



Introduction
This Research Note reflects on the lessons that our team learned while implementing a mixed-methods study with foreign-born older adults in five languages (see also Tong, McKay, Martin-Matthews, Mahmood, & Sims-Gould, Reference Tong, McKay, Martin-Matthews, Mahmood and Sims-Gould2019; Tong, Sims Gould, & McKay, Reference Tong, Sims Gould and McKay2018; Tong, Sims-Gould, & McKay, Reference Tong, Sims-Gould and McKay2016). One third of older adults in Canada are foreign-born (Ng, Lai, Rudner, & Orpana, Reference Ng, Lai, Rudner and Orpana2012), but research with this heterogenous group is limited in both size and scope (Koehn, Badger, & Mullings, Reference Koehn, Badger and Mullings2015). What does exist is underdeveloped and fragmented; research on foreign-born older adults (FBOAs) in Canada is difficult to locate and is often found in the “grey literature” (Koehn et al., Reference Koehn, Badger and Mullings2015). The self-reported health of both middle-aged immigrants (Kobayashi & Prus, Reference Kobayashi and Prus2012) and FBOAs is poor compared to that of their Canadian-born peers (Ng et al., Reference Ng, Lai, Rudner and Orpana2012). Several studies confirm that these foreign-born adults, similarly, report a higher prevalence of chronic conditions, poor self-rated health, and greater difficulties with instrumental activities of daily living (IADLs) (e.g., Dunn & Dyck, Reference Dunn and Dyck2000; Lai, Tsang, Chappell, Lai, & Chau, Reference Lai, Tsang, Chappell, Lai and Chau2007). Recent scoping reviews also suggest that foreign-born older adults experience difficulties in accessing primary care (Wang, Guruge, & Montana, Reference Wang, Guruge and Montana2019), have unmet health needs (Wang et al., Reference Wang, Guruge and Montana2019), and experience mental health inequities (Guruge, Thomson, & Seifi, Reference Guruge, Thomson and Seifi2015). In order to appropriately intervene, we must first have a baseline understanding of health habits and behaviours among potentially at-risk groups (Prochaska & Velicer, Reference Prochaska and Velicer1997).
Although physical activity and mobility (i.e., movement around one’s home and community) are decidedly health enhancing in older age (Chodzko-Zajko et al., Reference Chodzko-Zajko, Proctor, Singh, Minson, Nigg, Salem and Skinner2009; Paterson, Jones, & Rice, Reference Paterson, Jones and Rice2007), we know very little about the physical activity and mobility habits of FBOAs in Canada. This is especially true for those foreign-born adults who are unable to participate in research that is conducted in Canada’s two national languages, English and French (Koehn et al., Reference Koehn, Badger and Mullings2015). The objective of our study was to assess the physical activity and mobility of FBOAs in South Vancouver, British Columbia, using a linguistically accessible approach that would facilitate the participation of FBOAs who do not necessarily communicate in one of the official languages (also reported in Tong et al., Reference Tong, Sims Gould and McKay2018, Reference Tong, McKay, Martin-Matthews, Mahmood and Sims-Gould2019).
There is lively debate in the translation and interpretation literature about the merits and pitfalls of various methods and approaches, including how to conduct translations in a qualitative research context (e.g., Clark, Birkhead, Fernandez, & Egger, Reference Clark, Birkhead, Fernandez and Egger2017; Larkin, de Casterlé, & Schotsmans, Reference Larkin, de Casterlé and Schotsmans2007; Santos, Black, & Sandelowski, Reference Santos, Black and Sandelowski2015). Similarly, there is a sizeable body of literature on the importance of translation and validity with survey measures (e.g., Angel, Reference Angel2013; Hambleton & Patsula, Reference Hambleton and Patsula1998; Milfont & Klein, Reference Milfont and Klein2018; World Health Organization, 2018). Notwithstanding, we found limited guidance on the practical aspects of conducting a multilingual study with older adults from diverse backgrounds.
Researchers have completed multilingual studies on the physical activity and mobility of FBOAs. For example, in their analysis of older adults’ walking behaviours in Melbourne, Australia (n = 341), Bird et al. conducted surveys in English, Croatia, Greek, Italian, Macedonian, Maltese, and Vietnamese (Bird et al., Reference Bird, Radermacher, Sims, Feldman, Browning and Thomas2010; Feldman, Radermacher, Browning, Bird, & Thomas, Reference Feldman, Radermacher, Browning, Bird and Thomas2008). As a companion to this research, Feldman et al. (Reference Feldman, Radermacher, Browning, Bird and Thomas2008) produced an insightful manuscript on the essential role of bilingual interviews and recommendations regarding the recruitment and retention of “culturally and linguistically distinct” older adults. What was unique about our study, however, is that our mixed-methods approach meant that we needed to consider multilingual data collection in multiple forms, at multiple time points. We sought guidance on multilingual data collection with older adults using surveys, accelerometers, global positioning system (GPS) units, qualitative interviews, and walking interviews.
Objective
Given the limited guidance that we found in the literature, the aim of this Research Note has been to share the lessons learned from the implementation of a mixed-methods study in five languages, with older adults from diverse ethno-cultural groups.
Study Overview
Our study (Tong et al., Reference Tong, Sims-Gould and McKay2016, Reference Tong, Sims Gould and McKay2018, Reference Tong, McKay, Martin-Matthews, Mahmood and Sims-Gould2019) aimed to characterise the physical activity habits and mobility of multilingual and non-English-speaking FBOAs who resided in South Vancouver, British Columbia. Participants were foreign-born, over the age of 65, community-dwelling, and able to complete the study in either Hindi, Punjabi, Cantonese, Mandarin, or English. (For more information on recruitment, please see Tong et al. [Reference Tong, Sims Gould and McKay2018]). We worked closely with the Seniors Advisory Council at South Vancouver Neighbourhood House to conduct this research, which was approved by the University of British Columbia’s ethics board.
The mixed-methods study consisted of two waves. In the first (n = 49), we used questionnaires to assess five domains: self-reported physical activity, self-reported health, perceptions of the local built environment, height and weight, and demographics. Participants were also given an accelerometer (ActiGraph GT3X+) to measure their daily physical activity for one week, and a GPS unit to measure their spatial mobility for the same week (n = 46). In the second wave, which included the same cohort of participants, we conducted in-depth interviews (n = 18) and interACTIVE interpreted walking interviews (n = 13) to gain a deeper understanding of participants’ physical activity habits and their neighbourhood mobility (Tong et al., Reference Tong, Sims-Gould and McKay2016). This article focuses on the methods and techniques that we used to implement a mixed-methods study with older adults in five languages. The following section further elaborates on the techniques we used and lessons learned.
Results: Lessons from the Field
Early Community Engagement
We worked with the Seniors Advisory Council (SAC) for four years, including more than a year before we commenced the study. We developed a close working relationship with the SAC, which had staff and volunteers who represented several ethno-cultural minority groups in South Vancouver. For more information on our collaboration with the SAC, see Tong et al. (Reference Tong, Sims Gould and McKay2018). In a series of approximately 20 in-person meetings, we worked with volunteers from the SAC to determine study objectives, apply for funding, and design the study. Prior to commencing data collection, volunteers from the SAC played a vital role in ensuring that our study was culturally and linguistically accessible and tailored to the anticipated participants. It was the SAC that selected the five languages, given their knowledge of local FBOA residents. Volunteers from the SAC recommended translation agencies and interpreters that they had worked with previously. They also reviewed the recruitment materials (consent forms, posters, and letters of introduction) to provide feedback on the translation. The SAC encouraged us to simplify the documents, to make the language less academic and more accessible. We incorporated their feedback prior to submitting materials for ethics approval and final translation. The SAC also cautioned us that some potential participants may not read or may have a very low level of comprehension of their first language in the written format; having this knowledge ahead of time allowed us to plan study documents and data collection accordingly.
Ethics and Recruitment
The first translation task was submitting English and translated versions of the consent forms to our university behavioural research ethics board. Our ethics board requires all consent forms to be professionally translated, even if the study investigators can conduct translations themselves. Professional translation is costly, especially when one document must be translated into five different languages. Most organisations charge by the word for professional translation, so we endeavoured to keep the consent forms as complete yet succinct as possible. Per the guidance of the SAC, we also endeavoured to make the language of the consent form’s English version as simple as possible, prior to translation. We emphasised to the translators that our objective was to keep the consent forms at an accessible reading level. Volunteers from the SAC reviewed the translated versions of the consent forms before we commenced recruitment. The SAC volunteers highlighted several instances in which the language of the consent form needed to be simplified.
Upon receipt of ethics approval, peer volunteers from the SAC introduced the study and collected the names of individuals interested in the study. Volunteers shared information about the study at the South Vancouver Neighbourhood House, community centres, ESL and computer classes, places of worship, and culturally specific social groups and gatherings. These were the same volunteers who helped conceive of and design the study. Recruitment sheets included name, phone number, preferred time of call, and preferred language of communication. Some participants spoke numerous languages (e.g., English, Hindi, Punjabi and Urdu, or English, Mandarin, and Vietnamese), and it was therefore important to ask them which language they would prefer. Multilingual research assistants then followed up with this list of names to confirm eligibility and to further describe the study.
Translation and Data Collection Team
Team members who worked with participants, including the research assistants (RAs) and interpreters were all women with prior experience working with older adults and vulnerable populations. The team members’ roles, education and experience, and languages are summarised in Table 1. It was cost-effective and efficient to hire RAs who spoke multiple languages (for example, one RA spoke Mandarin and Cantonese; another spoke Hindi and Punjabi). We knew that it was vital to create a direct line of communication between the RAs and research participants; we never wanted a situation whereby an older adult telephoned our team and was misunderstood or unable to communicate. On study documents we highlighted and repeated the one telephone number that would directly connect study participants to the research assistant who spoke their language. This process included removing our general office telephone number from letterhead and stationery to avoid any potential confusion or miscommunication. We budgeted for cellular phones for RAs and planned for overtime hours so that participants could reach RAs outside regular business hours on these phones.
Table 1: Multilingual data collection team

FBOAs = Foreign-born older adults
Our consent forms also included the contact information for the university research board; this is a standard requirement of most research boards to protect participants. If a participant telephoned this number, the university official answering the phone likely would have answered and communicated in English. To support this potential communication, we provided every participant with an English language consent form, with the hope that participants could and would share this form with a trusted family member or other English-speaking individual who could speak to the university board on their behalf. During data collection, we saw many adult children reviewing our English version of the consent forms.
Data Collection – Wave 1: Surveys, Accelerometers, and GPS Units
Data collection took place from May through June 2013. Data collection for both waves occurred in quick succession, enabling us to capitalise on the multilingual research team that we had in place for both components of the study. Wave 1 consisted of 2-hour survey sessions in large rooms at local community centres and neighbourhood houses. After the survey session, participants were asked to wear an accelerometer and GPS unit for one week to track both the intensity and location of their movement.
Organisational Considerations. Data collection for Wave 1 revealed several organisational considerations. First, we were not sure if we could conduct survey sessions in multiple languages in the same room at the same time. Being mindful of noise and privacy, we scheduled only two participants in the room for each appointment time. One-on-one measurement sessions were conducted at the South Vancouver Neighbourhood House for those who requested it. We also quickly learned that we needed additional items, not just study documents, translated – for example, wayfinding signage (see Figure 1) and labels on envelopes that said “please open and read”. We also required English labels to guide our research staff: for example, the research coordinator could not distinguish between Hindi and Punjabi script. We added English labels as “footers” to all study documents to indicate the version/language being used. In an English language study, we would typically assign and label participant IDs in advance (e.g., providing booklet 102 to participant ID 102); however, this was not possible when using documents in multiple languages. Accordingly, we took enough booklets in each language, and then assigned IDs as participants arrived and indicated their language preference. Many participants spoke several languages, and it was important not to make assumptions about which language they would prefer to use in a research setting. Using this method, we might assign ID 102 to a Mandarin-language participant package, and ID 103 to a Punjabi-language package.

Figure 1: Multilingual wayfinding signage
Survey Administration and Vocabulary Cards. We did not translate the survey booklet. Professionally translating the entire booklet, which was 60 pages, into five languages would have been cost-prohibitive. We also knew that some participants would have limited literacy, even with translated documents. Consequently, for each language, we had one RA consistently administer the survey sessions verbally. Each RA piloted their translation of the survey booklet prior to data collection by administering a copy of the booklet to an older adult volunteer who was not part of the study. After these pilots, we reconvened as a team to review any issues that arose related to translation. Two issues were raised by both research assistants. First, the term “walkable” did not readily translate. We decided as a team to use and translate the English phrase “a good place to walk” to replace “walkable”. Many participants, however, readily understood the concept of “walkable” in English, and translation was not necessary.
The second issue was that many built environment terms were difficult to translate. One example is “curb cut”. According to the Merriam-Webster Dictionary, a curb cut is “a ramp cut into a street curb at a corner for wheelchair access or at a driveway for vehicular access” (“Curb cut”, 2018). Of the surveys that we administered (see Tong et al., Reference Tong, McKay, Martin-Matthews, Mahmood and Sims-Gould2019), the Neighbourhood Environment Walkability Survey was the most difficult to translate, as it included many built-environment terms that are not necessarily part of everyday conversation. Problematic vocabulary included “curb cuts”, “cul-de-sacs”, and statements such as “There is a grass/dirt strip that separates the streets from the sidewalks in my neighbourhood.” To aid in the translation of this survey, we created visual vocabulary cue cards (see example in Figure 2). A professional photographer, who was also part of our research team, travelled to South Vancouver to take photos of the concepts to which these questions referred.

Figure 2: Sample vocabulary cue card
Take-home Booklets and the Role of Family Assistance. Of the 49 participants who completed the survey sessions, 48 agreed to take home an accelerometer and GPS unit to measure their physical activity and spatial mobility. We asked participants to wear these units for one week, during waking hours. Along with the units, we sent a take-home booklet that included instructions, visuals, and a daily log to track their wear time and pertinent notes (e.g., if they took a nap and removed the units mid-day; if they removed the units for swimming, etc.). We knew in advance that some participants would have limited literacy, even with translated booklets; however, we also knew that many of these participants co-resided with family members who could assist. To facilitate a role of family support, we typically sent home two versions of the take-home booklets, one in the participant’s first/preferred language, and one in English. We knew from our work with the SAC that some second- and third-generation relatives would be willing to help, and these individuals might have spoken Punjabi, Cantonese, and so on, but would not have been able to read or write in these scripts. Providing materials in multiple languages allowed family members to be of assistance when needed and desired by the participants.
Communication with the Research Team. Participants were keen to wear their accelerometers and GPS units correctly. With the aforementioned direct line of communication to RAs’ cellular phones, RAs received daily calls from participants. These telephone calls were often queries on how to correctly wear the accelerometers, what the lights on the units indicated, if they should still be wearing the units, how we wanted the units returned, and so on. This line of questioning led to a very high level of compliance, as reported in Tong et al. (Reference Tong, McKay, Martin-Matthews, Mahmood and Sims-Gould2019).
Data Collection — Wave 2: Interviews and Walking Interviews
Wave 2 consisted of in-depth interviews with 18 participants, and optional walking interviews with 13 participants. For more information on the interACTIVE interpreted walking interview method, see Tong et al. (Reference Tong, Sims-Gould and McKay2016).
Working with Professional Interpreters. In a multilingual study with limited resources, we chose to prioritise the cost of professional interpretation. Colleagues and peers who had conducted research with FBOAs advised us to employ professional interpreters if and when possible. Also, the SAC advised us to avoid the use of peer and/or volunteer interpreters, citing privacy concerns for participants. We worked with a local interpretation agency to contract two women – one who spoke English, Hindi, and Punjabi, and one who spoke English, Cantonese, and Mandarin – each with 10 years of experience. Although professional interpreters are expected and trained to insert themselves into interviews without preparation, we provided copies of the consent form, interview guide, and a summary of study objectives one week prior to our first interviews. Interpreters were allocated one hour of paid time to review materials prior to commencing data collection. We also met with interpreters one hour prior to the first interview, to review any questions, comments, or concerns.
Including the Interpreters as “Co-researchers”. In the interACTIVE walking interviews, the interpreter’s role evolved from that of translator to that of co-interviewer. In the seated interviews, the interpreters maintained their formal interpretation role. Both interpreters had experience working in health care and legal settings and were accustomed to scenarios in which their primary role is to find approximate word equivalence between two languages. The interACTIVE interviews, however, provided a less-prescribed format, and allowed the interpreters the opportunity to contribute to the discussion in different ways. In the dynamic mobile interviews, interpreters posed their own questions, initiated conversations, and contributed to group discussions. As often happens in multilingual contexts (Myers-Scotton, Reference Myers-Scotton1993), these conversations were typically conducted in several languages, sometimes combining English and the participant’s other languages in a single sentence. Participants’ English language abilities were highly varied; consequently, the role of the interpreter varied from interview to interview. For participants with very limited English, the interACTIVE interview still required thorough translation. Participants with stronger English skills were able to combine physical and visual cues in the environment – some English words or sentences, and some verbally translated discussions to convey their impressions of the local environment and their interactions with said space.
After each interview, the interpreter and interviewer had a 15- to 20-minute debriefing. In the debriefing, the interpreter and interviewer verbally reviewed the verbal content of the interACTIVE interview, co-reviewed the rough field notes for completeness, and the interpreters then offered their impressions of the interview. The content of the debriefing was added to the field notes that we took throughout Wave 2. As the interpreters became more accustomed to this method, and more familiar with our research objectives, they increased their level of participation beyond that of translator. At the end of the study, both interpreters expressed their appreciation for the opportunity to add their voices and their own questions to the interview.
Data Transcription and Analysis. Our research team had an established relationship with a reliable and efficient professional translation agency, but the transcribers worked only in English. The transcriber was instructed to transcribe only sections of the audio file that we had recorded in English. Professional interpreters translated both the interviewer’s questions and participants’ responses into English. This process relied on complete and faithful interpretation into English.
To ensure the quality of the transcribed interviews, multilingual RAs who were not present during the interviews were asked to review a random selection of transcripts (five interviews per assistant). Research assistants listened to the original audio files and compared them to final interview transcripts to ensure both faithful translation of the interview and faithful transcription of the English text. No major issues were reported. Minor omissions were recorded on the checked transcripts, and largely consisted of a missing word. One lengthy discussion about the divorce of one participant’s daughter was not fully translated. At the time, this was discussed with the interpreter who felt that the information was sensitive and not pertinent to the research questions. This was the only noted significant omission from interpretations and transcriptions. In short, when employing high-quality professional interpreters, it was possible to work with a monolingual, English-only transcriber.
Sharing the Results: A Multimodal Approach
At one of our first interviews, a participant expressed her frustration with previous research studies that she had participated in. She explained that her community had “been researched a lot”, but she didn’t feel that she ever received enough feedback from previous research teams. She felt that her community had been “used”. It was a priority of ours to ensure that participants felt that their involvement was valuable, appreciated, and would have an impact. We mailed a personalised, handwritten thank-you card to each participant immediately following data collection; RAs assisted with these notes. Within approximately four months, each participant received a personalised “mobility and physical activity report”. They received a full-colour copy in English, and a translated version in their preferred language. This report included their personal physical activity report from the accelerometers, a map of their mobility based on their GPS outputs, and a more global summary of high-level study findings. We produced a higher-level summary of the studying findings in English for the SAC and neighbourhood stakeholders.
Finally, approximately eight months after data collection we also held a half-day community forum at the South Vancouver Neighbourhood House, in which we shared study findings. Presentations were made in English, whereas work and discussions in smaller groups at tables were conducted in multiple languages, with the assistance of peer volunteers from the SAC translating as needed. The community forum was attended by approximately 40 stakeholders, including study participants and partners from the SAC and South Vancouver Neighbourhood House. In Figure 3, we have provided an overview of the project timelines and the documents and resources required at each phase to implement this mixed-methods, multi-language study.
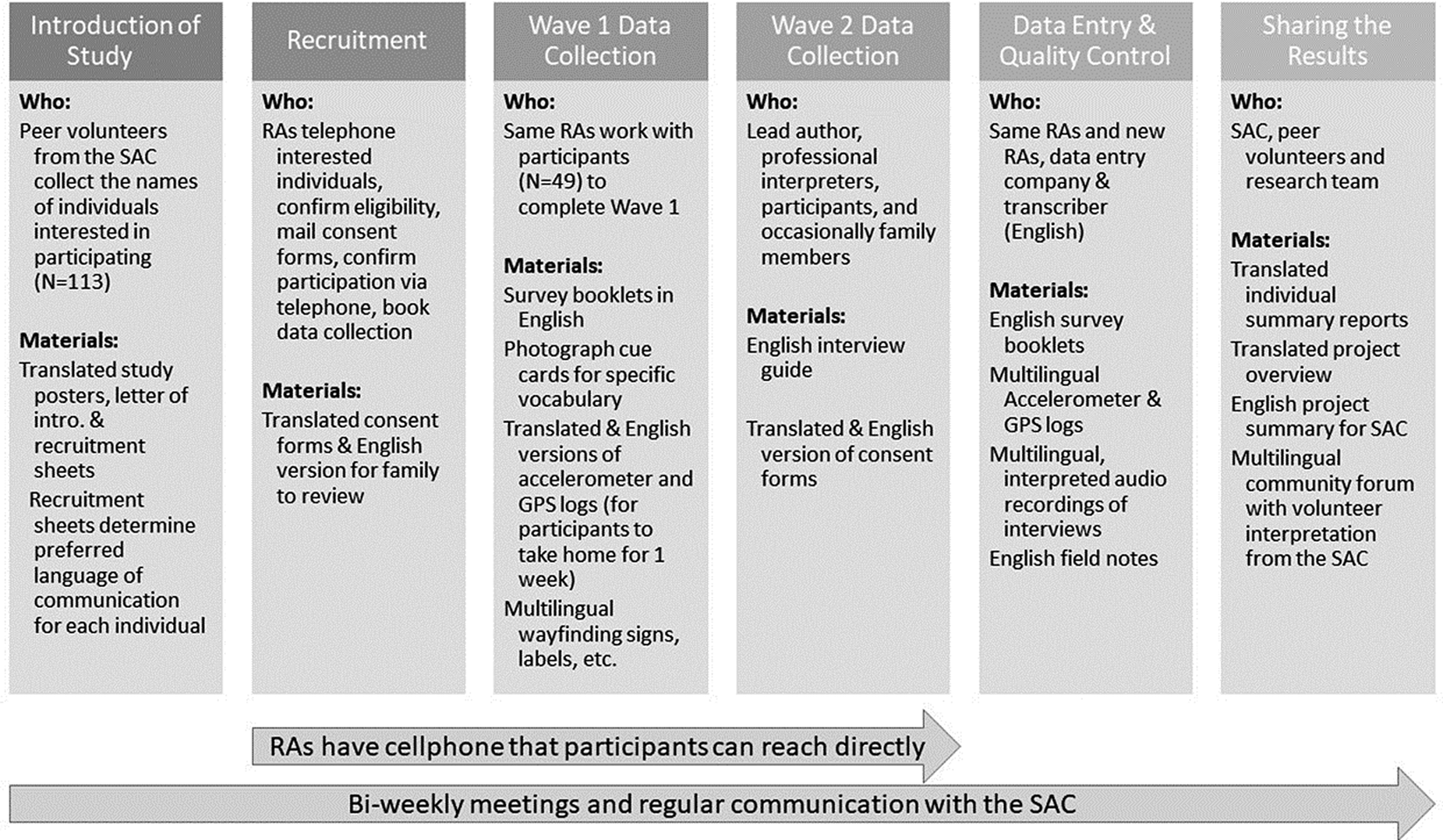
Figure 3: Study overview: Roles and multilingual materials
Discussion
We worked with the SAC for a year prior to commencing data collection (see Tong, Franke, Larcombe, & Sims Gould, Reference Tong, McKay, Martin-Matthews, Mahmood and Sims-Gould2017). Generally speaking, this level of “frontline” work, getting to know participants and partners, is not “always practical or enthusiastically pursued by researchers” (Sin, Reference Sin2004, p. 267). This high level of engagement with the SAC prior to data collection gave us important insights that allowed us to design an accessible study. We knew ahead of time, for example, that some participants would have limited literacy and that some participants would require assistance from co-residing family members who read and write in different languages. By sharing these “lessons learned” here, future researchers can learn from our process and they may also benefit from the concerns and recommendations raised in our intensive frontline work with the SAC. We summarise our key lessons in Table 2.
Table 2: Summary of key lessons learned

RA = research assistant
Some of the survey instruments that we used are available in other languages. For example, the Neighbourhood Environment Walkability Survey is available in traditional Chinese script (Cerin et al., Reference Cerin, Sit, Cheung, Ho, Lee and Chan2010). However, in the translation and validation of this survey for administration in Hong Kong, the instrument was changed to reflect life, habits, and the built environment in the ultra-dense urban metropolis of Hong Kong. Cerin et al.’s (Reference Cerin, Sit, Cheung, Ho, Lee and Chan2010) Neighbourhood Environment Walkability Survey for Chinese seniors is an admirable effort to tailor the instrument for use in an Asian context, but it is not appropriate for use with Chinese older adults living in Canada. A translated document is not sufficient; it also must be appropriate for the specific context in which data is being collected.
We did not professionally translate the entire survey booklet. Rather, we relied on consistent research assistants to translate the survey booklet in situ, as they administered it to participants. We also did not use “forward-and-back translation”, wherein documents are translated from one language into another, and are then re-translated by another translator, who is unfamiliar with the original content, back into the original language, to ensure equivalence between the original and translated versions. Forward-and-back translation has been the standard for decades, and this process is endorsed by the World Health Organization (2018) for translating of survey measures into other languages. Forward-and-back translation, however, is costly, time-intensive (Guillemin, Reference Guillemin1995), and often critiqued by translation professionals as superfluous and/or flawed (Ozolins, Reference Ozolins2009). We chose to focus our available resources on hiring the right people, with the right training and experience (Santos et al., Reference Santos, Black and Sandelowski2015) to ensure quality translation, professional interpretation, and to provide an accessible and meaningful experience for the FBOAs who participated in our study.
Conclusion
It has been encouraging to see a recent increase in research focused on foreign-born older Canadians (e.g., Curtis & Lightman, Reference Curtis and Lightman2017; Guruge et al., Reference Guruge, Thomson and Seifi2015; Koehn et al., Reference Koehn, Badger and Mullings2015; Wang et al., Reference Wang, Guruge and Montana2019), including here in the Canadian Journal on Aging. We have prepared this Research Note in the hope that it may support continued efforts in this area, in particular as it is projected that the ageing population will become increasingly diverse.





