



Beverage intake plays a significant role in daily energy and nutrient intake, influencing the overall quality of the diet. Beverages such as milk are important for calcium ingestion, while sugar-sweetened beverages, such as sodas and processed juices, contribute to added sugar intake. The energetic contribution of beverages to overall energy intake can increase the risk of health problems(Reference Scander, Monteagudo and Nilsen1). The consumption of sugar-sweetened beverages, for example, is often associated with the risk of developing diseases including hypertension and various types of cancers(Reference Hernández-López, Canto-Osorio and Vidaña-Pérez2,Reference Malik and Hu3) . Alcohol consumption, in turn, has also been linked to adverse outcomes, such as an increased risk of mortality from cardiovascular diseases (CVD) (Reference Krittanawong, Isath and Rosenson4).
The American Heart Association recommends limiting the intake of added sugars, in part, by avoiding sugar-sweetened beverages due to their known association with unfavourable health outcomes, including weight gain, type 2 diabetes, high blood pressure and CVD. However, the consumption of other beverages, such as alcohol, coffee and fruit juices, has also been linked to adverse health effects(Reference Rebholz, Young and Katz5).
Health promotion recommendations often focus on restricting specific unhealthy beverage choices; however, there is a lack of comprehensive information on the health implications of a wide range of beverage options(Reference Rebholz, Young and Katz5). This occurs because most studies on beverage consumption concentrate on specific beverage items instead of overall consumption patterns, making analyses more limited in assessing the risk of obesity and other cardiometabolic risk factors(Reference Salinas-Mandujano, Laiseca-Jácome and Ramos-Gómez6). Therefore, in the field of nutritional epidemiology, new studies should be developed with the perspective of investigating beverage consumption patterns rather than isolated beverage consumption in relation to health outcomes(Reference Lee and Shin7).
In this regard, non-communicable chronic diseases (NCCD) pose an emerging threat to global health and are listed by the WHO as the leading cause of death worldwide. The Global Burden of Disease study revealed that 543·25 per 100 000 inhabitants died globally in 2019 due to NCCD, also demonstrating a loss of 20 939·23 disability-adjusted life years per 100 000 inhabitants(Reference Leal, Vegi and Meireles8).
Therefore, NCCD such as those related to metabolic disorders like obesity, arterial hypertension and diabetes are serious public health issues since they are considered key risk factors for various diseases, such as CVD, which, in turn, deteriorate the quality of life and may increase mortality. As these chronic diseases are preventable and controllable, several risk factors have been identified, and among them, diet has emerged as a crucial modifiable factor. Additionally, the relationships between beverage consumption and various health outcomes have also been investigated(Reference Lee and Shin7).
Thus, this study aimed to characterise beverage consumption patterns and examine their association with the prevalence of NCCD in individuals aged 20 years or older from a capital city in Northeastern Brazil.
Methods
Study design
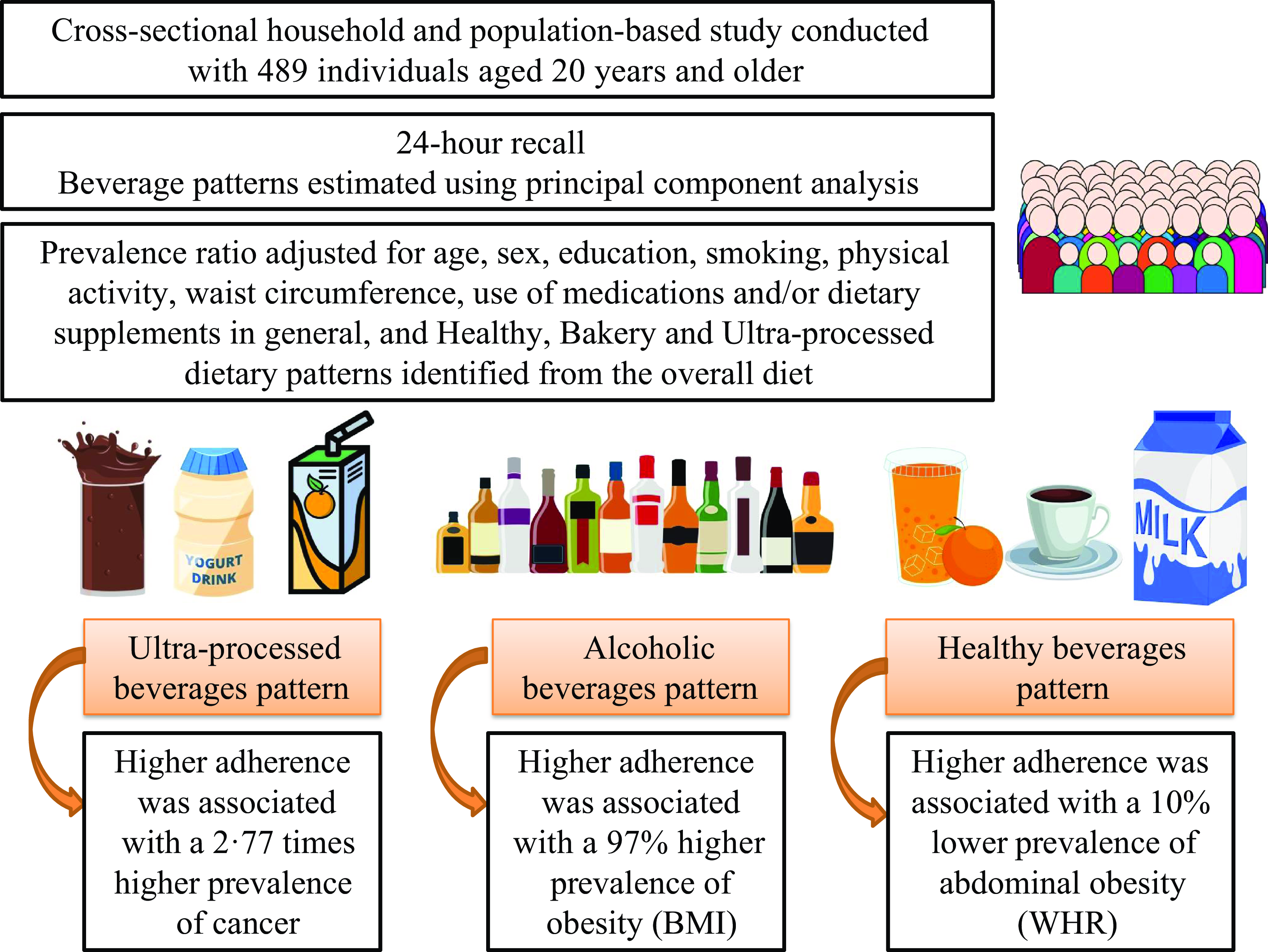
A cross-sectional, population-based study, which corresponds to a subset of data from the research ‘Household Health Survey in the municipalities of Teresina and Picos (PI)’, aimed at analysing the living conditions and health status of the population through home visits in urban areas of the municipalities of Teresina and Picos, Piauí, Brazil. For the present study, a subset was considered, focusing only on the sample from the city of Teresina, Piauí, Brazil.
The study employed a complex probabilistic sampling method, using clusters in two stages: census tract and household. The census tract is the smallest geographic unit with similar sociodemographic data of residents, consisting of approximately 300 families or about 1000 inhabitants.
For the sample size calculation, the population size of Teresina (767 557 inhabitants) was considered, based on the 2010 IBGE census(9), as well as the stratification of the population in both cities, according to the age of individuals for both sexes.
Based on this, the average number of individuals in each age group per household was calculated. To ensure that a minimum of thirty individuals from each age group participated in the sample, the number of households needed for each group was calculated. Subsequently, the expected number of individuals within the age group and sex was calculated, considering the group with the largest sample size in terms of households, represented by the 3–4 years old female group (n 578 households) in Teresina. Thus, the expected number of individuals for each age group and sex was calculated based on 578 households.
Then, a study was conducted simulating the behaviour of the 95 % CI and the coefficient of variation of the standard error of the proportion – CV(p) for proportion estimates (p) ranging from 10 % to 70 %, according to age groups, sex and their respective sample sizes (values for estimates of 50 %).
However, it was considered that during data collection, losses could occur due to various reasons. The final sample size for this study was adjusted using n = n0/0·90, assuming a response rate of 90 %, resulting in an approximate n of 642 households in Teresina.
Due to logistical reasons, a second collection stage was conducted only in the municipality of Teresina, following the same sampling plan. In this stage, 50 % of the households selected in each census tract were systematically included, forming a subsample of 617 individuals. For this, in addition to the data collected in the first stage, adolescents (10–19 years old), adults (20–59 years old) and older adults (60 years old or older) residing in households included in the subsample were invited to participate in data collection on food consumption, using a 24-h food recall (R24h).
For this study, the age groups of adults (20–59 years) and older adults individuals (60 years or older), of both sexes, who had complete data on dietary consumption, anthropometry, medical diagnosis of NCCD and comprehensive sociodemographic, economic and lifestyle data, were included. Out of the 497 adults and older adults individuals initially included, only eight were excluded due to incomplete data, resulting in a final sample of 489 participants. Comparative analyses of the variables of interest, following the exclusions, indicated no significant differences between the characteristics of the total sample and the final study sample, confirming that the sample remains representative (Fig. 1). Only adults and older adults were selected for the present study due to the low prevalence of NCCD in adolescents. Including adolescents would complicate statistical analyses because of their lower prevalence rates. Additionally, adolescents often have significantly different eating habits compared with adults and older adults, which could introduce bias into the study’s findings. Therefore, focusing on adults and older adults allows for a more homogenous sample, facilitating more accurate and reliable results. More information about the sampling process is described in the article by Rodrigues et al. (Reference Rodrigues, Costa e Silva and Oliveira10).

Fig. 1. Sample selection flow chart.
Data collection
Sociodemographic (age, sex and education), economic (family income), lifestyle (smoking and physical activity) and self-reported chronic disease diagnosis data were obtained through the administration of questionnaires. These questionnaires were previously used in other Brazilian population-based studies(Reference Szwarcwald, Malta and Pereira11,12) and were administered using the Epicollect 5® app (Imperial College London, 2018) on mobile devices.
Diagnosis of non-communicable chronic diseases
The diagnosis of NCCD was self-reported through the question ‘Has any doctor ever given you a diagnosis of this disease?’ with possible answers of ‘Yes’, ‘No’ and ‘No response’. The investigated diseases were arterial hypertension, diabetes mellitus, hypercholesterolemia and cancer.
Anthropometric data
Body weight and height were measured according to Jelliffe and Jelliffe(Reference Jelliffe, Jelliffe, Jelliffe and Jelliffe13) and Cameron(Reference Cameron and Tanner14). Body weight was measured with an electronic scale with an accuracy of 100 g. Height was measured with a portable stadiometer with an accuracy of 0·1 cm. BMI was calculated according to the WHO(15) and was classified according to the WHO(15) recommendation for adults and according to OPAS(16) for older adults. Waist circumference (WC) was measured at the midpoint between the last true rib and the iliac crest, using an inelastic measuring tape with an accuracy of 0·1 cm(17). WC classification was performed as recommended by the WHO(17), considering cardiometabolic risk for a WC ≥ 80 cm for women and ≥ 94 cm for men.
The waist-to-height ratio (WHR) was calculated as the ratio of WC in centimetres to height in centimetres. Individuals with WHR greater than or equal to 0·50 were classified as having abdominal obesity(Reference Ashwell and Hsieh18).
Dietary intake
Dietary intake was obtained through a R24h using the Multiple-Pass Method(Reference Moshfegh, Rhodes and Baer19). A second R24h was conducted in 40 % of the population after a 2-month interval, employing the same procedures as the first interview, to adjust for intrapersonal variability, as demonstrated in the study by Verly-Jr et al. (Reference Verly-Jr, Castro and Fisberg20), which showed minimal loss of precision in estimating dietary intake, regardless of sample size. The household measures reported by the interviewees were converted into grams (g) or millilitres (ml) with the help of the Table for Assessing Food Intake in Household Measures(Reference Pinheiro, Lacerda and Benzecry21). Data from both R24h assessments were used to adjust for intrapersonal variability in intake using the Multiple Source Method statistical technique(Reference Harttig, Haubrock and Knüppel22).
Descriptions of preparations were standardised, and in cases where habitual sugar consumption was reported but the interviewee could not quantify it, the addition of 5 g of sugar for every 100 ml of coffee, coffee with milk (whole, semi-skimmed and skimmed milk), tea and 10 g of sugar for every 100 ml of juices and smoothies was standardised.
Dietary patterns
More than 800 food items consumed were identified and categorised into twenty-one food groups based on consumption frequency and nutritional characteristics. The data were analysed in grams or millilitres. Measurements were not standardised. Dietary patterns were identified through principal component analysis using the Stata® version 13.0 program. Initially, the applicability of the method was assessed using statistical tests: Kaiser–Meyer–Olkin (KMO), which is acceptable when KMO > 0·50, and Bartlett’s test of sphericity (BTS), acceptable when < 0·05. The BTS measured the presence of relationships within the data (P < 0·001), and the KMO measured the sampling adequacy (KMO = 0·51). Both demonstrated the dietary dataset was suitable for principal component analysis which reduces the diet components based on their correlations with one another while retaining as much variation within the diet as possible(Reference Mumme, Conlon and Von Hurst23).
The scree plot (graphical representation of eigenvalues >1·45) was analysed. Three factors or patterns were identified. The factors (dietary patterns) were then orthogonally rotated using the varimax rotation technique to ensure they were uncorrelated and to facilitate the interpretation of their meaning. Factor loadings with values ≥ 0·25 were considered components of the pattern. Based on the items considered in each factor, the patterns were interpreted and labelled as ‘Healthy’, ‘Bakery’ and ‘Ultra-processed’. The three patterns obtained explained 20·1 % of this population’s dietary consumption (online Supplementary Table 1).
Beverage consumption patterns
Initially, all beverages (measured in millilitres) were grouped into thirteen different categories based on consumption frequency and nutritional characteristics. Measurements were not standardised. The categories included teas (sweetened and unsweetened), coffee with milk (sweetened or not), coffee without milk (sweetened or not), skimmed or semi-skimmed milk, whole milk, dairy beverages, chocolate milk, natural juices (sweetened or not), fruit smoothies (sweetened), ultra-processed juices, sodas, fermented alcoholic beverages (beers) and distilled alcoholic beverages (whisky and cachaça).
Subsequently, the applicability of the method was assessed through the statistical tests KMO (KMO = 0·52) and BTS (P < 0·001). Both demonstrated the dietary dataset was suitable for principal component analysis.
Following this, through the principal component analysis of beverage groups, beverage consumption patterns were categorised. The factors (beverage patterns) were orthogonally rotated using the varimax rotation technique to ensure they were uncorrelated and to facilitate the interpretation of their meaning. Factor values were determined after evaluating eigenvalues, graphical analysis and interpretability. Each factor was defined by a subgroup that placed beverages on the factor axis, with an absolute loading ≥ 0·25 (groups with a loading factor ≥ 0·25 were considered to make a significant contribution to the beverage pattern). The derived factors were then labelled to make the data easily interpretable.
Covariates
The covariates used included sociodemographic and economic data (age, sex, education and family income), lifestyle factors (smoking and physical activity), use of medication and/or supplements in general, and anthropometric data (body weight, height and WC).
Smoking status was estimated using the question ‘Do you currently smoke or have you smoked in the past (at least 100 cigarettes or 5 packs)?’ And through the question ‘Do you currently smoke? If yes, do you smoke daily?’
The use of medication or supplements in general was assessed using the question: ‘Are you currently taking any medication or food, vitamin or mineral supplements?’
Physical activity was estimated using the International Physical Activity Questionnaire (IPAQ), the long version for adults and the short version for the elderly(Reference Matsudo, Araújo and Matsudo24). Individuals were classified as insufficiently active or active according to the 2020 WHO recommendations(25), which advocate for at least 150 min of light to moderate physical activity and/or 75 min of vigorous physical activity per week.
Ethical aspects
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Human Research Ethics Committee of the Federal University of Piauí under opinion number 2.552.426. Written informed consent was obtained from all subjects.
Statistical analysis
Continuous variables were expressed as mean and standard deviation, and categorical variables were expressed as absolute and relative values. The distribution of continuous variables was analysed using the Shapiro–Wilk test. The Kruskal–Wallis test and the Bonferroni post hoc test were used to analyse continuous variables. Categorical variables were analysed using Pearson’s χ 2 test. The factor scores of beverage patterns were categorised into tertiles. The association between tertiles of beverage consumption patterns and the prevalence of NCCD was examined through Poisson regression, expressed as crude and adjusted prevalence ratio (PR), adjusting for potential confounding factors based on the scientific literature(Reference Rebholz, Young and Katz5,Reference Rivera-Paredez, Muñoz-Aguirre and Torres-Ibarra26) , including age, sex, education, smoking, physical activity, WC, use of medications and/or supplements in general, and Healthy, Bakery, and Ultra-processed dietary patterns identified from the overall diet in the first model. Due to the cross-sectional nature of this study, which prevents determining whether WC is a mediator or a confounder, a second model without adjustment for this variable was included.
The sample was not weighted, given that the probability of the sample was equiprobable. All analyses were performed using Stata version 13.0. The survey mode was utilised to adjust the analyses for the complex sampling of the survey. A significance level of 5 % and 95 % CI were adopted.
Results
Table 1 shows the results of the characterisation of the study sample. The average age was 46·5 years, and the majority of the population was female (66·9 %), of brown skin (62·4 %), had studied up to high school (40·9 %), had a family income of up to two minimum wages (76·5 %), were not smokers (78·1 %) and were physically active (80·4 %).
Table 1. Characterisation of the study population (n 489) (Mean values and standard deviations; numbers and percentages)

WC, waist circumference; WHR, waist-to-height ratio.
* Yellow, Indigenous and others.
As for the prevalence of NCCD, the prevalence of hypertension, diabetes, hypercholesterolemia, cancer, obesity and abdominal obesity was 28·0 %, 9·6 %, 20·4 %, 3·9 %, 27·0 % and 65·6 %, respectively.
Table 2 shows the factor loadings of the patterns identified. Three patterns of beverage consumption were identified: Ultra-processed Beverages Pattern, Alcoholic Beverages Pattern and Healthy Beverages Pattern. The Ultra-processed Beverages Pattern was characterised by the consumption of ultra-processed dairy beverages, semi-skimmed and skimmed milk, chocolate milk, industrialised juices and sodas. The Alcoholic Beverages Pattern was characterised by the consumption of fermented and distilled alcoholic beverages, and the Healthy Beverages Pattern was characterised by the consumption of coffee with milk, skimmed or semi-skimmed milk and natural fruit juices and the non-adherence to the consumption of coffees without added milk.
Table 2. Factor loading matrix for beverage consumption patterns (n 489)

Factor loadings ≥ 0· 25.
The bold text has been used to highlight and facilitate the identification of the beverages that represent each consumption pattern.
The KMO value was 0·52. The BTS was < 0·001. Each dietary pattern presented eigenvalues of 1·45, 1·42 and 1·41 for Ultra-processed Beverages Pattern, Alcoholic Beverages Pattern and Healthy Beverages Pattern, respectively. The three patterns obtained explained 33·0 % of this population’s beverages consumption.
Table 3 presents the characterisation of the study population according to tertiles for each beverage consumption pattern. Individuals in the first tertile of the Ultra-processed Beverages Pattern had a higher mean age. In contrast, those in the third tertile of the Alcoholic Beverages Pattern were younger compared with the first tertile. Significant associations were found between skin colour and the Alcoholic Beverages Pattern, as well as between education and all three beverage patterns.
Table 3. Characterisation of the study population according to tertiles of beverages consumption patterns (n 489) (Mean values and standard deviations; numbers and percentages)

WC, waist circumference; WHR, waist-to-height ratio.
* Yellow, Indigenous and others.
† Pearson χ 2 test.
‡ Kruskal-Wallis test followed by the Bonferroni post-hoc test. Different superscript letters in the same row indicate a statistically significant difference.
Additionally, individuals in the first tertile of the Ultra-processed Beverages Pattern had a higher prevalence of hypertension, whereas those in the third tertile of this pattern had a higher prevalence of cancer. Conversely, individuals in the third tertile of the Healthy Beverages Pattern exhibited a lower prevalence of abdominal obesity, as estimated by the waist-to-height ratio (WHR).
Table 4 shows the results of the association between beverage consumption patterns and the prevalence of NCCD. It was observed that individuals with higher adherence to the Ultra-processed Beverages Pattern (third tertile) had a 2·77 times higher prevalence of cancer (PR: 3·77; 95 % CI 1·57, 9·07) compared with the first tertile in adjustment model 1, and 2·91 times higher prevalence of cancer in model 2 (PR: 3·91; 95 % CI 1·64, 9·34). Additionally, higher adherence to the Alcoholic Beverages Pattern, represented by individuals in the third tertile, was associated with a 97 % higher prevalence of obesity in model 2 (PR: 1·97; 95 % CI 1·13, 3·44), compared with those in the first tertile.
Table 4. Association between the beverages consumption patterns and the prevalence of non-communicable chronic diseases (n 489) (95 % confidence intervals)

PR, prevalence ratio; WC, waist circumference; WHR, waist-to-height ratio.
* Adjusted for age, sex, education, smoking, physical activity, WC, use of medications and/or dietary supplements in general, and Healthy, Bakery and Ultra-processed dietary patterns identified from the overall diet.
† Not adjusted for WC.
On the other hand, individuals in the second tertile of adherence to the Healthy Beverages Pattern had a 39 % lower prevalence of hypercholesterolemia compared with the first tertile in model 1 (PR: 0·61; 95 % CI 0·40, 0·92) and model 2 (PR: 0·61; 95 % CI 0·40, 0·93). Similarly, individuals in the third tertile of adherence to the Healthy Beverages Pattern also had a 10 % lower prevalence of abdominal obesity estimated by the WHR in adjustment model 2 (PR: 0·90; 95 % CI 0·83, 0·97).
Discussion
In this study, three main patterns of beverage consumption were identified: Ultra-processed Beverages Pattern, Alcoholic Beverages Pattern, and Healthy Beverages Pattern. Similar beverage consumption patterns were found in the study by Lee and Shin(Reference Lee and Shin7), conducted with Koreans from the Korea National Health and Nutrition Examination Survey (KNHANES), such as the Healthy Beverages consumption pattern characterised by high consumption of fruit/vegetable juices, as well as the Sugar-Sweetened Beverages pattern characterised by elevated consumption of beverages like sodas, industrialised fruit juices and sugary coffees or teas.
Similarly, in studies by Salinas-Mandujano et al. (Reference Salinas-Mandujano, Laiseca-Jácome and Ramos-Gómez6) and Rebholz et al. (Reference Rebholz, Young and Katz5), conducted with Mexican students from the Autonomous University of Queretaro and US adults from Jackson, Mississippi, respectively, the Alcoholic Beverages Pattern was also identified, characterised by high consumption of distilled and fermented beverages. Additionally, in the study by Rebholz et al. (Reference Rebholz, Young and Katz5), the pattern of fruit/vegetable juice consumption was also identified, similar to the Healthy Beverages Pattern found in the present study.
The data from this study demonstrated that those with higher adherence to the Ultra-processed Beverages Pattern (third tertile) had a higher prevalence of cancer. Furthermore, higher adherence to the Alcoholic Beverages Pattern was associated with a higher prevalence of obesity. Conversely, individuals in the second tertile of adherence to the Healthy Beverages Pattern had a lower prevalence of hypercholesterolemia compared with the first tertile, and individuals in the third tertile of adherence to this beverage pattern had also a lower prevalence of abdominal obesity estimated by the WHR.
Similar to our findings, the pattern of healthy beverage consumption identified in the study by Lee and Shin(Reference Lee and Shin7) was inversely associated with abdominal obesity and elevated triglycerides, indicating that the consumption of milk-based beverages and natural fruit juices may have a protective effect against obesity and dyslipidemias.
In this study, the Healthy Beverages Pattern was predominantly characterised by the intake of natural fruit juices and low-fat milk. Moderate fruit juice consumption can bring nutritional benefits and does not seem to have a negative impact on body weight measures(Reference Garduño-Alanís, Malyutina and Pajak27). In a review study, the consumption of fruit juice, in moderate doses consistent with the dietary guidelines of the USA and some European countries, approximately 75–224 ml per day, did not increase the risk of obesity or other NCCD(Reference Ruxton and Myers28). Similarly, in a review of observational studies and randomised clinical trials, no statistical associations were found between regular fruit juice consumption and BMI or weight gain(Reference D’Elia, Dinu and Sofi29).
Natural fruit juices are sources of various micronutrients and bioactive compounds that can contribute to health maintenance, such as potassium, vitamin C, folate, carotenoids and polyphenols (hesperidin, quercetin, carotenoids, anthocyanins and punicalagin). These substances could even contribute to slower intestinal absorption of dietary sugars(Reference Ruxton and Myers28), which may reduce insulin spikes and prevent the accumulation of body fat.
Milk and dairy products are valuable sources of high-quality protein, promoting satiety and contributing significantly to the recommended adult intake of calcium. Calcium intake may modulate adipocyte lipid metabolism and enhance fatty acid absorption through its effects on intracellular calcium levels. Moreover, higher calcium intake has been linked to reduced lipogenesis and increased lipolysis through hormonal regulation(Reference Schwingshackl, Hoffmann and Schwedhelm30). Furthermore, milk and dairy products are also rich in compounds with antioxidant properties, including sulphur amino acids, whey proteins, vitamins A, E and C, or β-carotene(Reference Stobiecka, Król and Brodziak31).
Regarding the Alcoholic Beverages Pattern, this study showed that this pattern was associated with general obesity, which contrasts with findings from other studies(Reference Salinas-Mandujano, Laiseca-Jácome and Ramos-Gómez6,Reference Rivera-Paredez, Muñoz-Aguirre and Torres-Ibarra26) , where adopting the Alcoholic Beverages Pattern was associated with a better cardiometabolic profile and lower body fat percentage.
However, alcohol has a relatively high energy content of 7·1 kcal per gram, while also stimulating appetite and limiting the development of satiety. Consequently, alcohol intake can be one of the main contributors to the development of overweight and obesity(Reference Inan-Eroglu, Powell and Hamer32).
The results of a study conducted with NHANES data (2003–2012) demonstrated a positive association between excessive alcohol consumption (equal to or greater than five drinks) and BMI in men, while individuals who consumed alcohol moderately had higher BMI compared with former drinkers(Reference Butler, Popkin and Poti33). Thus, the contrasting results observed between studies may be related to the amount of alcohol consumed and the type of alcoholic beverage consumed, as the consumption of beverages such as wine is generally not associated with increased body weight(Reference Inan-Eroglu, Powell and Hamer32). In the present study, no participant reported wine consumption.
The higher adherence to the Ultra-processed Beverages Pattern observed in this study was positively associated with a higher prevalence of cancer in the sample. Most of the beverages constituting this pattern were sugar-sweetened beverages, such as ultra-processed dairy beverages and industrialised juices. Similar results were reported in the NutriNet-Santé cohort study conducted with French individuals, which found a positive association between the intake of sugar-sweetened beverages and the overall risk of cancer, including breast cancer(Reference Debras, Chazelas and Srour34).
The consumption of sugar-sweetened beverages may increase the risk of certain types of cancer by contributing to excess adiposity(Reference Malik and Hu3). However, this association remained even after adjustments for WC in the present study, suggesting that other mechanisms beyond excess weight may be involved in this relationship. Even in the absence of weight gain, other mechanisms such as oxidative stress, inflammation and insulin resistance can also be promoted by sugar intake. High sugar intake increases postprandial glucose responses, stimulating the production of pro-oxidant molecules and inducing DNA damage, thereby increasing the risk of cancer(Reference Debras, Chazelas and Srour34). Furthermore, many ultraprocessed beverages may contain caramel colourings, such as methylimidazole, which are known carcinogens(Reference De Lorgeril, Salen and Rabaeus35).
Despite the results obtained, it is important to note that, in some cases, such as the association between the consumption of ultra-processed beverages and cancer, significantly wide CI were observed, which can be attributed to the limitation of the analytical sample divided into tertiles based on cancer status, with only nineteen individuals diagnosed with the disease. This division resulted in small subgroups, affecting the precision of the estimates. Therefore, the interpretation of these results must take this limitation into account, emphasising the need for future studies with larger and more representative samples to confirm such observations.
The lack of association observed between beverage consumption patterns and the prevalence of hypertension and diabetes can be explained by factors such as different biological mechanisms between NCCD, which affect how beverage consumption impacts each condition differently, as well as the influence of uncontrolled confounding factors such as genetics, family history and differences in disease control and treatment adherence. Moreover, given the cross-sectional nature of the study, a larger number of people diagnosed with hypertension and diabetes may have a greater impact on the average consumption of beverages, resulting from a possible reverse causality.
The limitations of this study include the use of the R24h to assess food consumption, as it is prone to memory bias and may lead to underestimation or overestimation of intake. Additionally, the study did not collect data on plain water consumption, a significant confounding variable that could impact the intake of other beverages as well as the risk of NCCD. Another limitation is the potential for underdiagnosis due to self-reporting of NCCD. Furthermore, the cross-sectional nature of the study does not allow for the establishment of clear cause-and-effect relationships, focusing instead on prevalence rather than incidence. On the other hand, it is noteworthy that only a few studies have evaluated the impact of beverage consumption on health using this methodological approach, since the analysis of beverage consumption patterns provides a more accurate representation of overall drinking behaviour and is easier to understand and communicate, especially in clinical, public health or research contexts, facilitating the implementation of recommendations and interventions based on beverage consumption patterns.
Conclusion
The data from this study showed that beverage consumption patterns can be associated with NCCD regardless of factors such as age, sex, education, smoking, physical activity level, WC, use of medications and/or dietary supplements, and overall diet quality as estimated by food consumption patterns.
In light of this, it is important to conduct more studies investigating the impact of beverage consumption patterns on population health, rather than focusing on research that evaluates specific types of beverages in isolation. This is especially crucial given the current scarcity of studies employing this methodological approach, which provides a more comprehensive understanding of how different types of beverages collectively influence health outcomes. Focusing on broader patterns rather than isolated beverage types contributes significantly to addressing gaps in current research methodologies.
Acknowledgements
This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Coordination for the Improvement of Higher Education Personnel (grant number 23038.000925/2016-02). The Coordination for the Improvement of Higher Education Personnel had no role in the design, analysis or writing of this article.
Conceptualisation: L. C. d. C. L. and K. d. M. G. F.; methodology: L. C. d. C. L., P. C. d. A. F. V., F. d. C. C. and K. d. M. G. F.; formal analysis: L. C. d. C. L., P. C. d. A. F. V., K. d. M. G. F., L. M. N., J. d. M. C. and P. V. d. L. S.; investigation: L. C. d. C. L., K. d. M. G. F., P. C. d. A. F. V., L. M. N., J. d. M. C. and F. d. C. C.; data curation: L. C. d. C. L. and K. d. M. G. F.; writing – original draft preparation: L. C. d. C. L.; writing – review and editing: L. C. d. C. L., K. d. M. G. F. and P. V. d. L. S.; visualisation: L. M. N., J. d. M. C., P. V. d. L. S., F. d. C. C. and K. d. M. G. F.; supervision: K. d. M. G. F.; project administration: K. d. M. G. F.; funding acquisition: K. d. M. G. F.
There are no conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114524002083







