of the nutrition transition.
Considering this, a comprehensive and systematic literature review is needed to understand key patterns and identify gaps in the published literature on the complex interactions between environmental, social, economic, cultural and political factors and nutritional intake and health. This scoping review therefore aims to characterise the nature, range and extent of published research discussing the drivers and implications of the dietary transition in Inuit populations residing in Inuit Nunangat. By exploring and synthesising published literature, this review provides insight into the complex challenges influencing nutritional health among Inuit, which can inform research, decision-making and action on risk assessment, food policy and community food programmes.
Methods
Due to the complex and multidisciplinary nature of the literature on food, nutrition and nutrition-related health outcomes in the Canadian Arctic, we selected a scoping review approach, which is particularly suited to identify, examine and characterise the extent, nature and findings of research across diverse disciplines. Scoping reviews are particularly appropriate for mapping out research activities on a broad topic and are often used to compile and summarise emerging areas of research and to determine gaps in an existing body of knowledge(Reference Levac, Colquhoun and O’Brien10). This scoping review was guided by the work of Arksey and O’Malley(Reference Arksey and O’Malley11), Dijkers(Reference Dijkers12) and Levac and colleagues(Reference Levac, Colquhoun and O’Brien10). Methods and findings were reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews checklist(Reference Tricco, Lillie and Zarin13). The review protocol is available upon request.
Study selection
We conducted a literature search using PubMed, Web of Science (Web of Knowledge), CINAHL with Full Text (EBSCO), Academic Search Premier (EBSCO), Circumpolar Health Bibliographic Database and High North Research Documents. The search covered articles published up to 21 September 2019, limited to English language and available in an electronic format. Searches employed both controlled vocabularies, such as Medical Subject Headings, and keywords. The search strategy comprised three groups of search terms: geographic area or population (Canadian Arctic, Northern Canada, Inuit, Eskimo, Inuvialuit Settlement Region (ISR), Nunavut, Nunavik, Nunatsiavut and NunatuKavut), food consumption qualifiers (food, diet, nutrition, nutrient, hunt, harvest and contaminant) and health qualifiers (health, disease, infection, syndrome, wellness, well-being and malnutrition). No limiters were used, and search strategies were adapted for each database. A Science Citation Index (Web of Science) search strategy is presented in Box 1.
Box 1: Example search strategy to identify studies on the impacts of dietary change on nutrient intake and contaminant exposure in Canadian Arctic Inuit communities using Web of Science
TS = ((“Canadian Arctic” OR Inuit OR Eskim* OR “Northern Canada” OR Inuvialuit OR Nunavut OR Nunavik OR Nunatsiavut OR NunatuKavut)
AND TS = (Food* OR Diet* OR Contaminant* OR Nutrition* OR Nutrient* OR Hunt* OR Harvest*)
AND TS = (Health* OR Disease * OR Infect* OR Syndrome* OR Wellness OR Wellbeing OR Malnutrition)
Note: Eskim* captures references to Eskimo and Eskimeaux and is included as a search term to capture historical literature published over the last decades, although these terms are not considered acceptable by Inuit or contemporary academic communities.
Inclusion criteria
Population-based studies, reviews and reports of any design (including qualitative studies, prospective cohort studies, cross-sectional studies, intervention trials and systematic literature reviews) were included if they provided information relevant to food consumption, nutrient intake, dietary adequacy, dietary change, food security, nutrition-related chronic diseases or CF harvesting and consumption among Inuit populations residing in Inuit Nunangat. Inuit Nunangat refers to the homeland region of Inuit in present-day Canada, including ISR (Northwest Territories), Nunavut, Nunavik (northern Quebec), Nunatsiavut (northern Labrador) and NunatuKavut (southern Labrador)(14).
Exclusion criteria
Articles that were unavailable in full text were excluded. Studies focusing on in vitro or in vivo experiments were excluded. Additionally, studies that primarily reported on health impacts of contaminant exposure or zoonoses from CF sources were excluded, due to a number of recent reviews on this subject(Reference Singh, Bjerregaard and Chan9,15–Reference Van Oostdam, Donaldson and Feeley18) .
Screening process
Two independent reviewers (M.L. and H.H.) conducted the first screening stage, during which titles, abstracts and keywords of each article were screened for relevance using an eligibility form. The Kappa score for this stage was 0·81, indicating a strong level of agreement between reviewers(Reference McHugh19). Articles meeting the screening criteria proceeded to a second stage of screening, which entailed a full-text review conducted by two reviewers using a detailed screening form. The Kappa score for the full-text screening stage was 0·92, indicating an almost perfect level of agreement between reviewers(Reference McHugh19). Reviewers met throughout the screening process to resolve conflicts. For all included articles, reference lists were hand-searched for relevant titles that were not captured in the initial search. Relevant full-text articles proceeded to data extraction and analysis.
Data extraction and synthesis
Data were extracted by the two reviewers working independently. Any disagreements were resolved by consensus; if consensus was not reached, a third reviewer also conducted data extraction. The Kappa score for data extraction could not be calculated because both descriptive and qualitative (text) data were extracted from each article. Descriptive data items were extracted in DistillerSR (Evidence Partners), using a charting form designed for the purpose. Descriptive characteristics included study year, region of study, study design, analytical techniques, type of participants, sample size, exposures and outcomes assessed (if applicable), relevant measures of frequency (e.g. prevalence, incidence, dietary intake, if applicable) and associations (e.g. odds ratios and incidence rate ratios, if applicable). Following this, data were imported into Microsoft Excel (Microsoft Corporation) for analysis.
A thematic analysis was conducted on each full-text article using NVivo version 12.0 (QSR International), qualitative data analysis software. Thematic analysis is a method for identifying, analysing and reporting ‘themes’ in data(Reference Braun and Clarke20) and is often used in qualitative data sets; however, its usefulness for conducting systematic literature reviews and scoping reviews has recently been recognised(Reference Levac, Colquhoun and O’Brien10). We employed an inductive thematic analysis to derive initial codes (basic elements or segments of information) from each full-text article(Reference Boyatzis21), then merged codes into themes in an iterative process that identified and separated themes based on similarities, differences and depth of supporting data. Finally, we reviewed, defined, named and reported on themes(Reference Braun and Clarke20).
Results
Characteristics of included articles
The search strategy identified 3301 articles and 1824 articles after deduplication. A total of 162 peer-reviewed articles, government publications and organisational reports met all the inclusion and exclusion criteria and were included in the literature review (Fig. 1). Articles are presented by year in Fig. 2; of the 162 articles, the largest proportion was published in 2010, with a decreasing trend in recent years. Research conducted in multiple regions of Inuit Nunangat was most common (30 %), followed by Nunavik (25 %), Nunavut (28 %) and ISR (10 %) (Fig. 3). Cross-sectional epidemiological studies (73 %) and qualitative studies (10 %) comprised the majority of the articles, followed by literature reviews (e.g. systematic reviews and scoping reviews) (6 %) and studies on interventions (e.g. community-based food programmes and policies) (4 %) (Fig. 4).
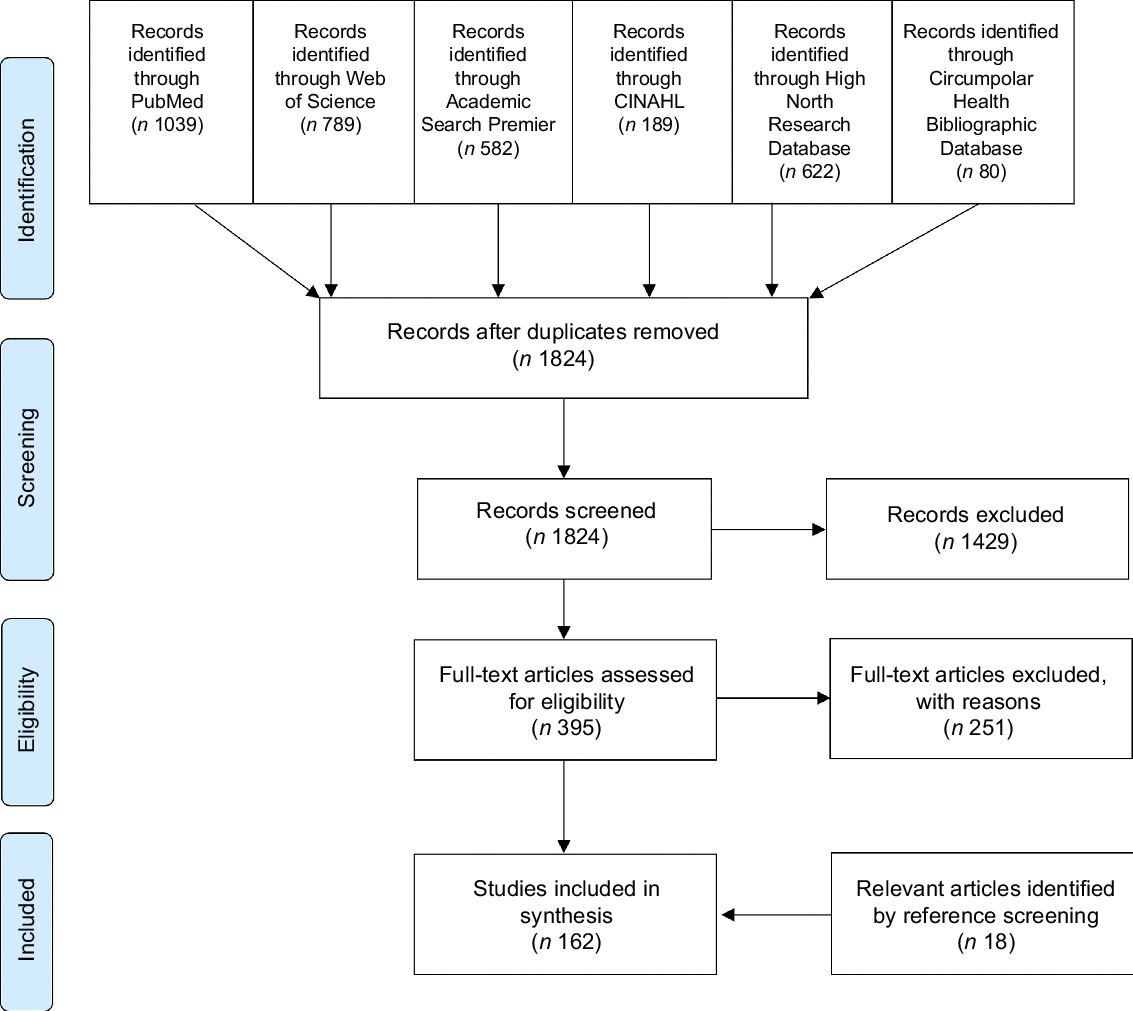
Fig. 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting flow diagram showing four-stage article selection process used to identify articles on drivers and health implications of the dietary transition among Inuit in the Canadian Arctic
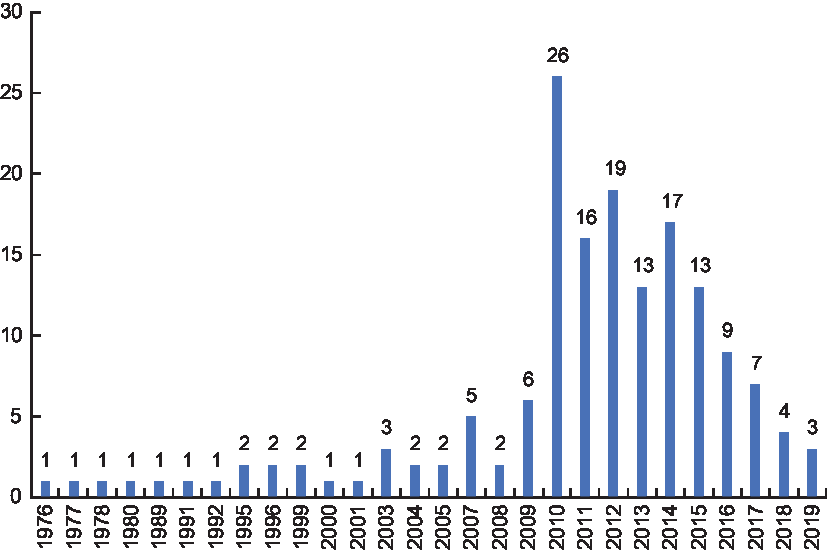
Fig. 2 Number of relevant articles discussing drivers and implications of the dietary transition in the Canadian Arctic by year of publication (n 162)
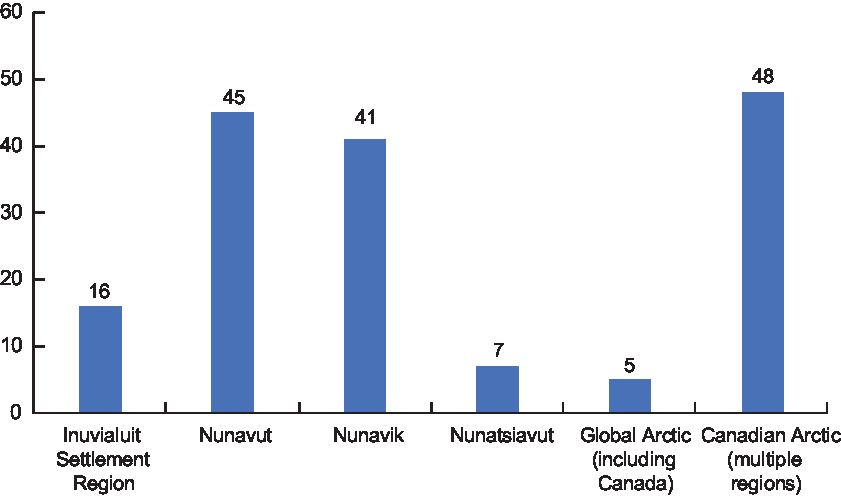
Fig. 3 Number of articles by region on drivers and health implications of the dietary transition among Inuit in the Canadian Arctic (n 162)
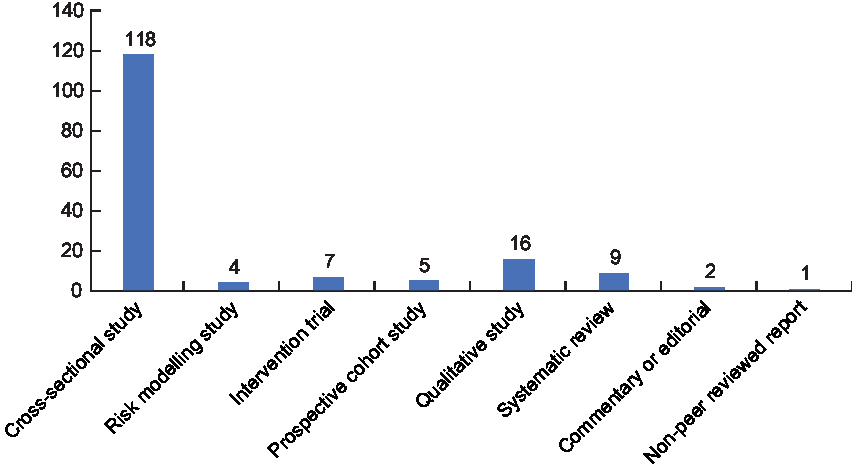
Fig. 4 Number of articles by study type on drivers and health implications of the dietary transition among Inuit in the Canadian Arctic (n 162)
Themes identified in the literature
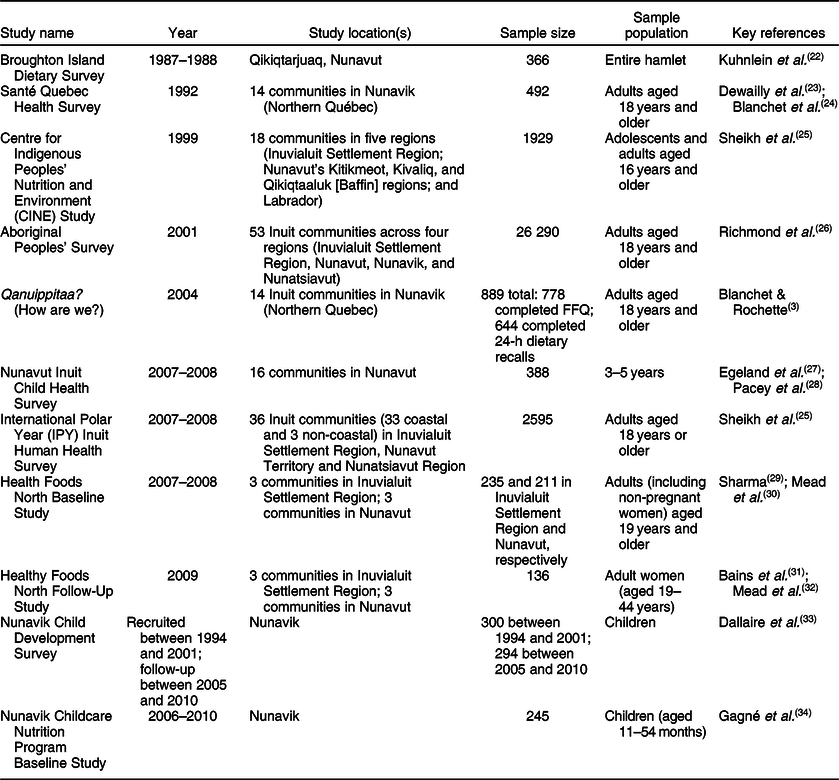
Articles were grouped broadly by primary topic (Fig. 5). A large proportion (65 %) of articles described dietary intake and adequacy and assessed nutrition-related health outcomes and biomarkers. Lesser proportions of articles examined food security (11 %), food-related programmes and policies (9 %), impacts of climate change on food access (4 %) and risk-benefit trade-offs of CF and MF consumption (4 %). Notably, while many articles mentioned the socio-cultural importance and implications of CF consumption, few articles examined this as a primary topic (5 %). Few articles examined food environments and determinants of dietary choices (2 %). Many articles used data from the same studies, the most common of which are presented in Table 1. Several themes were identified in the thematic analysis and will be described in detail in the following sections.
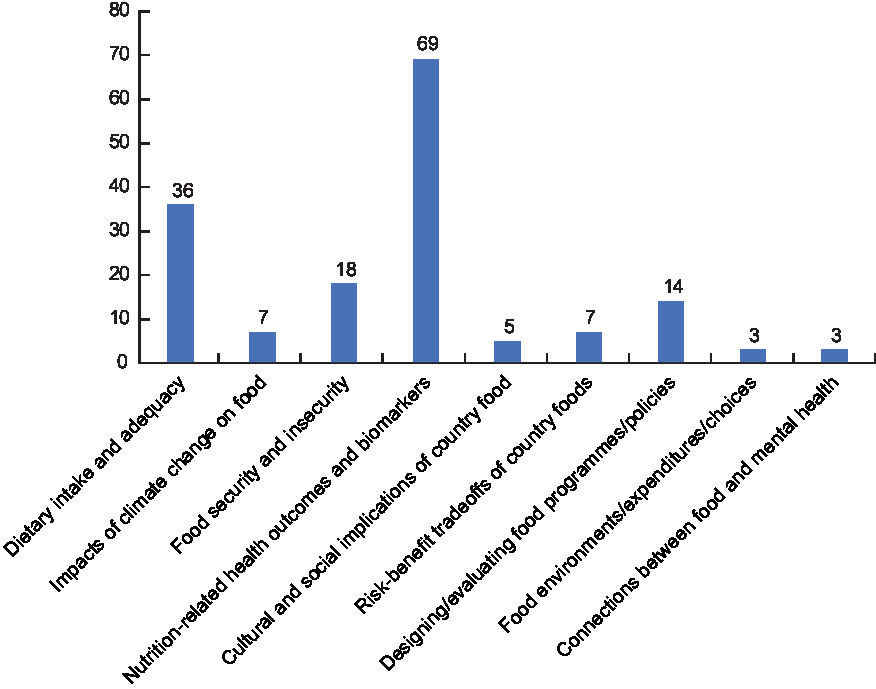
Fig. 5 Number of articles by topic included in scoping review on drivers and health implications of the dietary transition among Inuit in the Canadian Arctic
Table 1. Identification and characteristics of major studies conducted with Inuit populations in the Canadian Arctic since 1987
Description of dietary trends
Prior to colonial contact, the diets of Inuit consisted entirely of CF acquired from land-based harvesting. Dietary staples included land mammals (e.g. caribou, muskox and polar bear), marine mammals (e.g. seal, whale and walrus), fish (e.g. Arctic char, brook trout, lake whitefish and lake trout), shellfish (e.g. mussels, clams and oysters), wildfowl (geese, ptarmigan, marine birds and eggs) and plant-based foods (e.g. seaweed and berries)(Reference Sharma, Hopping and Roache1,Reference Gagne, Blanchet and Lauziere5,Reference Sharma29) . Overall, while longitudinal data are sparse, the literature suggests that CF consumption has declined rapidly in the last several decades (Table S1), in many cases replaced by purchased NNDF (defined as high-fat and/or high-sugar foods). Published data do not precede 1969, but surveys from the late 1960s and 1970s suggest that CF comprised approximately half of all consumed foods during those decades(Reference Mayhall35–Reference Ellestad-Sayed, Haworth and Hildes37). As recently as 1987, CF still provided between up to one-half (46·5 %) of the total energy intake (TEI: measured as energies consumed) of Inuit in Qikiqtarjuaq (Nunavut), depending on the age group(Reference Kenny, Hu and Kuhnlein38–Reference Kuhnlein, Soueida and Receveur40). Successive surveys in ISR, Nunavut and Nunavik have found that TEI contributions from CF declined from 21 to 28 % in the 1990s to between 14 and 16 % in studies conducted between 2004 and 2008(Reference Blanchet and Rochette3,Reference Sheikh, Egeland and Johnson-Down25,Reference Proust, Lucas and Dewailly41–44) . In Nunatsiavut, while historical data are sparse, a study conducted in 2014–2015 in three communities suggested that CF comprised, on average, only 2 % of TEI(Reference Calder, Bromage and Sunderland45).
Conversely, the percentage of energy intake from MF, including NNDF, has increased steadily. Currently, NNDF are consumed much more frequently than CF, contributing between 25 and 51 % of TEI, depending on region and age group(Reference Mayhall35,Reference Kenny, Hu and Kuhnlein38,Reference Kuhnlein39,Reference Proust, Lucas and Dewailly41–Reference Zotor, Sheehy and Lupu50) . Meanwhile, consumption of nutrient-dense MF (e.g. fruits and vegetables) is reported to be low(Reference Proust, Lucas and Dewailly41,Reference Mead, Gittelsohn and De Roose49,Reference Hopping, Erber and Mead51,Reference Hopping, Mead and Erber52) . Of particular concern is the increased popularity of foods high in simple carbohydrates. Indeed, the percentage of energy intake from sweetened beverages (e.g. carbonated and powdered drinks, coffee and tea with added sugar) and high-carbohydrate foods (e.g. bread, pasta and bannock) increased substantially between the late 1980s and 2008 and now contributes over 20 % of TEI, on average(Reference Sheikh, Egeland and Johnson-Down25,Reference Kenny, Hu and Kuhnlein38,Reference Kuhnlein, Soueida and Receveur40,Reference Sharma, De Roose and Cao43,44,Reference Sheehy, Roache and Sharma46–Reference Zotor, Sheehy and Lupu50) . In 2007–2008, the International Polar Year (IPY) Inuit Health Survey reported that the top ten contributors to TEI were mostly NNDF, including candy, processed meats, chips, white bread and pizza(Reference Kenny, Hu and Kuhnlein38).
Reviewed literature reported that dietary patterns differed according to demographic factors. Women reported consuming less CF than men across all age groups in all Arctic regions, dating back to surveys in the 1980s(Reference Sheikh, Egeland and Johnson-Down25,Reference Kuhnlein, Soueida and Receveur40) . Irrespective of gender, CF intake increased with age across all dietary studies(Reference Gagne, Blanchet and Lauziere5,Reference Blanchet, Dewailly and Ayotte24,Reference Mayhall35,Reference Mayhall36,Reference Berti, Hamilton and Receveur53) and youth and young adults consistently consumed fewer CF and more MF than their parents(Reference Singer, Putulik Kidlapik and Martin2,Reference Gagne, Blanchet and Lauziere5,Reference Dewailly, Blanchet and Lemieux23–Reference Sheikh, Egeland and Johnson-Down25,Reference Kuhnlein, Soueida and Receveur40,Reference Proust, Lucas and Dewailly41,Reference Galloway, Johnson-Down and Egeland54) . Recently, the IPY Inuit Health Survey found that adults aged 41–60 years consumed almost double the proportion of CF compared to younger adults(Reference Kuhnlein, Receveur and Soueida55). Several studies reported that households with children consumed more MF than households without children(Reference Egeland, Pacey and Cao27,Reference Huet, Ford and Edge56,Reference Rosol, Huet and Wood57) . However, households with children also consumed more fruits and vegetables(Reference Egeland, Pacey and Cao27,Reference Huet, Ford and Edge56,Reference Rosol, Huet and Wood57) , perhaps partially offsetting nutrients lost from low consumption of CF. Studies conducted in Nunavut and Nunavik indicated that participation in traditional activities, such as hunting, increases from youth to adulthood, with potential impacts on CF access and consumption(Reference Condon, Collings and Wenzel58). A paucity of longitudinal data limits our ability to determine whether and how much CF intake changes as one ages. It is likely that dietary changes occur across generations as well as over the life course of individuals, creating challenges to interpreting overall time trends in average intake of CF and MF(Reference Blanchet, Dewailly and Ayotte24).
Determinants of dietary transitions, dietary intake and food security
Articles described a number of complex mechanisms and processes that have affected dietary patterns among Inuit and driven the transition from CF to MF(Reference Akande, Hendriks and Ruiter59,Reference Kuhnlein60) . Colonial economic and political factors, cultural food preferences, harvesting practices and climate change have interacted to drive dietary changes across Inuit Nunangat.
Historical, colonial and economic factors
Historical and ongoing colonial processes have had wide-ranging impacts on Inuit sovereignty, cultural practices and social structures, impacting food access and consumption in a number of ways(Reference Mead, Gittelsohn and Kratzmann65). Several authors emphasised the integral importance of harvesting, sharing and consuming CF to Inuit traditions, culture, identity, health and well-being(Reference Pufall, Jones and McEwen7,Reference Kuhnlein and Receveur8,Reference Kuhnlein, Receveur and Soueida22,Reference Ford, Lardeau and Blackett61–Reference Mead, Gittelsohn and Kratzmann65) . Qualitative studies have documented the importance of CF in connecting Inuit with surrounding lands, community and family(Reference Pufall, Jones and McEwen7,Reference Ford, Lardeau and Blackett61) . Changes to household and social structures following the establishment and growth of Inuit communities have contributed to disruptions in CF sharing networks, resulting in reductions in some food sharing practices(Reference Counil, Gauthier and Blouin66,Reference King and Furgal67) . Schooling and employment have restricted the time available for collecting food from the land(Reference Counil, Gauthier and Blouin66–70). Meanwhile, wildlife management structures have established and enforced harvest restrictions and harvest bans on certain animal populations (e.g. beluga and caribou), thereby limiting their accessibility for Inuit hunters(Reference Kuhnlein60,Reference Martin68,Reference Kenny, Fillion and Simpkin71–Reference Pearce, Ford and Caron73) . Some authors identified and discussed the cyclical nature of knowledge loss, in which reductions in hunting, preparing and consuming CF limit the intergenerational transfer of traditional knowledge, causing further reductions in CF consumption(Reference Mead, Gittelsohn and Kratzmann65,Reference King and Furgal67,Reference Pearce, Ford and Caron73) . Elders in northern communities have expressed particular concern that youth are spending less time conducting subsistence activities, thus poorly equipping them to participate in CF harvest and preparation(Reference Pufall, Jones and McEwen7,Reference Martin68,Reference Pearce, Ford and Caron73) .
Over time, transport infrastructure and retail stores have provided increased availability of MF. In addition, MF have become increasingly acceptable and desirable as a result of advertising and social exchange with non-Indigenous people(Reference Kuhnlein60). Meanwhile, CF have not yet been consistently integrated into the market economy in most regions, perhaps due to the cultural incongruity of exchanging money for foods that were traditionally shared(Reference Ford, Lardeau and Blackett61,Reference Ford, Macdonald and Huet74) . When CF are available for purchase (often through the online informal economy), they tend to be costly(Reference Ford, Lardeau and Blackett61,Reference Ford, Macdonald and Huet74) . Moreover, nutrient-dense MF (e.g. fresh vegetables and fruit) are often unavailable, expensive or poor quality in remote Arctic communities due to logistical challenges (e.g. weather disruptions) and extreme temperatures during transport(Reference Sheehy, Kolahdooz and Schaefer75). In many communities, limited competition among food retailers has been reported to further exacerbate high food prices(Reference Sheehy, Kolahdooz and Schaefer75). Damaged or spoiled products past their best-before dates were commonly reported in northern stores, creating a reliance on less expensive, non-perishable processed foods that are usually non-nutrient dense(Reference Richmond26,Reference Ford, Lardeau and Blackett61,Reference Sheehy, Kolahdooz and Schaefer75–Reference Kolahdooz, Pakseresht and Mead77) .
Financial challenges and low socio-economic status were often cited as barriers to accessing CF and healthy MF. Increased dependence on modern equipment for CF harvesting (e.g. vehicles, fuel, firearms and ammunition), combined with their high cost in northern communities, creates significant challenges to harvesting CF(Reference Hopping, Erber and Mead51,Reference Galloway, Johnson-Down and Egeland54,Reference Mead, Gittelsohn and Kratzmann65,Reference King and Furgal67,Reference Organ, Castleden and Furgal78–Reference Ford, Lardeau and Vanderbilt80) . Studies across the Arctic found that a number of indicators of socio-economic status (e.g. low education, unemployment, household crowding, receiving social assistance, public housing and having a home in need of major repairs) were associated with food insecurity and lower consumption of CF and fruits and vegetables(Reference Erber, Hopping and Beck48,Reference Hopping, Mead and Erber52,Reference Akande, Hendriks and Ruiter59,Reference Beaumier and Ford81–Reference Ruiz-Castell, Muckle and Dewailly85) . Successive studies in Nunavut found that availability and affordability of foods, high cost of harvesting CF, limited budgeting skills and unfamiliarity with nutritional content of different MF were driving food choices towards NNDF(Reference Beaumier and Ford81,Reference Ford and Beaumier82,Reference Lardeau, Healey and Ford86) .
Food preferences, perceptions and knowledge
Several studies reported on food preferences, perceptions and knowledge. A qualitative study conducted with Inuit living in south-east Labrador discussed the changing relationship that Inuit have with their food. This study confirms that individuals have had to rapidly adapt from a food environment replete with locally harvested CF to one with many food choices, including newer MF. As argued by the authors, these rapid changes in food availability limited the ability of Inuit to rely on traditional nutrition and food preparation knowledge and have forced individuals to ‘re-learn’ how and what to eat(Reference Martin68).
Importantly, many Inuit maintain a desire to consume CF. Several surveys conducted with Inuit reported that the majority of respondents preferred a mixture of CF and MF and expressed a desire to eat more CF than they currently consume(Reference Galloway, Johnson-Down and Egeland54,Reference Ford, Lardeau and Blackett61,Reference Egeland, Faraj and Osborne87) . CF were viewed as healthier than MF, and some Inuit reported feeling ‘lazy’, ‘tired’ and ‘unfulfilled’ when they do not eat CF(Reference Pufall, Jones and McEwen7,Reference Gittelsohn, Roache and Kratzmann62,Reference Sheppard and Hetherington88) . MF were often perceived as being of inferior quality, being described as ‘sugary’, ‘junk’ or ‘garbage’(Reference Harper, Edge and Ford63). However, due to availability, convenience, affordability, advertising and palatability, food preferences may be shifting towards MF, particularly among young people. In interviews, some Inuit describe the difficulties of having children who only crave junk food, and how this was often the least expensive option to feed them(Reference Pufall, Jones and McEwen7,Reference Ford, Lardeau and Blackett61) . Risk perception was an important challenge; semi-structured interviews with Inuit adults in Nunavik revealed that 33 % of individuals were worried about environmental contaminants in CF and intentionally limited their consumption of foods they viewed as ‘high-risk’(Reference Mead, Gittelsohn and Kratzmann65).
As Inuit transition from CF to MF, a number of factors may act as barriers to the acceptability of nutrient-dense MF (e.g. fruits and vegetables) and drive food choices towards NNDF. The introduction of improved means of communication (television and, more recently, internet) has increased exposure to food marketing, likely contributing to shifting food preferences, particularly among young people(Reference Ford, Lardeau and Blackett61). An ethnographic study conducted in Iqaluit, Nunavut suggested that easy-to-eat products such as store-bought snack foods may be popular since they align with the traditional practices of food sharing, eating ‘on-the-go’ while hunting or fishing, and eating when one is hungry instead of structured meals(Reference Counil, Julien and Lamarche89,Reference Searles90) . Household crowding and financial insecurity may also influence food purchasing and eating behaviours by forcing families to make more frequent, smaller grocery purchases(Reference Searles90). Further, limited culinary knowledge of preparation methods for perishable MF may reduce their acceptability among Inuit households and encourage consumption of more convenient non-nutrient dense MF dishes(Reference Pakseresht, Lang and Rittmueller84).
Climate change
Dietary changes have been exacerbated by climate change, which has disrupted CF harvest practices by altering migration patterns of animals (birds, land mammals and marine mammals), intensifying animal population declines(Reference Kenny, Fillion and Simpkin71) and reducing the predictability of weather and travel conditions, thus impacting the navigability of traditional hunting grounds (e.g. by altering water levels, snow pack and sea ice)(Reference Galloway, Johnson-Down and Egeland54,Reference Harper, Edge and Ford63,70,Reference Pearce, Ford and Caron73,Reference Goldhar, Bell and Wolf79,Reference Beaumier and Ford81,Reference Ford and Beaumier82,Reference Cunsolo Willox, Harper and Ford91–Reference Wesche and Chan95) . In Nunavut, hunters have reported lower water levels in ponds and rivers along the coastline, resulting in reduced access to fish and birds(Reference Nancarrow and Chan93). Snowfall has become more variable, driving a shift in migration patterns of caribou across Inuit Nunangat(Reference Harper, Edge and Ford63,Reference Nancarrow and Chan93) . Availability of berries was reported to have declined across the Arctic due to changing weather patterns and invasive plant species(Reference Harper, Edge and Ford63,Reference Nancarrow and Chan93) . Inuit have described reductions in sea ice extent, thickness, quality and duration, limiting access to traditional hunting areas and increasing the danger and difficulty associated with harvesting marine CF(Reference Harper, Edge and Ford63,Reference Beaumier and Ford81,Reference Ford and Beaumier82,Reference Nancarrow and Chan93) . Other climate-induced changes reported by hunters include ‘paler’ flesh in Arctic char (possibly indicative of a changing diet), less fat on ringed seals (resulting in less buoyancy and a higher proportion of lost seals) and increased parasites in caribou meat(Reference Nancarrow and Chan93). Changes in predator-prey balance have also been reported by hunters; for example, increased killer whale (orca), polar bear, narwhal and bowhead whale populations in Repulse Bay have reportedly driven beluga populations away from the community(Reference Nancarrow and Chan93). Climate change has also affected CF safety. In Nunatsiavut, Inuit residents have reported that the sun’s heat has intensified in recent years, at times spoiling meat during harvest and increasing the risk of parasites, pathogens and toxins (e.g. botulinum toxin) in CF preparations(Reference Harper, Edge and Ford63,Reference Nancarrow and Chan93,Reference Parkinson and Butler96) . Collectively, these climate-induced phenomena challenge skilled harvesters and reduce their capacity to harvest, share and prepare CF(Reference Akande, Hendriks and Ruiter59,Reference Harper, Edge and Ford63,Reference Wesche and Chan95) .
Possible impacts of the dietary transition on health outcomes
Despite declining intake, it is important to note that CF remain a very important source of energy and nutrients and often contribute up to half of overall protein and Fe and over 70 % of overall n-3 polyunsaturated fatty acid (PUFA) intake(Reference Egeland, Johnson-Down and Cao4,Reference Sharma, Cao and Roache42,Reference Calder, Bromage and Sunderland45,Reference Kuhnlein60,Reference Kenny, Fillion and Simpkin71,Reference Schaefer, Erber and Trzaskos97) . Indeed, individuals that regularly consume CF have significantly higher intakes of energy, percentage of energy from protein and protein-related micronutrients, fibre, Ca, n-3 PUFA, riboflavin, niacin, Fe, Zn, Cu, Mg, K, selenium (Se), vitamins A, B6, B12, C, D and E and a lower intake of carbohydrates, saturated fat and Na(Reference Egeland, Johnson-Down and Cao4,Reference Gagne, Blanchet and Lauziere5,Reference Dewailly, Blanchet and Lemieux23,Reference Sharma29,Reference Kuhnlein, Soueida and Receveur40,Reference Calder, Bromage and Sunderland45,Reference Berti, Hamilton and Receveur53,Reference Kuhnlein, Receveur and Soueida55,Reference Kuhnlein60,Reference Sheehy, Kolahdooz and Roache69,Reference Jamieson, Kuhnlein and Weiler98–Reference Lemire, Kwan and Laouan-Sidi100) .
However, the dietary transition from primarily CF to primarily MF (including a large proportion of NNDF) has implications for nutrient intakes, food security and health (including nutritional, cardiometabolic, oral, socio-cultural and psychological health). No studies conducted with Inuit populations in the Canadian Arctic have directly assessed the impacts of dietary change using longitudinal data; however, successive cross-sectional studies provide insight into the shifting food security and health burdens that parallel the dietary transition.
Food insecurity and dietary adequacy
Cross-sectional studies in Inuit Nunangat employed different questionnaires and classifications of food security, leading to inconsistent figures; however, it is well recognised that Inuit disproportionately suffer from food insecurity, nutrient deficiencies and poor dietary adequacy compared with the rest of Canada. Overall, across Inuit Nunangat, 62·6 % of Inuit households are food insecure, with 27·2 % being severely food insecure(Reference Huet, Rosol and Egeland83). Consistently high localised prevalence of household food insecurity was reported in Nunavut (68·8 %), ISR (43·3 %), Nunatsiavut (45·7 %) and Nunavik (49·7 %)(Reference Rosol, Huet and Wood57,Reference Huet, Rosol and Egeland83,Reference Findlay, Langlois and Kohen101–Reference Guo, Berrang-Ford and Ford106) . While food retail subsidy initiatives, such as Nutrition North Canada (NNC), exist to support healthy MF transport to Inuit communities, data suggest that food insecurity has increased in many regions (including Nunavut) over the past decade despite such subsidies(Reference St-Germain, Galloway and Tarasuk104).
Food insecurity and reduced CF consumption may combine to produce dietary inadequacies and nutrient deficiencies across Inuit communities(Reference Berti, Hamilton and Receveur53,107–Reference Waiters, Godel and Basu116) . Studies reporting on dietary adequacy suggested that consumption of micronutrients (e.g. Ca and folate), essential vitamins (vitamins A, C, D and E) and fibre was significantly lower than recommended levels in ISR(Reference Kenny, Hu and Kuhnlein38) and Nunavut among adults(Reference Sharma, Cao and Roache42) and children(Reference Berti, Soueida and Kuhnlein108,Reference El Hayek Fares and Weiler111,Reference El Hayek, Egeland and Weiler112) (Table S5). Other assessments in Inuit adults confirmed that dietary fibre, Ca, folate, Mg, and K and vitamins A and E (and vitamin D among women) were below recommended intake in 50–100 % of participants, and deficiency was often associated with food insecurity(Reference Dallaire, Dewailly and Shademani33,Reference Erber, Hopping and Beck48,Reference Hopping, Mead and Erber52,Reference Schaefer, Erber and Trzaskos97,Reference Kolahdooz, Barr and Roache99,Reference Berti, Soueida and Kuhnlein108–Reference Egeland, Berti and Soueida110,Reference Johnson-Down and Egeland113–Reference Rittmueller, Corriveau and Sharma115) . Another contributing factor to poor dietary adequacy may be limited intake of fruits and vegetables, likely due to poor access, poor quality and high prices, as described above(Reference Zotor, Sheehy and Lupu50,Reference Hopping, Mead and Erber52,Reference Johnson-Down and Egeland113) .
Iron deficiency and anaemia
Iron deficiency and anaemia are substantial public health concerns among Inuit, despite frequent consumption of foods high in bioavailable iron, including traditional meats(Reference Jamieson and Kuhnlein117). Most studies have found that dietary adequacy of iron is sufficient; indeed, between 91 and 100% of Inuit consume more than the estimated average requirement of iron(Reference Kuhnlein, Receveur and Soueida55). However, prevalence of clinical iron deficiency (based on serum ferritin) is high in Inuit communities, with figures between 20·4 and 35·6 %(Reference Jamieson, Kuhnlein and Weiler98,Reference Christofides, Schauer and Zlotkin118–Reference Zhou, Kubow and Egeland120) among women and 18 and 33% among children(Reference Pirkle, Lucas and Dallaire102,Reference Pacey, Weiler and Egeland121) (Table S2). Overall prevalence estimates of anaemia were similarly high, with studies determining figures between 22 and 43 %(Reference Jamieson, Kuhnlein and Weiler98,Reference Christofides, Schauer and Zlotkin118,Reference Zhou, Kubow and Egeland120) among women, 13 and 17% among children(Reference Pirkle, Lucas and Dallaire102,Reference Pacey, Weiler and Egeland121,Reference Egeland, Williamson-Bathory and Johnson-Down122) , and 16% among men(Reference Jamieson, Weiler and Kuhnlein123,Reference Jamieson, Weiler and Kuhnlein124) . Determinants of low serum ferritin, iron deficiency, depleted iron stores, low Hb and/or anaemia included infection with H. pylori (Reference Jamieson, Kuhnlein and Weiler98,Reference Christofides, Schauer and Zlotkin118,Reference Jamieson, Weiler and Kuhnlein123) , food insecurity(Reference Egeland, Johnson-Down and Cao4,Reference Jamieson, Kuhnlein and Weiler98,Reference Jamieson, Weiler and Kuhnlein123) , not having a hunter in the home(Reference Jamieson, Weiler and Kuhnlein123,Reference Jamieson, Weiler and Kuhnlein124) , low frequency of sea mammal consumption(Reference Jamieson, Kuhnlein and Weiler98) and decreased red blood cell PUFA status(Reference Jamieson, Kuhnlein and Weiler98). Due to the co-existence of high meat consumption with anaemia, Jamieson and Kuhnlein argued that iron deficiency anaemia likely does not constitute the majority of anaemia cases in the Arctic and that other underlying nutritional deficiencies (e.g. vitamins A, E, C, riboflavin and folate), as well as active infections, parasitosis and gastrointestinal H. pylori colonisation, must be considered important determinants(Reference Jamieson and Kuhnlein117).
Cardiometabolic health
Until recently, obesity and related cardiometabolic health outcomes (including type 2 diabetes (T2D), hypertension, hypercholesterolaemia and CVD) were uncommon among Inuit(Reference Schaefer, Timmermans and Eaton140,Reference Thouez, Rannou and Foggin141) . Several researchers attributed this to their elevated consumption of marine foods, which are rich in cardioprotective n-3 PUFA and Se(Reference Laird, Goncharov and Egeland17,Reference Proust, Lucas and Dewailly41,Reference Lemire, Kwan and Laouan-Sidi100,Reference Blanchet, Lauziere and Gagne125–Reference Valera, Dewailly and Anassour-Laouan-Sidi139) . Yet, obesity and related health outcomes are becoming more common, likely in part due to reduced n-3 PUFA consumption and increased intake of NNDF high in sodium, sugar and unhealthy fats (Table S3)(Reference Kuhnlein, Receveur and Soueida22,Reference Proust, Lucas and Dewailly41,Reference Lucas, Proust and Blanchet130,Reference Galloway, Young and Egeland142,Reference Hopping, Erber and Beck143) . Estimates from surveys conducted between 2004 and 2008 suggest that combined overweight and obesity affects between 52 and 63 % of Inuit(Reference Kellett, Poirier and Dewailly6,Reference Egeland, Cao and Young147) and is particularly prevalent among women(Reference Singer, Putulik Kidlapik and Martin2,Reference Kuhnlein, Receveur and Soueida22,Reference Zotor, Sheehy and Lupu50,Reference Charbonneau-Roberts and Young144–Reference Hopping, Erber and Mead146) . Smaller scale studies have also reported high prevalence of childhood overweight and obesity in recent years(Reference Singer, Putulik Kidlapik and Martin2,Reference Galloway, Young and Egeland142,Reference Panagiotopoulos, Nguyen and Smith148,Reference Medehouenou, Ayotte and St-Jean149) . Dietary determinants of at-risk body mass index (BMI), overweight and obesity included food insecurity(Reference Egeland, Pacey and Cao27,Reference Zienczuk and Egeland150) , high-sugar drink consumption(Reference Zienczuk, Young and Cao151) and low physical activity(Reference Huet, Rosol and Egeland83,Reference Zienczuk, Young and Cao151,Reference Kolahdooz, Mathe and Katunga152) . The Nunavut Inuit Child Health Survey (2007–2008) was unable to establish a relationship between obesity and consumption of MF or food insecurity among children aged 3–5 years, suggesting that non-dietary factors may be driving childhood obesity(Reference Egeland, Pacey and Cao27,Reference Johnson-Down and Egeland113,Reference Galloway, Young and Egeland142) .
BMI, waist:hip ratio, waist circumference and overweight/obesity were associated with a number of adverse cardiometabolic health outcomes in health surveys conducted across Inuit communities, including hypertension(Reference Chateau-Degat, Dewailly and Noël153), unfavourable lipid profiles(Reference Château-Degat, Dewailly and Charbonneau154), metabolic syndrome(Reference Chateau-Degat, Dewailly and Noël153), insulin resistance(Reference Chateau-Degat, Dewailly and Noël153), fasting glycaemia(Reference Singer, Putulik Kidlapik and Martin2,Reference Egeland, Cao and Young147) , type 2 diabetes(Reference Egeland, Cao and Young147) and CVD(Reference Ronn, Lucas and Laouan Sidi155). However, some studies reported that obesity has fewer cardiometabolic health impacts among Inuit when compared with other Canadians. Indeed, Inuit have lower fasting glucose, triacylglyceride levels, cholesterol, blood pressure and lower prevalence of T2D for a given BMI or waist circumference when compared with Canadians of European ancestry(Reference Kellett, Poirier and Dewailly6,Reference Chateau-Degat, Dannenbaum and Egeland156–Reference Young, Bjerregaard and Dewailly158) . It has been suggested that long-term adaptation to Arctic cold favours deposition of abdominal fat, thus higher BMI in Inuit may be a natural adaptive evolution to a colder environment(Reference Noel, Dewailly and Chateau-Degat159). Such hypotheses would support the establishment of different BMI, waist:hip ratio and waist circumference risk thresholds for Inuit when compared with Euro-Canadians(Reference Chateau-Degat, Dannenbaum and Egeland156,Reference Noel, Dewailly and Chateau-Degat159) .
Despite this, adverse cardiometabolic health outcomes have been steadily increasing in recent years to parallel rises in overweight and obesity. Successive cross-sectional studies across the Arctic have shown increasing trends in the prevalence of glucose intolerance and T2D (Table S4), although the general T2D burden remains lower than in other Indigenous populations in Canada(Reference Singer, Putulik Kidlapik and Martin2,Reference Pakseresht, Lang and Rittmueller84,Reference Charbonneau-Roberts and Young144,Reference Chateau-Degat, Dewailly and Louchini145,Reference Egeland, Cao and Young147,Reference Healey and Meadows157,Reference Erber, Beck and De Roose160–Reference Sefidbakht, Johnson-Down and Young163) . However, among certain Inuit sub-populations (e.g. elderly females), age-standardised prevalence of T2D may exceed Canadian reference values(Reference Hu, Singh and Kenny164). Few studies reported associations between dietary intake and measures of glucose intolerance or T2D(Reference Singer, Putulik Kidlapik and Martin2,Reference Sefidbakht, Johnson-Down and Young163) . Singer and colleagues(Reference Singer, Putulik Kidlapik and Martin2) reported that individuals who spent less time on the land had lower odds of T2D, which may be indicative of the protective effects of physical activity and diets high in CF.
Meanwhile, cardiovascular risk factors (hypertension, hypercholesteraemia and poor blood lipid profiles) are also becoming more prevalent among Inuit. Subsequent cross-sectional studies conducted in Nunavik showed that hypertension doubled among adults between 1994 and 2004 from 9 to 19 %(Reference Chateau-Degat, Dewailly and Louchini145) and is currently above 25 % across other regions of the Arctic(Reference Erber, Beck and De Roose160). Hypercholesterolaemia and poor blood lipid profiles are increasingly common, likely due to a combination of (and interactions between) genetic, dietary and lifestyle traits(Reference Chateau-Degat, Dewailly and Louchini145,Reference Egeland, Cao and Young147,Reference Labonte, Dewailly and Lucas165–Reference Rudkowska, Ouellette and Dewailly167) . Further, several CVD (stroke, cerebrovascular diseases and ischemic heart disease), once absent in Inuit populations, are now reaching burdens similar to the Canadian general population(Reference Chateau-Degat, Dewailly and Louchini145,Reference Hu, Singh and Kenny164) .
While measures of overweight and obesity were consistently associated with poorer cardiometabolic health, few studies examined dietary risk factors associated with hypertension, poor lipid profiles and CVD among Inuit populations(Reference Ronn, Lucas and Laouan Sidi155). Dietary sodium intake was highly correlated with blood pressure and hypertension in Nunavik(Reference Chateau-Degat, Ferland and Déry168), which may indicate that MF consumption is associated with adverse cardiometabolic outcomes. While several authors speculated that dietary factors may be responsible for increasing prevalence of CVD(Reference Counil, Julien and Lamarche89,Reference Dewailly, Blanchet and Gingras169) , only one study was able to establish associations between dietary patterns and CVD health outcomes(Reference Hu, Kenny and Chan170). Using principal component analysis to derive profiles of food consumption, Hu and colleagues(Reference Hu, Kenny and Chan170) identified three dietary patterns (‘market food’, ‘country food – fat’ and ‘country food – fish’) and found that the ‘market food’ diet was associated with elevated prevalence of coronary heart disease (CHD) and myocardial infarction(Reference Hu, Kenny and Chan170). Meanwhile, the ‘country food – fish’ diet (characterised by high fish consumption and low sugar and sweets intake) was inversely associated with the prevalence of CHD, myocardial infarction, stroke and hyperlipidaemia(Reference Hu, Kenny and Chan170).
Psychological, social and mental health outcomes
Traditional practices of harvesting, sharing and consuming CF have been linked to improved mental and social health outcomes(Reference King and Furgal67,Reference Richmond and Ross184) . Three studies indicate that higher n-3 PUFA status (which are abundant in marine CF) is protective against psychological distress(Reference Lucas, Dewailly and Blanchet134,Reference Lucas, Kirmayer and Dery136,Reference Skogli, Geoffroy and Weiler138) . In a study assessing individual- and community-level determinants of Inuit youth mental wellness in Nunavik, Gray and colleagues found that a strong relationship to the land, including harvesting, processing, sharing and consuming CF, was associated with better mental wellness and lower suicidal ideation(Reference Gray, Richer and Harper185). At the community level, they also observed lower suicidality rates in communities where more CF were harvested, processed and shared(Reference Gray, Richer and Harper185). These results aligned with another study by Fraser and colleagues, who found that participating in hunting activities was protective against suicide attempts among young Inuit women(Reference Fraser, Geoffroy and Chachamovich186). Importantly, several studies found that participation in CF harvesting, sharing and consumption built pride and confidence(Reference Huet, Ford and Edge56), encouraged good mental and spiritual health(Reference Pufall, Jones and McEwen7,Reference Harper, Edge and Ford63,Reference Cunsolo Willox, Harper and Ford91,Reference Durkalec, Furgal and Skinner187) and was associated with high levels of social support and stronger relationships between individuals, their families, communities and the land(Reference Pufall, Jones and McEwen7,Reference Sheppard and Hetherington88,Reference Richmond and Ross184) .
Community-based interventions to improve food security and nutrition
Evaluations of nutrition intervention trials and community food programmes showed that community-based initiatives can successfully improve dietary adequacy, nutrition education, and food-related self-efficacy and intentions(Reference Mead, Gittelsohn and Roache32,Reference Ford, Lardeau and Blackett61,Reference Kolahdooz, Pakseresht and Mead77,Reference Organ, Castleden and Furgal78) . For example, the Healthy Foods North nutrition intervention, implemented in six communities in Nunavut and NWT, revealed that a holistic approach composed of education workshops, media campaigns and targeted changes in the food environment (e.g. improved availability of healthy MF) positively impacted food intentions and choices and improved dietary adequacy, especially among overweight and obese participants(Reference Bains, Pakseresht and Roache31,Reference Kolahdooz, Pakseresht and Mead77) . A dietary intervention programme implemented in childcare centres across Nunavik was found to improve children’s intakes of vegetables and fruit, grain products, and milk and alternatives, as well as several nutrients (e.g. n-3 PUFA, total Fe and Ca)(Reference Gagné, Blanchet and Vaissière34). Healthy eating policies have been implemented with some success in a school in Aklavik, NWT(Reference Fournier, Illasiak and Kushner188). Meanwhile, community food programmes, such as food banks, soup kitchens and community freezers, have successfully alleviated severe food insecurity and improved access to culturally appropriate foods in many northern communities(Reference Ford, Lardeau and Blackett61,Reference Organ, Castleden and Furgal78) .
Discussion
The purpose of this review was to synthesise published literature on ongoing dietary changes among Inuit living in northern Canada and implications for health and well-being. Evidence from across the Canadian Arctic indicates that a dietary transition is indeed occurring, characterised by reductions of CF and increased consumption of MF, and in particular NNDF(Reference Sheehy, Roache and Sharma46,Reference Kuhnlein, Receveur and Soueida55) . This transition is occurring despite widespread preferences for CF(Reference Galloway, Johnson-Down and Egeland54,Reference Ford, Lardeau and Blackett61,Reference Egeland, Faraj and Osborne87) . Ongoing dietary transitions are driven by the profound social, economic, cultural and environmental changes across Inuit Nunangat in the past several decades that impact all spheres of Inuit life(Reference Akande, Hendriks and Ruiter59). Such changes are largely rooted in colonial processes. Demographic pressures, poverty, lack of time (due to schooling and employment), loss of traditional knowledge, improved transportation and communication networks, hunting and fishing restrictions, shifting dietary preferences, fear of environmental contaminants and climate change have all challenged access to land and local resources, reduced CF harvest and consumption, and increased intake of NNDF foods(Reference Sheehy, Roache and Sharma46,Reference Akande, Hendriks and Ruiter59,Reference Ford, Lardeau and Blackett61,Reference Kenny, Fillion and Simpkin71,Reference Organ, Castleden and Furgal78,Reference Durkalec, Furgal and Skinner187) . Dietary changes are compounded by shifting lifestyle patterns (e.g. reduced physical activity) to alter health and disease patterns among Inuit across the Arctic(Reference Sharma, De Roose and Cao43,Reference Akande, Hendriks and Ruiter59) . While cardiovascular and metabolic risk factors and health outcomes were once absent among Inuit, successional cross-sectional studies suggest steadily increasing prevalence of overweight and obesity, impaired glucose tolerance and T2D, hypertension, hypercholesterolaemia and CVD(Reference Singer, Putulik Kidlapik and Martin2,Reference Pakseresht, Lang and Rittmueller84,Reference Chateau-Degat, Dewailly and Louchini145–Reference Egeland, Cao and Young147,Reference Healey and Meadows157,Reference Erber, Beck and De Roose160,162,189) . In many cases, prevalence estimates of overweight and obesity, type 2 diabetes, CVD and associated risk factors among Inuit are approaching or surpassing those seen in the Canadian general population and represent serious public health concerns(Reference Chateau-Degat, Dewailly and Louchini145,Reference Healey and Meadows157,Reference Hu, Singh and Kenny164,Reference Rodd and Sharma190,191,193).
In Inuit communities, the high cost of CF harvesting activities and nutritious MF poses a significant challenge to obtaining a healthy diet. High food costs persist despite the existence of NNC, a programme that replaced the Food Mail Program in 2011. NNC is administered by Crown-Indigenous Relations and Northern Affairs Canada (CIRNAC) and is designed to lower the cost of perishable foods by providing northern retailers with a subsidy on a selected list of foods(194). This programme has been criticised for several years due to poor reporting tools and programme responsiveness, inappropriate eligibility criteria for communities, failing to mitigate geographical inequities in the availability and affordability of food, a lack of accountability and failing to ensure that subsidies are passed to the consumer(Reference Burnett, Skinner and LeBlanc195–197). Despite the subsidies provided by NNC, the amount of household income spent on food in the Canadian North is considerably higher than in the rest of the country. Food Secure Canada and Qikiqtani Inuit Association have recommended developing a national food policy that embraces a food sovereignty approach for Inuit, including changes to the NNC to improve affordability and accessibility of healthy MF and increased support for CF harvesting(Reference Pakseresht, Lang and Rittmueller84,198) . While CIRNAC announced changes to the NNC programme in December 2018, including hunter support grants (to be implemented in 2020), it will be important to closely monitor the community impacts of NNC to determine if such changes ultimately benefit Inuit(199).
While CF are recognised as having nutritional, cultural and spiritual benefits, consumption of CF confers higher-than-average levels of some environmental contaminants in Inuit populations, including heavy metals (e.g. MeHg and Pb) and persistent organic pollutants (POP) (e.g. polychlorinated biphenyls, organochlorine pesticides, polybrominated diphenyl ethers, perfluoroalkyl and polyfluoroalkyl substances)(Reference Donaldson, Van Oostdam and Tikhonov16,Reference Van Oostdam, Donaldson and Feeley18) . While body burdens of many environmental contaminants (e.g. legacy POP such as polychlorinated biphenyls, organochlorine pesticides, polybrominated diphenyl ethers, and some polyfluoroalkyl substances) are declining(15), Inuit are still exposed to considerably higher levels of these contaminants than the Canadian general population, and some emerging POP are increasing cause for concern. Meanwhile, harvesting, preparing and consuming CF introduce unique risks of some zoonotic pathogens, including Toxoplasma gondii, Trichinella spp. and Clostridium botulinum (Reference Messier, Levesque and Proulx171–Reference Wright, Sargeant and Edge183). Thus, a serious challenge for public health practitioners, regulators, academics and Inuit communities is supporting, maintaining and promoting the cultural, social and nutritional health benefits of CF harvesting and consumption while also minimising exposure to harmful contaminants and zoonoses, particularly in the context of global environmental change(15,Reference Dewailly, Ayotte and Blanchet200,Reference Kinloch, Kuhnlein and Muir201) . This challenge has been acknowledged by several authors(Reference Laird, Goncharov and Egeland17,Reference Pacey, Nancarrow and Egeland28,Reference Mead, Gittelsohn and Roache30,Reference Kuhnlein39,Reference Rudkowska, Dewailly and Hegele166) and organisations(15,202) . A parallel challenge to risk assessment is risk communication, which must be done cautiously to avoid exaggerated fears of CF consumption(Reference Boyd and Furgal203–Reference Binnington, Curren and Chan206). A nascent body of research uses mathematical modelling to investigate the trade-offs of CF and MF based on food availability, cultural appropriateness, nutrition and health outcomes, and economic feasibility(Reference Laird, Goncharov and Egeland17). Such techniques have informed specific recommendations for food substitutions using food replacement modelling(Reference Laird, Goncharov and Egeland17,Reference Calder, Bromage and Sunderland45,Reference Rosol, Huet and Wood57,Reference Binnington, Curren and Chan206,Reference Gmelch, Hintelmann and Hickie207) . For example, Calder and colleagues suggested that replacing CF with locally caught Atlantic salmon will lead to net benefits for neurodevelopmental and cardiovascular health and reduced risk of cancer in three communities in Nunatsiavut(Reference Calder, Bromage and Sunderland45). However, a notable gap is the frequent failure of such models to account for the complex interactions between CF nutrients and contaminants (e.g. Se and n-3 PUFA may mitigate the harmful effects of MeHg and dietary calcium may mitigate Pb absorption and toxicity), risks of zoonoses and the less tangible benefits of CF harvesting, sharing and consumption which include cultural, social and mental health dimensions(Reference Hu, Eccles and Chan126,Reference Hu, Sharin and Chan127,Reference Alkazemi, Egeland and Roberts208,Reference Turgeon O’Brien, Gagné and Vaissière209) . Future modelling research should therefore incorporate community-identified priorities in an attempt to weigh all possible benefits and risks of CF against available MF. Thus, it is crucial that Inuit partners, researchers across disciplines and public health practitioners collaborate to develop culturally appropriate risk assessment and communication strategies grounded in Inuit Qaujimajatuqangit (knowledge) and scientific knowledge.
A number of gaps were identified that comprise possible avenues for further investigation (Box 2). A major concern is the limited research conducted in Inuit communities that directly assesses existing coping mechanisms and Inuit-led adaptations or solutions to challenges posed by dietary transitions. There is a need to better evaluate the feasibility and possible structures of community-led initiatives that address drivers of the dietary transition and subsequent health implications. Community-based nutrition interventions targeting retail food systems and food education have been shown to improve dietary adequacy, nutrition knowledge and food-related self-efficacy and intentions(Reference Mead, Gittelsohn and Roache32,Reference Ford, Lardeau and Blackett61,Reference Kolahdooz, Pakseresht and Mead77,Reference Organ, Castleden and Furgal78) . Community food programmes, such as food banks, soup kitchens and community freezers, have successfully alleviated severe food insecurity and improved access to culturally appropriate foods in many northern communities(Reference Ford, Lardeau and Blackett61,Reference Organ, Castleden and Furgal78) . However, such initiatives (and evaluations of their effectiveness) are far from ubiquitous in Inuit communities, and there is a need to support community capacity to establish and evaluate such programmes. There is also a notable lack of research that addresses economic and structural constraints (e.g. food environments) as key determinants of food insecurity, food choices and nutritional health(Reference McIntyre210,Reference Skinner, Burnett and Williams211) .
Box 2: Gaps in research on drivers and implications of the dietary transition among Inuit
-
There is a need to harmonise the priorities of academic research with those of Inuit communities and organisations
-
Very little published research actively incorporates Inuit Qaujimajatuqangit (knowledge) into data collection and analysis methods, reporting and recommendations
-
While many studies boasted engagement with Inuit communities as a key component of project development, there was little standardisation across articles for what constituted engagement and how this was reported
-
While many successive cross-sectional studies have examined dietary intake, dietary adequacy and health outcomes in Inuit communities, there have been few longitudinal studies to confirm and monitor long-term dietary and lifestyle changes and subsequent impacts on health
-
Future research should explore the relative contributions of dietary and lifestyle changes for increasing burdens of obesity and related non-communicable diseases
-
There is a necessity for harmonisation and standardisation of methods for assessing dietary intake, food security, health outcomes and northern food environments for better comparisons across populations and time periods(212)
-
Future research should assess the causes of gender- and age-based differences in traditional food consumption across Inuit communities(25)
-
Risk assessments and risk-benefit analyses (including food replacement models) of traditional foods tend to focus on one or a few exposures (e.g. environmental contaminants) and outcomes (e.g. physical health)(207,208). No studies have attempted to conduct actionable risk-benefit analyses of the trade-offs between traditional food and MF consumption that simultaneously incorporate multiple dimensions of health (e.g. physical, mental, spiritual and cultural), cost effectiveness, local/regional realities, feasibility, sustainability and food preferences
-
There is a need to prioritise research on the impacts of climate change on accessibility, availability and affordability of CF and MF and potential adaptation strategies to mitigate the risks of climate-mediated diet-related risks to Inuit health and well-being and integrate these issues in the risk-benefit analyses
-
There is a need to evaluate the necessity, feasibility and possible structures of community-led initiatives that provide solutions to challenges posed by the dietary transition to simultaneously reduce food insecurity and improve nutritional health while aligning with Inuit preferences, traditions and priorities
Finally, there is a crucial gap between the priorities of existing academic literature and those of Inuit communities and organisations. While there is a substantial body of academic literature assessing dietary adequacy, epidemiological trends and environmental contaminants in CF across Inuit Nunangat, very little published research is explicitly grounded in Inuit priorities, embodies participatory action research or other approaches that centralise Inuit experiences and collective action, or incorporates Inuit authorship. Recent Inuit-led consultations and publications have called for a food sovereignty approach that includes increased harvester-enabling infrastructure and harvester support and steward programmes, including wages for harvesters, funding for equipment and supplies, and skills development/mentorship programmes(205,Reference Adlard, Donaldson and Odland212–214) . Such priorities and potential interventions have received little attention from published academic literature; there is therefore considerable need to align the approaches of academic research with those of Inuit communities to unify resources, skills, evidence and voices.
Limitations
Several limitations of the current study should be acknowledged. Due to a limited systematic search strategy for identifying sources from grey literature, the findings may be biased towards academic and Western-derived knowledge while excluding other forms of information, such as Indigenous knowledge reports published by institutions outside academia. Furthermore, while the search strategy was wide-ranging, it was informed by pre-conceived notions of terms relevant to the research question, thereby possibly excluding relevant articles and research themes. Finally, as is common with the scoping review methodology, we did not assess any measures of study or data quality, so it is possible that biases present in included articles translated into similar biases in this review(Reference Grant and Booth215).
Conclusion
Canadian Inuit have undergone profound cultural, social and environmental changes that have undermined traditional ways of life and driven a dietary transition from primarily CF to MF in a short period of time. The health implications of this dietary transition are complex. Anaemia, overweight and obesity, and cardiometabolic health outcomes (e.g. hypertension, type 2 diabetes and CVD) are serious public health concerns. Declining traditional food consumption may also exacerbate mental and psychological health problems associated with the trauma of the loss of cultural and social traditions. However, CF can be a source of environmental contaminants, and declining CF consumption has been paralleled by reductions in population-level body burdens of POP, MeHg, and Pb. As of yet, it is relatively unknown to what extent this trend is due to reduced levels in CF themselves, declining consumption of certain CF or shifting patterns from some CF to others. There is a need for further research on activities that simultaneously promote the consumption of CF and healthy MF to reduce food insecurity and improve nutritional health in a way that is culturally appropriate and grounded in Inuit priorities. This is a monumental task that will require strong partnerships between Inuit, researchers, practitioners and policymakers. A combination of localised research, community-driven health and food policies, community-based monitoring and supports, and global activism will be required to address the complex health burdens driven by the dietary transition among Inuit populations.
Acknowledgements
Acknowledgements: The authors would like to acknowledge the participants who have contributed to research conducted with Inuit communities across the Canadian North. Additionally, the authors would like to thank the Nunavik Nutrition and Health Committee for their contributions to the manuscript revisions. Financial support: Financial support was provided by Health Canada through a private contract (no grant number). Conflict of interest: The authors declare no conflicts of interest. Authorship: M. Little conceptualised the review, conducted the literature search, screened articles for eligibility, reviewed full-text articles, conducted thematic analysis, wrote the manuscript and responded to manuscript revisions. H.H. screened articles for eligibility, reviewed full-text articles, extracted study characteristics, performed an analysis of study characteristics, developed all figures and provided comments on manuscript drafts. C.Z. screened articles for eligibility, resolved screening conflicts and provided comments on manuscript drafts. W.D. co-wrote some sections of the manuscript, provided comments on manuscript drafts, provided editorial assistance and assisted with responding to manuscript revisions. K.S. provided conceptual oversight of the review, consulted on review protocol, provided comments on manuscript drafts and assisted with responding to manuscript revisions. T.-A.K. provided conceptual oversight of the review, co-wrote some sections of the manuscript, provided comments on manuscript drafts and assisted with responding to manuscript revisions. A.C. provided extensive insight from a northern perspective on the review protocol and thematic analysis, provided comments on manuscript drafts and assisted with responding to manuscript revisions. J.G. screened some articles for eligibility, resolved screening conflicts, provided editorial oversight of manuscript drafts and assisted with responding to manuscript revisions. M. Lemire provided conceptual oversight of the review, consulted on review protocol, co-wrote some sections of the manuscript, provided comments on manuscript drafts and assisted with responding to manuscript revisions. Ethics of human subject participation: This manuscript does not include primary research involving human participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020002402








