



INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative condition that is associated with cognitive and functional decline. Evidence to date suggests that Black and Latino older adults are twice and 1.5 times as likely to have AD compared to White older adults (Alzheimer’s Association, 2021; Tang et al., Reference Tang, Cross, Andrews, Jacobs, Small, Bell, Merchant, Lantigua, Costa, Stern and Mayeux2001). However, there are mixed findings on the rates of AD among Latino older adults with data showing higher risk in Latinos from the east coast (primarily Caribbean Hispanics), but not in Latinos from the west coast (primarily Mexican Americans) (Haan et al., Reference Haan, Miller, Aiello, Whitmer, Jagust, Mungas, Allen and Green2007; Mehta & Yeo, Reference Mehta and Yeo2017; Tang et al., Reference Tang, Cross, Andrews, Jacobs, Small, Bell, Merchant, Lantigua, Costa, Stern and Mayeux2001). It is important to understand factors that might contribute to racial/ethnic differences in AD. This includes biological factors as well as sociocultural factors including cultural differences and factors adversely impacting minority groups such as lower socioeconomic status, health inequalities, and less access to health care.
Although the apolipoprotein E ϵ4 (APOE ϵ4) allele is linked to increased risk of AD and cognitive decline, reported prevalence rates of the APOE ϵ4 allele across racial/ethnic groups varies across studies, though some studies suggest that there may be a higher prevalence of ϵ4 among Black older adults (Weuve et al., Reference Weuve, Barnes, Mendes de Leon, Rajan, Beck, Aggarwal, Hebert, Bennett, Wilson and Evans2018) and lower prevalence among Latino older adults (Campos, Edland, & Peavy, Reference Campos, Edland and Peavy2013) compared to White older adults. Importantly, the effects of the APOE ϵ4 allele across racial/ethnic groups is not well understood at this time. Some studies report a weaker effect of APOE ϵ4 status on AD risk among Black and Latino groups compared to Whites older adults (Campos et al., Reference Campos, Edland and Peavy2013) while other studies have shown a similar effect (Tang et al., Reference Tang, Stern, Marder, Bell, Gurland, Lantigua, Andrews, Feng, Tycko and Mayeux1998; Weuve et al., Reference Weuve, Barnes, Mendes de Leon, Rajan, Beck, Aggarwal, Hebert, Bennett, Wilson and Evans2018). There is also limited research on the influence of APOE ϵ4 on continuous measures of cognitive decline over time across racial/ethnic groups, although the limited data with Black individuals shows a similar pattern of decline in memory compared to White individuals (Barnes et al., Reference Barnes, Arvanitakis, Yu, Kelly, De Jager and Bennett2013). While some studies report that ϵ4 is associated with higher risk of cognitive impairment and dementia among Latino individuals, these studies do not examine APOE ϵ4 effects on pattern of cognitive decline across domains of cognition in Latino older adults. It is important to delineate the effect of APOE ϵ4 on cognitive trajectories since decline is a more specific marker of brain disease and is less related to non-brain variables (e.g., education level, cultural background, sociodemographic factors, etc.) that can have strong associations with one time cognitive measurements. Furthermore, to understand the impact of APOE ϵ4 on cognition within a specific group, it is important that we consider both prevalence and magnitude of effect of ϵ4 within a group. Given the limited research and largely unknown effects of APOE ϵ4 on cognition among diverse groups, further research in this area is essential.
The goals of this study were to: (1) evaluate the prevalence of APOE ϵ4 among Black, Latino, and White older adults, (2) evaluate the differential effects across these groups of APOE ϵ4 status on baseline level and change over time of cognitive outcomes, and (3) evaluate the combined impact of prevalence of APOE ϵ4 and magnitude of its effect on cognitive decline within each racial/ethnic group. Examining both prevalence and effect size of APOE ϵ4 on cognitive decline is important for understanding differential risk for cognitive decline across racial/ethnic groups (i.e., overall impact of APOE ϵ4 within a group will likely be larger if the prevalence of ϵ4 is higher and the effect of ϵ4 is greater).
METHODS
Participants
Participants were from the UC Davis Diversity Cohort, a longitudinal study that includes substantial numbers of self-identified Latino, Black, and non-Latino White older adults. This cohort is heterogeneous in race, ethnicity, educational and occupational attainment, and socioeconomic and cognitive status. Participants were recruited through (1) a community outreach and screening program designed to identify and recruit individuals with cognitive functioning representative of the community dwelling population in a six-county catchment area in the central Sacramento/San Joaquin valley and east San Francisco Bay area of Northern California and (2) memory/dementia clinics (Hinton et al., Reference Hinton, Carter, Reed, Beckett, Lara, DeCarli and Mungas2010). All participants signed informed consent, and all human subject involvement was overseen by the institutional review board.
All participants received multidisciplinary diagnostic evaluations at baseline and at approximately annual intervals following the baseline evaluation. Baseline and follow-up evaluations followed the same protocol with a detailed medical history, physical and neurological exam, clinical neuropsychological assessment, routine dementia work-up laboratory tests (e.g., Vitamin B12, thyroid stimulating hormone (TSH), rapid plasma regain (RPR), etc.), and neuroimaging (1.5T or 3T structural brain MRI including T1 weighted, T2 weighted, and FLAIR images). A family member or other informant was interviewed to obtain information about cognitive and independent functioning. Clinical neuropsychological tests were different from the cognitive measures used in analyses in this study to estimate cognitive trajectories.
Diagnosis of cognitive syndrome (normal, mild cognitive impairment (MCI), Dementia) and, for individuals with dementia, underlying etiology, was made in a multidisciplinary consensus conference following standardized criteria and methods. Dementia was diagnosed using DSM-III-R (American Psychiatric Association, 1987) criteria for dementia modified such that dementia could be diagnosed in the absence of memory impairment if there was significant impairment of two or more other cognitive domains. MCI was diagnosed according to standard clinical criteria and was further sub-typed into amnestic MCI or non-amnestic MCI, single or multiple-domain (Petersen, Reference Petersen2004; Morris et al., Reference Morris, Weintraub, Chui, Cummings, Decarli, Ferris, Foster, Galasko, Graff-Radford, Peskind, Beekly, Ramos and Kukull2006). Normal cognitive function was diagnosed if there was no clinically significant cognitive impairment. All diagnoses were made blind to the neuropsychological tests that were analyzed in this study.
The study consisted of 584 participants with APOE genotype and two or more cognitive assessments. There was variability in the number of evaluations completed by each individual due to a rolling enrollment; however, all baseline cognitive assessments were standardized. There were 297 White (51%), 138 Latino (24%), and 149 Black (26%) participants; 74 Latino participants (13%) were tested in Spanish, and all others were tested in English. Sample characteristics are presented in Table 1.
Table 1. Sample characteristics. (BL = Black, LA = Latino, WH = non-latino white)
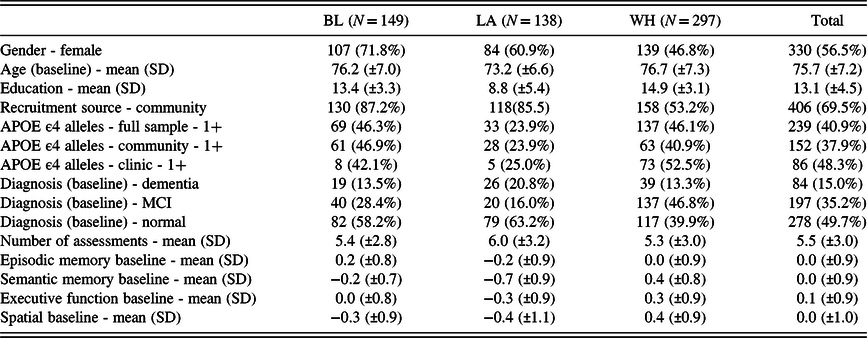
Variables that differed significantly by race/ethnicity include: gender, recruitment source, baseline age, education, diagnosis, prevalence of one or more APOE ϵ4 allele, and all baseline cognitive scores.
Cognitive Assessment
The cognitive outcomes in this study were measures of episodic memory, semantic memory, executive function, and spatial ability derived from the Spanish and English Neuropsychological Assessment Scales (SENAS). The SENAS has undergone extensive development (Mungas et al., Reference Mungas, Reed, Marshall and González2000, Reference Mungas, Reed, Crane, Haan and González2004) as a battery of cognitive tests relevant to cognitive aging (Carmichael et al., Reference Carmichael, Mungas, Beckett, Harvey, Tomaszewski Farias, Reed, Olichney, Miller and Decarli2012; Early et al., Reference Early, Widaman, Harvey, Beckett, Park, Farias, Reed, Decarli and Mungas2013; Fletcher et al., Reference Fletcher, Gavett, Harvey, Farias, Olichney, Beckett, DeCarli and Mungas2018; Gavett et al., Reference Gavett, Fletcher, Harvey, Farias, Olichney, Beckett, DeCarli and Mungas2018; Mungas et al., Reference Mungas, Gavett, Fletcher, Farias, DeCarli and Reed2018) that allow for valid comparisons across racial, ethnic, and linguistic groups (Brewster et al., Reference Brewster, Melrose, Marquine, Johnson, Napoles, MacKay-Brandt, Farias, Reed and Mungas2014; Melrose et al., Reference Melrose, Brewster, Marquine, MacKay-Brandt, Reed, Farias and Mungas2015; Mungas et al., Reference Mungas, Reed, Haan and González2005; Mungas, Reed, Farias, DeCarli, Reference Mungas, Reed, Farias and DeCarli2005; Mungas et al., Reference Mungas, Widaman, Reed and Tomaszewski Farias2011; Mungas et al., Reference Mungas, Beckett, Harvey, Farias, Reed, Carmichael, Olichney, Miller and DeCarli2010).
Item response theory and confirmatory factor analysis methods were used to construct Spanish and English Neuropsychological Assessment Scales (SENAS) measures that are psychometrically matched across domains in terms of level of reliability across the ability continuum. Importantly, these measures do not have floor and ceiling effect and are normally distributed. The episodic memory score is derived from a multi-trial 15-item word-list-learning test (Mungas et al., Reference Mungas, Reed, Crane, Haan and González2004). The semantic memory measure is a composite of highly correlated verbal (object-naming) and nonverbal (picture association) tasks. The executive function composite is constructed from component tasks of category fluency (animals, fruits, vegetables), phonemic (letter) fluency, and working memory (digit-span backward, visual-span backward, list sorting). Spatial ability was measured using the SENAS Spatial Localization scale which assesses ability to perceive and reproduce two-dimensional spatial relationships that are increasingly complex. Language of test administration was determined by an algorithm that combined information regarding each participant’s language preference in several specific contexts (e.g., conversing at home, listening to radio or television, conversing outside the home, preferred language for reading). Each domain was z-standardized using the full baseline sample mean and standard deviation (mean of 0 and standard deviation of 1, range = −4 to 4).
APOE genotyping
Apolipoprotein E (APOE) genotyping was carried out using the LightCycler ApoE mutation detection kit (Roche Diagnostics, Indianapolis, IN). APOE ϵ4 prevalence (carrier status) was based on absence or presence of ≥1 APOE ϵ4 allele. Allele frequencies were also computed for each ethnoracial group and subgroup of interest.
Data Analysis Measures and Data Processing
SENAS measures of episodic memory, semantic memory, executive function, and spatial ability were measures of longitudinal change in cognition. Each of these four cognitive variables was transformed using the Blom inverse normal rank order transformation (Blom, Reference Blom1958) in order to normalize these variables and establish a common scale (mean = 0, SD = 1). Presence versus absence of the APOE ϵ4 allele was the primary independent variable. Covariates included age at baseline evaluation, education, gender, recruitment source, loss of follow-up due to death, and loss to follow-up for other reasons.
Longitudinal Modeling of Cognitive Trajectories
Mixed effects, parallel process longitudinal analyses were performed using MPlus version 8.2 multilevel modeling (Muthen & Muthen, Reference Muthen and Muthen1998). In the within part of this model, each of the four cognitive outcomes was regressed on time in study. This generated person- specific intercept (in reference to cognitive baseline) and linear slope (in reference to cognitive change) random effects for each outcome. These random effects then served as dependent variables in the between part of the model.
We utilized multiple group models to evaluate racial/ethnic group similarities and differences in effects of APOE and covariates on cognitive baseline and change components. In multiple group analyses, models are estimated for each group and specific parameters, APOE ϵ4 effects for example, can either be constrained to be equal across groups or can be freely estimated within groups. Less constrained models are compared to nested, more constrained models to determine if fit is significantly better when the parameters of interest are allowed to differ across groups. The likelihood ratio test for nested models (Satorra & Bentler, Reference Satorra and Bentler2001; Satorra & Bentler, Reference Satorra and Bentler2010) was used to determine if freely estimating specific parameters across groups resulted in significantly better model fit to the data.
RESULTS
Sample Characteristics
Sample characteristics are presented in Table 1, stratified by race/ethnicity group. About 57% of the sample were female participants. Black and Latino participants were more likely to be females but White participants were evenly divided among males and females (χ 2[2] = 26.654, p = .001). Approximately two thirds of the sample were recruited from the community (69%). Recruitment source differed by race/ethnicity (χ2[2] = 77.789, p = .001), with White participants more likely to be clinic referrals. Average age was about 76 years and this differed across groups (F[2,581] = 11.975, p = 0.001) with Latino participants being about 3 years younger at the baseline assessment than Black and White participants. Average education was 13.1 years and differed across groups (F[2,581] = 120.216, p = .001), with Latino participants having substantially less education. Average number of cognitive assessments was 5.5 and did not differ across groups. Eighty-three percent had three or more assessments and 54.5% had five or more. The average time between assessments was 1.0 year.
About 15% were diagnosed with dementia at the first assessment, 35% had mild cognitive impairment (MCI), and 50% were cognitively normal. Diagnosis differed by race/ethnicity (χ 2[4] = 41.851, p = .001) with Whites more likely to have a diagnosis of MCI and less likely to be cognitively normal. ϵ4 was significantly related to baseline diagnosis (X-squared = 21.214, df = 2, p-value = 2.475e–05). See Table 5.
Prevalence of one or more APOE ϵ4 differed across groups (χ 2[2] = 21.631, p = .001); Latino participants had roughly half the ϵ4 prevalence (24%) of Black (46%) and White (46%) participants. In the entire sample, there are 23 ϵ4 homozygotes (2 Black, 2 Latino, and 19 White participants), with a much higher prevalence in White participants. White participants recruited through clinic had higher APOE ϵ4 prevalence than community recruits and this difference was not significant, but it approached significance (χ 2[1] = 3.506, p = 0.061). ϵ4 prevalence did not differ by recruitment source for Black or Latino participants. Baseline cognitive test scores all differed across race/ethnicity groups (p’s < .001). For episodic memory, Black participants had higher average baseline scores than White participants whose scores were higher than Latino participants. For semantic memory and executive function, the pattern was White > Black > Latino participants, and for spatial ability it was White > Black ≈ Latino participants.
Covariate Effects
We first estimated whether covariate effects on the intercepts (cognitive baseline) and slopes (change) of the four cognitive outcomes differed across groups. The effects of loss to follow-up on cognitive baseline (p = .001) and deceased status on cognitive change (p = .001) significantly differed across groups and were allowed to differ across groups in subsequent models. None of the other covariates had significantly different effects on cognitive baseline or change (p’s > .25).
APOE Effects
APOE effects in the full, combined sample are presented in Table 2. APOE had robust associations with cognitive change but limited associations on baseline scores. Episodic memory, semantic memory, and executive function all declined faster in participants with ≥1 ϵ4 allele and the magnitude of the APOE effects on change in these domains was very similar. Spatial ability change was also significantly related to APOE, but the magnitude of this effect was approximately half of that for the other three cognitive domains. Episodic memory baseline score was one-fourth standard deviation lower in those who were ϵ4 positive, but other baseline scores were not affected by APOE.
Table 2. APOE effects on cognitive baseline (intercepts) and change (slopes) in the full sample combining blacks, Latinos, and whites participants

Note: Tabled values are unstandardized regression weights (βs) with standard errors and p-levels. Results show estimates of APOE variable effects of ≥1 APOE ϵ4 allele versus 0 ϵ4 alleles on cognitive intercepts and slopes by racial/ethnic group. Estimates are SD units of cognitive composite scores. (+ p < .05, ++ p < .015, +++ p < .001)
Table 3 shows freely estimated effects of APOE on cognitive trajectory components in the three racial/ethnic groups. For slopes, presence of ≥1 ϵ4 allele was associated with faster decline of episodic memory and executive function in all three groups. ϵ4 was associated with faster semantic memory decline in Latino and White participants and was associated with spatial decline only in White participants. The ϵ4 effect on semantic memory significantly differed across groups (p = .042) but ϵ4 effects did not differ across groups for episodic memory (p = .975), executive function (p = .391), or spatial ability (p = .28). Pairwise comparisons performed to test differences in ϵ4 effects on sematic memory change (slope) showed that this effect was significantly larger for White participants in comparison with Black participants (p = .005) but the Black participant-Latino participant (p = .295) and Latino participant-White participant (p = .196) differences were not significant.
Table 3. APOE effects on cognitive baseline (intercepts) and change (slopes) by racial/ethnic group. Results show effects of presence of ≥1 APOE ϵ4 allele versus 0 ϵ4 alleles. BL = Black, LA = Latino, WH = non-latino white

Note: Tabled values are unstandardized regression weights (βs) with standard errors and p-levels. Results show estimates of APOE variable effects of ≥1 APOE ϵ4 allele versus 0 ϵ4 alleles on cognitive intercepts and slopes by racial/ethnic group. Estimates are SD units of cognitive composite scores. (+ p < 05, ++ p < .015, +++ p < .001).
APOE associations with cognitive baselines were less robust. ϵ4 was associated with a lower average baseline episodic memory in White participants and with a lower baseline executive function in Latino participants. Pairwise comparisons showed that the APOE effect on baseline episodic memory significantly differed only for Black participants compared with White participants (p = .001). The ϵ4 effect on executive function did not significantly differ across the three groups (p = .587).
Model predicted trajectories for ϵ4 positive and negative individuals within the three groups for two cognitive outcomes, episodic memory and semantic memory, are presented in Figure 1. This figure shows clear baseline differences in episodic memory between ϵ4 positive and ϵ4 negative White participants but smaller difference for Black and Latino participants, and small APOE related differences in baseline semantic memory. Episodic memory change (slopes) for ϵ4 positive individuals are quite similar across racial/ethnic groups, as are the slopes for ϵ4 negative individuals. In contrast, there is progressively greater divergence of ϵ4 positive and ϵ4 negative trajectories over time across for semantic memory from Black participants to Latino participants to White participants.

Figure 1. Trajectories of Episodic Memory and Semantic Memory by APOE ϵ4 Status and Race/Ethnicity - APOE Effects Freely Estimated.
Combined Effects of APOE ϵ4 Prevalence and Impact
Figure 2 shows how APOE ϵ4 prevalence and the impact of ϵ4 when present jointly contribute to cognitive trajectories. We used results from this study to calculate expected semantic memory trajectories for four hypothetical groups with varying ϵ4 prevalences and ϵ4 effect sizes: (1) no ϵ4, (2) low ϵ4 prevalence and moderate effect size, (3) high ϵ4 prevalence and moderate ϵ4 effect size, and (4) high ϵ4 prevalence and strong ϵ4 effect size.

Figure 2. Trajectories of semantic memory by APOE ϵ4 prevalence and ϵ4 effect size. Modest APOE effect is effect observed in single group model (semantic memory slope = −0.053, intercept =−0.027). Strong effect is effect observed for Whites in multiple group model: slope = −0.071, intercept = −0.150. Prevalences correspond to observed prevalences for Latino (0.24) and White (0.46) groups. Note. We used the estimated semantic memory intercepts and slopes for ϵ4 negative and ϵ4 positive individuals from the single group, combined sample model along with results from the multiple group analysis to derive expected semantic memory trajectories for four hypothetical groups: 1) no ϵ4 - based on the semantic memory intercept and slope for the no ϵ4 group in the single group model, 2) low ϵ4 prevalence (24% - equivalent to that observed in Latino group) and moderate ϵ4 impact (−0.053 SD/year - effect observed in the single group model), 3) high ϵ4 prevalence (46% - equivalent to that observed in Black and White groups) and moderate ϵ4 impact (−0.053 SD/year), and 4) high ϵ4 prevalence and strong ϵ4 impact (−0.071 SD/year - observed effect for Whites in multiple group model).
This figure demonstrates several salient points. First, absence of ϵ4 (hypothetical group 1) is associated with relatively stable semantic memory over time. Second, semantic memory decline is greater when prevalence of ϵ4 within a group is non-zero (groups 2, 3, and 4 compared to group 1), and higher prevalence is associated with faster decline when the impact/e4 effect size is the same (group 2 vs. group 3). Third, greater ϵ4 impact is also associated with faster decline when e4 prevalence is the same (group 3 vs. group 4). Overall, ϵ4 will have a minimal impact on late life cognition in a population if its prevalence is low and its impact when present is low. As prevalence and impact increase they have additive effects that jointly contribute to cognitive decline.
Secondary Analyses
We performed a secondary analysis in which baseline clinical diagnosis (cognitively normal vs. MCI vs. dementia) was added as a covariate to the primary multiple group model. The pattern of results was similar but APOE effects were attenuated (see Table 4). For White participants, APOE continued to be associated with changes in episodic memory, semantic memory, and executive function, and effect sizes for semantic memory (−.055) and executive function (−.059) were about 25% higher than for episodic memory (−.046). The APOE effect on episodic memory in Black participants continued to be strong (−.054), but APOE was not significantly related to decline in other cognitive domains for Black participants or to decline in any domain for Latino participants.
Table 4. APOE effects on cognitive baseline (intercepts) and change (slopes) by racial/ethnic group, adjusting for clinical diagnosis as a covariate. Results show effects of presence of ≥1 APOE ϵ4 allele versus 0 ϵ4 alleles. BL = Black, LA = Latino, WH = non-latino white, += p < .05, ++= p < 015, +++= p < .001)

Table 5. APOE status and cognitive diagnosis

We also examined the effects of number of ϵ4 alleles in full sample analyses. The number of ϵ4 was robustly associated with cognitive decline, but the incremental impact of a second ϵ4 was statistically significant only for executive function. We did not have adequate cell sizes to look at effects of ϵ4 homozygosity within racial/ethnic groups, specifically Black and Latino participants. However, among White participants, a second ϵ4 allele had no incremental impact on episodic memory change, but had a clear and statistically significant impact on executive function. Having a second ϵ4 allele had an impact on semantic memory (i.e., increases the ϵ4 effect by 70%), but it was not statistically significant (p = .27). Interestingly, when examining the overall ϵ4 effect, it was substantially reduced when ϵ4–4 cases were removed from the Black and Latino groups, whereas the effect for White participants remained as strong when ϵ4–4 cases were removed. The reduced ϵ4 effect in the Black and Latino groups after excluding ϵ4–4 cases suggest that ϵ4 may have a strong dose-dependent relation with cognition, but the small number of homozygous ϵ4 in these groups makes it difficult to interpret these results.
Summary of Results
Latino participants had roughly half the prevalence of ϵ4 carriers (24%) compared to Black (46%) and White (46%) participants. APOE ϵ4 showed robust relations to cognitive change (slopes) in all four domains in the full sample, but was related only to baseline performance for episodic memory, and not to baseline performance in other domains. APOE ϵ4 had a strong and equal effect on episodic memory change across the three groups, but its effect on semantic memory change followed a graded pattern: White > Latino > Black. A similar graded pattern was observed for executive function change, but these differences were not significant. APOE ϵ4 had limited effects on cognitive baselines, and was significantly associated only with episodic memory in White participants and executive function in Latino participants. When controlling for baseline clinical diagnosis (cognitively normal vs. MCI vs. dementia), we still found a very similar pattern of results although APOE effects were attenuated. Cognitive trajectories were influenced in an additive manner both by ϵ4 prevalence for a group and its effect size within the group.
DISCUSSION
Results showed a complex pattern of similarities and differences in the association of APOE ϵ4 with late life cognitive trajectories across Black, Latino, and White older adults. APOE ϵ4 had a strong and equivalent association with episodic memory decline in all three groups. Salient differences were that (1) APOE ϵ4 prevalence in Black and White participants was nearly double that of Latino participants, (2) ϵ4 had a larger association with semantic memory decline in White participants, (3) ϵ4 association with decline of non-episodic memory cognitive variables was smaller in Black participants, and (4) ϵ4 was related to baseline episodic memory only in White participants. Importantly, our findings do not seem to be explained by the groups differing in degree of cognitive impairment at baseline given that our sensitivity analysis controlled for baseline diagnosis. The main e4 pathway to cognitive decline is through brain changes resulting from ϵ4 related diseases like AD and CVD. Controlling for diagnosis should effectively remove a substantial part of the disease mediated pathway from APOE to cognition, consequently resulting in smaller e4 effects after adjusting for diagnosis.
The literature on racial/ethnic differences in the APOE association with cognitive decline has been largely confined to comparisons of White and Black groups and results have been mixed. Our findings that APOE ϵ4 is associated with cognitive decline in both Black and White participants is consistent with other studies comparing these two groups (Fillenbaum et al., Reference Fillenbaum, Landerman, Blazer, Saunders, Harris and Launer2001; Kaup et al., Reference Kaup, Nettiksimmons, Harris, Sink, Satterfield, Metti, Ayonayon and Yaffe2015; Knopman et al., Reference Knopman, Mosley, Catellier and Coker2009; Rajan et al., Reference Rajan, Barnes, Wilson, Weuve, McAninch and Evans2019; Sawyer, Sachs-Ericsson, Preacher, & Blazer, Reference Sawyer, Sachs-Ericsson, Preacher and Blazer2009). Our finding that the APOE association with episodic memory decline was the same in Black and White participants, while APOE had a stronger association with non-episodic memory decline in White participants is consistent with Barnes et al. (Reference Barnes, Arvanitakis, Yu, Kelly, De Jager and Bennett2013).
Results of this study showing APOE associations with cognitive decline in Latino older adults are novel and address a major knowledge gap. Latino participants in this study had roughly half the ϵ4 prevalence of Black and White groups, consistent with other studies that have reported lower ϵ4 prevalence in Latino individuals, especially in those with native American genetic ancestry. As depicted in Figure 2, ϵ4 prevalence and ϵ4 impact both contribute to expectancies for cognitive decline. The implication of lower ϵ4 prevalence in Latino older adults is that APOE is a less salient part of the pathway to cognitive decline in Latino individuals regardless of whether APOE has a similar effect when present.
There were also racial/ethnic groups differences in prevalence of homozygous ϵ4 carriers, which was higher in whites. Unfortunately, we could not systematically examine homozygous versus heterozygous e4 effects in Black and Hispanic participants due to cell size issues. There is evidence that homozygosity could contribute to domain specific effects in White participants, that is, there was an incremental effect of a second allele on executive function, but not on episodic memory, with a possible, intermediate effect on semantic memory (not reaching statistical significance).
Cognitive decline is multiply determined, and social cultural factors may modify the impact of biological factors like APOE. Results of this study raise questions about whether pathways from APOE to cognitive decline differ by race and ethnicity. APOE is a well-known risk factor for AD but is also a risk factor for vascular disease (Haan & Mayeda, Reference Haan and Mayeda2010) and perhaps other non-AD disease processes, and so can affect cognition through both AD and non-AD pathways. It is relevant to distinguish between episodic memory and non-memory cognitive abilities because episodic memory is strongly and selectively influenced by damage to a limbic, medial temporal circuit involving structures including the hippocampus and entorhinal cortex, whereas non-memory cognitive abilities are more dependent on neocortical structures and circuits. See Figure 3 for conceptual model of AD and non-AD pathways from APOE to cognitive decline. Relevant questions underlying racial/ethnic differences in APOE effects on cognition include: (1) Is APOE differentially related to AD and non-AD pathologies across ethnoracial groups? (2) Are AD and non-AD differentially related to cognitive decline in different groups?, and (3) Do AD and non-AD pathways differentially impact specific cognitive domains across groups?

Figure 3. Conceptual model of AD and non-AD pathways from APOE to cognitive decline.
This study did not measure underlying disease states and so cannot directly address questions about whether APOE is differentially related to AD across groups. Some previous studies on Black-White group disparities show equal risk for AD in these groups in ϵ4 positives but 2–4 times increased risk for AD in Black individuals for ϵ4 negatives (Tang et al., Reference Tang, Stern, Marder, Bell, Gurland, Lantigua, Andrews, Feng, Tycko and Mayeux1998; Weuve et al., Reference Weuve, Barnes, Mendes de Leon, Rajan, Beck, Aggarwal, Hebert, Bennett, Wilson and Evans2018), and a meta-analysis identified a stronger association of APOE with AD in White individuals (Farrer et al., Reference Farrer, Cupples, Haines, Hyman, Kukull, Mayeux, Myers, Pericak-Vance, Risch and van Duijn1997). Collectively, these studies suggest that ϵ4 is less salient for AD risk in Black individuals, and conversely, that non-APOE factors are more important. A recent biomarker study showed lower CSF Tau and p-Tau levels in ϵ4 positive Black participants in comparison with ϵ4 positive White participants (Morris et al., Reference Morris, Schindler, McCue, Moulder, Benzinger, Cruchaga, Fagan, Grant, Gordon, Holtzman and Xiong2019), which may possibly reflect a differential effect of APOE ϵ4 on underlying AD mechanisms (i.e., molecular biomarkers) with a weaker link between APOE and AD mechanisms in Black individuals. Our finding of lower prevalence of ϵ4 in Latino participants also suggests that APOE is less salient for cognitive decline in this group and that the APOE to AD pathway is less important than in White participants. Finally, although APOE ϵ4 is linked to increased risk of AD and cognitive decline, not all older adults with AD have APOE ϵ4 alleles, highlighting the importance of understanding other sociocultural and biological variables that impact late-life cognitive health.
One hypothesis to explain our results is that AD is more strongly linked to APOE in White participants so that AD pathology is more advanced, on average, in ϵ4 positive White participants than in Black and Latino participants. There is a large body of evidence that AD selectively affects episodic memory early in the disease course when neurofibrillary pathology is confined to the medial temporal lobes, and then impacts non-memory cognition when pathology spreads to neocortex (Nelson, Braak, & Markesbery, Reference Nelson, Braak and Markesbery2009). Differential impact of the APOE to AD to cognition pathway could explain the group differences in effects of APOE on non-memory cognition in this study, but the equal effects on episodic memory would imply that non-AD pathways to episodic memory are more salient in the minority groups. APOE also is associated with vascular disease (Schilling et al., Reference Schilling, DeStefano, Sachdev, Choi, Mather, DeCarli, Wen, Høgh, Raz, Au, Beiser, Wolf, Romero, Zhu, Lunetta, Farrer, Dufouil, Kuller, Mazoyer, Seshadri and Debette2013), and previous studies have shown that APOE ϵ4 can modify the effects of cerebrovascular disease on cognitive outcomes and dementia risk. Memory impairment is most often associated with medial temporal lobe neurodegeneration in the elderly, but can also result from white matter disease affecting the uncinate and inferior longitudinal fasciculi (Lockhart et al., Reference Lockhart, Mayda, Roach, Fletcher, Carmichael, Maillard, Schwarz, Yonelinas, Ranganath and Decarli2012).
This study has important limitations. First, the sample is essentially a sample of convenience. While there was considerable effort to recruit a sample that is representative of the respective communities in northern California (Hinton et al., Reference Hinton, Carter, Reed, Beckett, Lara, DeCarli and Mungas2010), it is important to evaluate the generalizability of our findings to other samples and other methods. Our sample of Latino participants was predominantly of Mexican and Central American origin, and may well not represent other Latino subgroups who have different cultural and genetic ancestry backgrounds.
Additionally, clinical recruits, who were more likely to have MCI, constituted a larger percentage of White participants in our sample. Thus, our sample of White participants may not necessarily represent the general White population in the United States and could effectively enrich the White group for clinically apparent cognitive decline and presence of AD pathology. While this could contribute to greater average cognitive decline in White participants, it wouldn’t explain a stronger association of APOE with decline of non-episodic memory abilities in white participants nor the equivalent APOE effect across groups on episodic memory decline. Second, the sample size is relatively small for evaluating what essentially are race/ethnicity by APOE ϵ4 interaction effects. The lack of statistically significant differences across racial/ethnic groups in APOE effects on executive function change may reflect limitations of statistical power. Third, sample size limitations precluded us from examining specific combinations of APOE alleles among these groups. These limitations suggest a need for replication within different, larger, representative samples that include Latino participants from different backgrounds. It is important for future, larger studies to address ϵ4 dose effects that could not be examined in this study. Additional limitations include the use of dated diagnostic criteria, and lack of robust data regarding dementia etiology.
This study also has strengths. It addresses a major knowledge gap by comparing APOE effects in three well characterized racial/ethnic groups. The study sample was heterogenous with respect to APOE genotype, clinical characteristics, and cognitive trajectories. This heterogeneity facilitates finding relevant associations with cognitive decline. We measured cognitive decline across multiple domains using psychometrically matched measures on the SENAS which were carefully constructed to avoid floor and ceiling effects (Mungas et al., Reference Mungas, Reed, Crane, Haan and González2004). There was considerable longitudinal follow-up that enabled separation of APOE effects on baseline cognition from effects on longitudinal change.
Further research is needed to clarify the mechanisms by which APOE affects disease processes and ultimately late life cognitive decline in diverse older persons. Studies that directly measure disease biomarkers along with cognitive trajectories in large and representative samples of racially/ethnically diverse older adults are particularly relevant to answering questions about how racial/ethnic diversity influences cognitive decline and dementia. A better understanding of the complex pathways underlying cognitive decline is important not only for understanding dementia in these specific groups but also for elaborating the multiple, complex determinants of cognitive decline and dementia that transcend racial and ethnic differences.
Acknowledgments
We would like to acknowledge the devotion of the participants in this study who volunteered their time for comprehensive annual evaluations and repeated MRI scans. Many staff of the UC Davis Alzheimer’s Disease Center made this study a reality. Esther Lara supervised all aspects of study implementation from participant recruitment through retention over time leading to successful longitudinal follow-up.
FINANCIAL SUPPORT
This work was supported by multiple grants from the National Institute on Aging (NIA) (P30 AG10129, R01 AG021028, and R01 AG047827, C DeCarli, PI; R01 AG10220, D Mungas, PI; R01/RF1 AG031563, B Reed/D Mungas, PI; R01 AG031252, S Tomaszewski Farias, PI).
CONFLICTS OF INTEREST
The authors have nothing to disclose.








