



Introduction
Rarer dementias differ from typical dementias in that initial cognitive symptoms do not usually present as memory problems, and they are also more likely to occur before the age of 65 (Harvey et al., Reference Harvey, Roques, Fox and Rossor1996; Koedam et al., Reference Koedam2010; Rossor et al., Reference Rossor, Fox, Mummery, Schott and Warren2010). Rarer dementias are often misdiagnosed, with as many as 28% of patients given an incorrect psychiatric diagnosis (Woolley et al., Reference Woolley, Khan, Murthy, Miller and Rankin2011). Prevalence figures for rarer dementias are therefore difficult to establish; however, it is estimated that 3.9 million people worldwide are living with young-onset dementia (Hendriks et al., Reference Hendriks2021). The level of support received after diagnosis can be poor with carers facing difficulties in accessing appropriate information and services (Millenaar, Bakker, et al., Reference Millenaar, Bakker, Koopmans, Verhey, Kurz and de Vugt2016; Stamou et al., Reference Stamou2021). Potential challenges associated with a younger age of onset, such as childcare responsibilities, employment and income instability, and a lack of awareness in public, healthcare, and charitable sectors, can lead to an increased burden for carers (Bakker et al., Reference Bakker2013; Mayrhofer et al., Reference Mayrhofer2020).
Family carers take on a great deal of responsibility, with estimates suggesting that those caring for people with dementia represent a global equivalent of 40 million full-time workers (Wimo et al., Reference Wimo, Gauthier and Prince2018). Caring responsibilities are associated with increased depression, anxiety, stress, frustration, and grief, as well as reduced self-efficacy and low subjective well-being (Pinquart and Sörensen, Reference Pinquart and Sörensen2003). Carers of people with young-onset dementia experience lower quality of life and greater perceived difficulties (Millenaar, de Vugt, et al., Reference Millenaar2016; Hvidsten et al., Reference Hvidsten2020). Low self-esteem and low levels of satisfaction with social support are associated with increased depression and anxiety in carers of people with dementia (Crespo, et al., Reference Crespo, López and Zarit2005). Understanding the progression of dementia and associated emotional responses has the potential to reduce carer distress (Moore et al., Reference Moore2017). This evidence suggests that giving carers the opportunity to build social support, improve confidence, and explore their feelings could be beneficial in improving carer well-being.
Through the multiple, gradual losses, and profound changes that characterize dementia, it is possible to experience the loss of a loved one before they reach physical death. In a concept analysis by Lindauer and Harvath (Reference Lindauer and Harvath2014), the term predeath grief was coined to reflect the experience of grieving for someone with dementia, distinguished by the long and undefined trajectory of the condition, as well as compromised communication with a loved one and related changes in the relationship.
Studies suggest that between 47 and 71% of carers experience a grief reaction (Adams and Sanders, Reference Adams and Sanders2004; Collins et al., Reference Collins, Liken, King and Kokinakis1993; Diwan, et al., Reference Diwan, Hougham and Sachs2009; Sanders and Corley, Reference Sanders and Corley2003). Carers may not recognize their feelings as grief if they are experiencing disenfranchised grief, whereby their loss is not acknowledged by society or themselves (Doka, Reference Doka and Stroebe2008). One study found that 68% of carers reported grief, and those who did not report grief reported a strong sense of loss (Sanders and Corley, Reference Sanders and Corley2003). Predeath grief is associated with increased depression and carer burden, decreased emotional health, maladaptive problem-solving, and can also contribute to prolonged postdeath grief (Chan et al., Reference Chan, Livingston, Jones and Sampson2013; Lindauer and Harvath, Reference Lindauer and Harvath2014; Romero, et al., Reference Romero, Ott and Kelber2014).
Various interventions have been attempted to improve well-being for carers. Peer support, befriending, family support, online psychosocial modules, and support groups have reported mixed results with some indication of positive well-being outcomes (Czaja et al., Reference Czaja, Loewenstein, Schulz, Nair and Perdomo2013; Dam et al., Reference Dam, de Vugt, Klinkenberg, Verhey and van Boxtel2016; Marziali and Garcia, Reference Marziali and Garcia2011). A meta-analysis of studies trialing support groups found a positive impact on well-being, depression, and social outcomes, as well as a small impact on carer burden (Chien et al., Reference Chien2011). Several interventions have targeted predeath grief in carers of people with dementia and, although small in scale, show promising outcomes, such as a positive impact on grief, depression, anxiety, state of mind, resilience, empowerment, and self-efficacy (MacCourt et al., Reference MacCourt, McLennan, Somers and Krawczyk2017; Ott, et al., Reference Ott, Kelber and Blaylock2010; Paun and Cothran, Reference Paun and Cothran2019; Sanders and Sharp, Reference Sanders and Sharp2004). Qualitative findings from these studies suggest that interventions helped carers to identify, normalize, and process grief.
Existing predeath grief interventions have been designed primarily around the experience of those with typical late-onset and memory-led dementias and may not be appropriate or representative of the experiences of those caring for someone with a rarer form of dementia. The Road Less Travelled program was developed to help carers of people with rarer dementias to explore and acknowledge grief and loss and to process difficult emotions associated with these feelings.
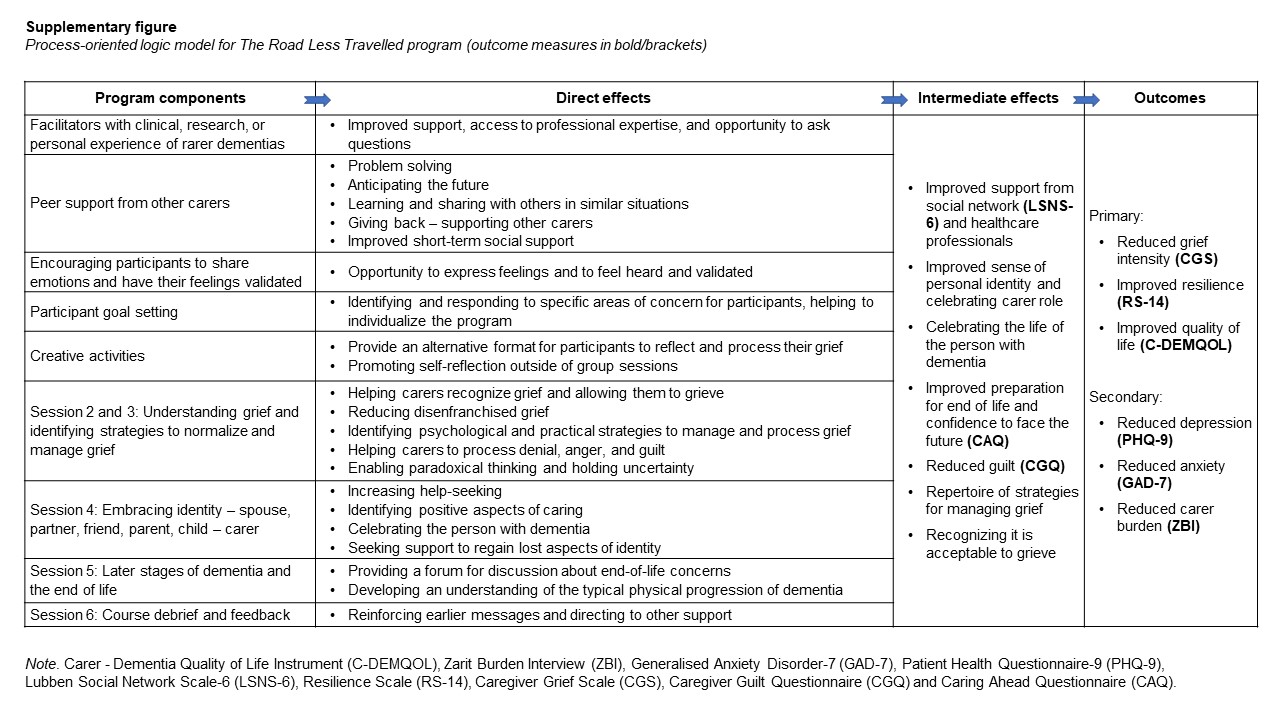
It was developed by Rare Dementia Support (RDS) and University College London (UCL), as part of the Rare Dementia Support Impact study (Brotherhood et al., Reference Brotherhood2020) in consultation with researchers, clinicians, and carers. It was embedded in existing literature and theories relating to predeath grief in dementia carers (Blandin and Pepin, Reference Blandin and Pepin2017; Doka, Reference Doka and Stroebe2008; Meuser and Marwit, Reference Meuser and Marwit2001; Moore et al., Reference Moore, Crawley, Vickerstaff, Cooper, King and Sampson2020). Carers and clinicians provided feedback on the format and content of the program to ensure it aligned with their personal and professional experiences. We incorporated this into a logic model (see Supplementary Material) theorizing how the program would impact carer grief and used this to inform the choice of outcome measures. The logic model links the program components with anticipated direct effects, intermediate effects, and broader outcomes.
While existing interventions exploring grief and loss have been shown to improve psychological outcomes for participants, discussions surrounding grief can be emotionally challenging for carers and could result in increased distress as they come to terms with their feelings of loss. It is therefore important to consider the impact that the program has on carer well-being as well as how acceptable and feasible it is. This study aims to evaluate the feasibility, acceptability, and impact on well-being of The Road Less Travelled program.
Method
Design
Using a mixed methods design, we conducted an exploratory pilot study of The Road Less Travelled program with a single group over a 6-month period. Quantitative data were collected from outcome measures at baseline (T1), post-intervention (T2), and 3 months post-intervention (T3). Qualitative data were collected from interviews with participants and facilitators at T2. The project was approved by the UCL Research Ethics Committee (reference no. 8545/004).
Recruitment
Carers of people with rarer dementias were invited to take part in the online program by an email sent to all members of the Rare Dementia Service. People interested in taking part were screened by service staff to ensure the program was suitable for them (for more information about recruitment, see Waddington et al., Reference Waddington2022).
Intervention
The Road Less Travelled program consisted of six 2-hour sessions held every 2 weeks from February to April 2021. The program was designed to be appropriate for carers at any stage of the caring journey either at home or in residential care. Sessions were hosted on the online meeting platform, GoToMeeting, and included: getting to know each other, exploring and understanding grief, adapting to loss and normalizing grief, embracing identity, later stages and end of life, and a program debrief. Participants were advised to contact one of the facilitators between sessions if they experienced any distress as a result of the content. A handbook was provided to participants with resources and information about the topics discussed, as well as independent activities that participants were encouraged to complete in their own time. These included creative activities such as writing a letter or drawing a line to represent their carer experience.
Measures
A record was kept of how many participants attended each session. Validated outcome measures (Table 1) were used to assess the impact of the program at three time points (T1, T2, and T3). The measures assessed quality of life, carer burden, depression, anxiety, social support, resilience, grief, guilt, and preparedness for end of life. At T2, participants were asked how they would rate the helpfulness of the program, on a four-point Likert scale ranging from “not helpful” to “very helpful”. They were also asked to rate how valuable they found different aspects of the program on a four-point Likert scale from “not at all” to “very”.
Table 1. Details of outcome measures

Qualitative interviews were conducted by RSN and SA 3–6 weeks after the end of the program using a semistructured interview guide of questions relating to participants’ experiences of the program. The two facilitators were interviewed separately by EG to gather their impressions of the program. Interviewers had not been involved in developing or facilitating the program.
Data analysis
Qualitative interviews were audio-recorded, transcribed, and analyzed in NVivo software using thematic analysis (Braun and Clarke, Reference Braun, Clarke, Cooper and tal2012). Using an inductive approach, key concepts were identified and used to formulate a coding framework by the analysis team. The analysis team included psychology graduates (RSN and SA), a PhD student (EG), and the program developers (KM and JW). KM is an experienced qualitative researcher with a psychology background and JW is an experienced dementia care nurse who also facilitated the program. The coding framework was applied to the transcripts in an iterative approach of revising and adding codes as necessary.
The questionnaire data were analyzed using Friedman tests with additional Wilcoxon signed-rank tests carried out when p < 0.05 and a trend was identified. One participant had missing data for 4 out of 22 items on the carer burden measure in both pre- and post-program measures, and carer burden scores have therefore been excluded for this participant. For other cases of missing data, the average score for the remaining items in the relevant scale or subscale was used.
Results
Participants
Nine carers based across the UK and Ireland participated (Table 2), exceeding our original recruitment target of eight people. Eight were recruited from an email sent to members of RDS. One additional participant was recruited after learning of the program through a family member who was also participating. Since this final participant was recruited later, they were unable to be included in the quantitative measures but were included in the qualitative interviews. In addition, the two facilitators of the program were interviewed. Both facilitators were female. The main facilitator had clinical experience of rarer dementias, and the second facilitator had personal experience as a carer of someone with a rare form of dementia.
Table 2. Details of carer participants at baseline

Note. During the course of the program, one person cared for at home was admitted to hospital and remained there throughout the program. The COVID-19 pandemic meant restrictions were in place at the time of the program limiting visitation to care homes and hospitals.
Qualitative findings: participant interviews
The findings from the thematic analysis for the participant interviews can be grouped into the themes of overall impressions, emotional processing, outlook, and social impact. Findings from the facilitator interviews are reported separately.
Overall impressions
Participants’ overall impressions of the program were overwhelmingly positive, and they described it as “invaluable”, “beneficial”, “worthwhile”, “important”, “well put together”, and “powerful”. When asked whether they thought the program should be offered to other carers, all participants felt that it should. All participants were happy with the length of the program and the frequency and duration of the sessions, as well as the size of the group.
None of the participants felt that having the sessions online substantially impacted their experience of the program. Many said that online sessions allowed them to fit attendance around their caring responsibilities more easily and that they would not have been able to attend all sessions in person. Some suggested that being in their own home may have encouraged people to open up as they were in a familiar environment.
Emotional processing
A common theme identified was having the opportunity to take the time to reflect on emotions, accompanied by thoughts about how self-reflection was difficult to achieve in a carer role:
“…the minute you don that carer’s hat you forget about yourself, you become less of a priority and sometimes dealing with your emotions and things, it’s easier not to deal with them and just carry on.”
(Participant 8)
One participant mentioned that having technical terms for concepts such as predeath grief had been helpful in putting labels on feelings they already knew they had. This was also mentioned by a participant who felt the program had helped them to recognize their emotions as grief:
“I think I’m more aware of it as grief. Sometimes grief can be channeled into anger or resentment. Then I’ve got to see it for what it is, but it’s a very complicated emotion.”
(Participant 7)
Alongside this deeper reflection on their emotions, several participants indicated feeling validated and more capable of accepting their emotions. One participant described how if they were feeling overwhelmed, they would imagine the faces and words of the group members validating their emotions. This feeling of self-validation was echoed by others.
“It has given me that breathing space to say, ‘I’m allowed to be hurting, and I’m allowed to be upset with myself and feel guilty,’ and all the rest of it”
(Participant 6)
Acceptance of emotions was stated by one participant to be the “biggest turnaround” from the program (Participant 8). Understanding the concept of predeath grief also helped with acceptance, as people felt more entitled to grieve, with one participant stating it gave “permission” for why they felt so terrible (Participant 3).
“I think it’s almost the whole societal thing of we only think of grief as being applicable if somebody has actually passed away. But actually feeling like I am entitled to say I’m grieving him has been the biggest thing and made me feel and think about grief very differently.”
(Participant 8)
Participants also mentioned how the program had helped to calm, soften, express, or “get rid of” feelings such as anger, frustration, and upset, remarking that sharing “lightens your load” and describing it as “cathartic”.
Alongside the positive emotional processing and comfort that group members reported, there were also moments of emotional discomfort experienced by almost all participants. Two participants reported coming away from the first session feeling emotionally drained, with one participant experiencing particular distress:
“I was really hysterical because it was just so much- And all those lovely people and all their emotions. Seven people had just dumped their lives at my feet. It was awful.”
(Participant 3)
Many remarked on how helpful it was to have the sessions 2 weeks apart, since this gave time to reflect and process the emotions raised. The emotional weight of the program was generally perceived as necessary to the processing they were going through:
“I think it forced a worsening of emotional well-being, to bring about a shift in me looking at things that need to be looked at. So, I got worse before I got better, but again that’s actually good. I don't see it as a bad thing at all.”
(Participant 7)
Outlook
Several participants made comments about how the program had helped them to see things from a different perspective and felt their outlook had been improved. Some felt the program had helped to separate the person from the disease, enabling them to reduce feelings of frustration. One participant also mentioned the independent activities in the program as particularly useful in thinking differently, describing them as a helpful “interjection” when people are “living inside their own heads quite a bit” (Participant 5).
Thinking about the future and preparations for the end of life brought about mixed feelings in the participants. For several, this seemed to have been helpful in a practical sense, providing the opportunity to think through the steps they would need to take and to hear from those who were further along in the caring journey. For others, it represented more of an emotional preparation in facing something they did not want to think about. For one participant, it brought up profound feelings of grief and they described the processing of this grief as having both positives and negatives. Several participants found this process difficult, while acknowledging it as necessary:
“I think it has given me a greater awareness of also what might be the future, because it’s something I didn't want to look at thank you, but it forced me to do that. I need to as well, yes.”
(Participant 7)
Participants also experienced a shift in the way they viewed and evaluated themselves as carers. Many mentioned feelings of guilt as a source of distress; however, the program had helped them become more forgiving and accepting in their appraisal of their caring role:
“We do the best we can, and that’s it. In childcare they have something called the ‘good enough parent.’ I call it the ‘good enough carer.’ That’s what I’m doing.”
(Participant 7)
One participant explained a direct effect that the program had on their feelings of guilt and attributed this to one of the independent activities which involved writing a letter about your feelings of loss and then writing a reply to this letter as if responding to a friend:
“And in writing that response, a little bit of a lightbulb went on and I thought, ‘Yes, why am I being so hard on myself, even with this whole feeling of guilt?’”
(Participant 8)
Increased confidence was mentioned by several participants. Examples of increased confidence included: participants’ ability to take difficult steps, such as opening up to their friends about their feelings, participants discussing grief openly with their children, and an increased belief in their ability to cope. Understanding predeath grief and feeling validated was also helpful to one participant who said they had previously viewed themself as simply not being able to cope with what was happening. For some, it also brought up thoughts about their identity outside of being a carer. In another ‘lightbulb moment’, one participant recognized how they had been sacrificing their own well-being:
“…the lightbulb moments were coming, saying, ‘Yes, you’re just running yourself into the ground. That’s no good for him, and it’s no good for you. You do need some time.’ And I realized other people in the group had a bit more personal time, and I was like, ‘Well, I’ve stopped doing everything.’”
(Participant 2)
Social impact
One of the most propounded benefits of the program was the opportunity to meet with others in a similar situation, as this was mentioned by every participant. The majority of participants mentioned feeling less alone, commenting on how isolating caring can be, and how reassuring it was to know others were having similar experiences.
“And what has also helped my well-being enormously is knowing that I’m not alone, that there are other people going through exactly the same, sometimes worse, sometimes better, but nonetheless, they can really empathize with the situation”
(Participant 8)
One of the aspects which seemed valuable to participants was not having to explain what they were going through or the feelings they were having, remarking on how similar others’ experiences and emotions were. This provided validation in knowing “you are not going mad” (Participant 3) and promoted a feeling of belonging.
“…it’s just so easy to talk to people that… You don't have to explain anything. You can say anything at all and they wouldn't be shocked. There’s no background needed.”
(Participant 1)
A few participants mentioned it was particularly helpful that others had experience of rarer dementias, voicing their frustration with most people’s misconceptions about their situation. Talking with others who understood the concept of predeath grief was also described as “one of the biggest highs” (Participant 8). Knowing that others were facing similar challenges seemed to give heart to some participants that they could “face anything” (Participant 4) knowing that others have done so. The chance to learn about possible challenges they may face in the future was mentioned as a valuable aspect of the program.
“I just learn so much from the people that have travelled this road.”
(Participant 4)
Most participants remained in contact after the end of the program. Many described the value of knowing there were people they could turn to who understood the situation. Some found this a source of comfort even without thinking they would reach out, with a participant mentioning that just imagining the group members’ faces makes them feel they are not alone.
“It’s a prop, knowing that there are people out there, should I be feeling the need, that I could turn to and say, ‘Look,’ or to share something with them. We have been keeping in contact.”
(Participant 6)
Qualitative findings: facilitator interviews
Overall, facilitators found the program feasible to deliver. They described the importance of being flexible with the sessions to allow people to discuss topics as they came up even if they were not planned. Giving people time and space to discuss their feelings was something the facilitators saw as key and commented on the benefits of allocating the first session to allow people to share their stories. This also provided the facilitators with the opportunity to get to know each participant well and allowed them to personalize sessions accordingly.
Facilitators commented on feeling very involved with the group, which could take an emotional toll, and highlighted the importance of providing support for the facilitators. Peer support and debriefing sessions which were made available for facilitators were recognized as helpful, since feeling responsible for the group members could feel overwhelming at times. They mentioned the importance of being clear from the start about what kind of help and support they would offer participants and recognizing when it would be appropriate to signpost to other services.
Quantitative findings
Across all sessions and participants, the attendance rate was 97.9%. The program was rated as “very helpful” by 73% of participants and “helpful” by 27% of participants. Figure 1 presents how the participants rated the value of different aspects of the program.

Fig. 1 The value of different aspects of the program to participants.
The results of the outcome measures for the impact of the program are presented in Figure 2, with statistical analyses reported in Table 3. The Friedman tests identified a trend in outcomes for quality of life, carer burden, and depression. Further analysis using Wilcoxon signed-rank tests for these three variables showed an improvement in quality of life and depression from T1 to T2 and T1 to T3. Carer burden increased at T3 compared to T1 and T2.

Fig. 2 Pre- and post-program scores for outcome measures.
Note. Outcome measures for (a) Patient Health Questionannaire-9 (PHQ-9), (b) Generalised Anxiety Disorder-7 (GAD-7), (c) Zarit Burden Interview (ZBI), (d) Caregiver Grief Scale (CGS), (e) Caregiver Guilt Questionnaire (CGQ), (f) Carer - Dementia Quality of Life Instrument (C-DEMQOL), (g) Lubben Social Network Scale-6 (LSNS-6), (h) Resilience Scale (RS-14), and (i) Caring Ahead Questionnaire (CAQ). Time point 1 = baseline, time point 2 = post-intervention, time point 3 = 3-month follow-up. Each line indicates an individual participant. In some cases, the y-axis does not start from zero and should be interpreted accordingly. On graphs (a) to (e) the y-axis has been reversed, so that a positive incline consistently represents an improved score.
Table 3. Analysis of outcome measures

Note. Asterisk (*) denotes when a higher score on the scale would indicate a better outcome. Measures included are Carer – Dementia Quality of Life Instrument (C-DEMQOL), Zarit Burden Interview (ZBI), Generalised Anxiety Disorder-7 (GAD-7), Patient Health Questionnaire-9 (PHQ-9), Lubben Social Network Scale-6 (LSNS-6), Resilience Scale (RS-14), Caregiver Grief Scale (CGS), Caregiver Guilt Questionnaire (CGQ), and Caring Ahead Questionnaire (CAQ).
Discussion
This study has found that The Road Less Travelled program was acceptable to carers and feasible to implement. Participants were enthusiastic about the benefits of taking part in the program, with the majority rating it as very helpful, and all felt that it should be offered to other carers. The number, duration, and frequency of sessions was considered appropriate by participants and was feasible to deliver. The online videoconferencing format did not present any challenges and was instrumental in allowing carers to attend. This is particularly important in rarer dementias where the smaller incidence means carers may be more geographically dispersed, as well as allowing those with caring responsibilities to balance their time more easily. Numerous aspects of the program were considered valuable by participants, including speaking to others in a similar situation who understood the experience of rarer dementias. Multiple improvements in well-being were reported in the qualitative interviews. The quantitative findings should be interpreted cautiously due to the small sample size. However, there are some promising findings in relation to decreased depression and increased quality of life across the course of the intervention.
This tallies with evidence from a meta-analysis of support groups for carers of people with dementia which found increased well-being and reduced depression (Chien et al., Reference Chien2011). At 3-month follow-up, improvements in depression and quality of life were sustained, suggesting a lasting effect or continued processing after the end of the program. Improvements in well-being occurred in spite of emotional discomfort experienced by some, and the benefit of working through difficult emotions seemed to have been recognized by participants. Most participants acknowledged that emotional processing was a necessary task which the program gave them the opportunity, time, and space to address, and that this would have been harder to achieve without this support. This reflects the previously reported finding that supporting carers to understand their emotional responses can help to reduce distress (Moore et al., Reference Moore2017).
Despite predeath grief being the primary target of the program, no uniform trend was discernible for a change in grief. Qualitative findings suggest that the program engendered an acceptance of grief, and it is possible that improvements in well-being are linked to accepting grief rather than reducing it. Other interventions have reported decreases in grief measures (MacCourt et al., Reference MacCourt, McLennan, Somers and Krawczyk2017; Ott, et al., Reference Ott, Kelber and Blaylock2010; Paun and Cothran, Reference Paun and Cothran2019); however, one reported that although only a small decrease was observed, qualitative findings suggested that participants felt their grief had been normalized (Sanders and Sharp, Reference Sanders and Sharp2004). A similar finding was identified in the qualitative interviews, where participants mentioned how useful it had been to accept and validate their feelings around grief and loss. In some cases, acknowledging grief may have had the opposite effect of making it felt more acutely.
The Dementia Grief Model (Blandin and Pepin, Reference Blandin and Pepin2017) posits that acceptance and acknowledgment can drive forward the processing of grief, whereas denial and avoidance can hinder it. This could be helpful in interpreting some participants’ reactions when faced with difficult emotions. Being able to accept emotions and prepare for the future was beneficial to many participants, while those who had previously reported avoidance of these issues found the subjects distressing or unsettling, despite acknowledging it was a necessary process.
The reassurance and comfort gained from mutual understanding were identified by participants as one of the most powerful and helpful aspects of the program. Many mentioned no longer feeling alone or as isolated, a finding that was similarly reported in another grief intervention (Paun and Cothran, Reference Paun and Cothran2019). Support groups have been shown to have positive impacts for carers of people with dementia (Chien et al., Reference Chien2011), and this was reflected in the findings that hearing the experiences of others was beneficial in providing validation, encouraging reflection, and enabling a shift in perspective. The observed decrease in depression could have been aided by the provision of beneficial social support, since low satisfaction with social support has been linked to increased depression in carers (Crespo, et al., Reference Crespo, López and Zarit2005).
Limitations and strengths
Several limitations to the study should be kept in mind. It was not always clear whether participants attributed certain changes directly to taking part in the program. Those most likely to benefit from a group program may have been more likely to volunteer to take part and may be more open to seeking out and receiving support. The small sample size makes it difficult to make inferences about outcome measures, and one participant was also not included in the outcome measures due to starting the program later. In addition, the sample was not culturally or ethnically diverse. The evaluation of the program involved those who developed and facilitated the program, potentially introducing bias in how findings were interpreted. To partly address this, interviews were conducted by researchers who were not involved in developing or facilitating the program.
A strength of the study was including a 3-month post-intervention follow-up to explore whether any effects endured over time, although the outcomes could be affected by other events. Facilitator interviews were also beneficial in corroborating the participants’ experience of the program in terms of feasibility and acceptability. The potential for emotional distress at points highlights the significance of the screening process for participants which ensured they were aware of difficult content that might have been experienced.
Future directions
These preliminary findings suggest this theoretically driven program is feasible and acceptable to carers and may benefit aspects of carer well-being. A larger scale pilot study could provide evidence for the effectiveness of the intervention and hosting multiple groups would enable the inclusion of a more diverse range of participants. It could also be trialed with carers of people living with more typical forms of dementia. Similar experiences of grief, loss, and diminished well-being could make this a valuable intervention for carers of people with different forms of dementia with minor adjustments. Further evaluation could be helpful to establish whether it would be beneficial to group members if they were all at a similar stage within their caring journey.
The experience of emotional discomfort in some sessions could also be explored further to establish whether this is a necessary component of examining feelings of grief. One aspect that became clear from the interviews was that discomfort was at times accompanied by feelings of progress or acceptance in the participants, making this a difficult process to conceptualize and evaluate. These findings illustrate the importance of having a skilled facilitator who is able to identify when carers are in need of additional support and may benefit from a referral to more individualized professional counseling. The results presented here capture a positive appraisal of how the program can impact well-being overall, and multiple aspects of the program were considered valuable by participants. Our logic model (see Supplementary Material) outlines the theorized mechanisms of how the program may influence carer well-being and provides a strong rationale for further testing. The findings are of potential value to healthcare professionals working with carers of people with rarer forms of dementia, with the indication that acceptance and peer support appear to be key aspects to consider in improving carer well-being.
Conclusion
The study has demonstrated that the program was feasible to implement and acceptable to carers. Evaluative data provides promise for the overall impact of the program on carer well-being. The processing of emotions did result in discomfort and distress for some participants, but it also appeared to be part of a process for acknowledging difficult emotions and finding acceptance.
Despite the small sample size, these initial findings provide justification for a larger-scale pilot study and for continuing and extending the program to reach more carers. Considering the significant impact that caring has on well-being, the particular challenges in caring for someone with a rarer dementia, and the implications for psychological and emotional health, establishing that The Road Less Travelled program has the potential to support and enhance carer well-being is of considerable benefit. This study was the first in the UK to test an intervention specifically targeting predeath grief for carers of people with rarer dementias. Framing the program around grief was conceptually helpful to participants and provides a promising avenue to improve carer well-being.
Conflicts of interest
None.
Source of funding
This work is part of the Rare Dementia Support Impact project (The impact of multicomponent support groups for those living with rare dementias, (ES/S010467/1)) and is funded jointly by the Economic and Social Research Council (ESRC) and the National Institute for Health Research (NIHR). ESRC is part of UK Research and Innovation. The views expressed are those of the author(s) and not necessarily those of the ESRC, UKRI, the NIHR or the Department of Health and Social Care. Rare Dementia Support is generously supported by The National Brain Appeal.
Description of authors’ roles
SJC is PI for the IMPACT study. EVB is responsible for IMPACT study program management. SJC and EVB managed the ethics application. JW and KJM researched and designed the intervention. JW, EVB, PMC, SJC, EH, RMJ, CW, and KJM contributed to research design and methodology. JW, EVB, SJC, EH, and KJM supervised data collection. JW and RMJ facilitated the intervention. RSN, SA, EH, SRH, RES, MVDBW, EVG, CW, and OW collected data. RSN, JW, and KJM prepared the manuscript and all authors critically reviewed and approved it.
Acknowledgments
Ali Rose Sisk (PhD student at Marie Curie Palliative Care Research department, University College London, London, UK) for her contribution to and review of session 5. Catherine Ader (Dementia Research Centre, Department of Neurodegenerative Disease, UCL Queen Square Institute of Neurology, University College London, London, UK) for the design of the handbook. Nuriye Kupeli (Senior Research Fellow at Marie Curie Palliative Care Research Department, Division of Psychiatry, University College London, London, UK) for her contribution to the compassionate writing exercises.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1041610223000236







 Open access
Open access