


The psychopathology that characterises the three DSM–IV eating disorder diagnoses – anorexia nervosa, bulimia nervosa and eating disorder not otherwise specified (American Psychiatric Association, 1994) – is distinctive and largely shared (Reference Fairburn and HarrisonFairburn & Harrison, 2003; Reference Fairburn, Cooper and ShafranFairburn et al, 2003). The close relationship between the diagnoses is further emphasised by the phenomenon of diagnostic crossover over time (Reference Fairburn and HarrisonFairburn & Harrison, 2003; Reference Fairburn, Cooper and ShafranFairburn et al, 2003; Reference Nielsen and PalmerNielsen & Palmer, 2003). Although such diagnostic flux is well known to clinicians, it has received limited research attention (Reference Sullivan, Bulik and CarterSullivan et al 1996; Reference Bulik, Sullivan and FearBulik et al, 1997; Reference Keel, Fichter and QuadfliegKeel et al, 2004). In particular, it has not been examined in relation to movement between all three eating disorder diagnoses. The aim of our study was to examine diagnostic change across the eating disorders using a prospective design and standardised diagnostic methods that employed clinical thresholds.
METHOD
Participants and procedure
The study was approved by the research ethics commission of the canton of Zurich. All participants received detailed information about the study, and gave written informed consent. Recruitment took place over 24 months (March 1997 until March 1999). The inclusion criteria were a current DSM–IV diagnosis of an eating disorder, age 17–50 years, ability to speak German, and female gender. In total 277 women with an eating disorder of clinical severity were recruited: 64 were consecutive patients in the eating disorder in-patient unit of the University Hospital Zurich, 57 were consecutive out-patients of the department of psychiatry of the University Hospital Zurich and 30 were recruited through contacts with eating disorder self-help groups in the Zurich area; an additional group of 126 participants with an eating disorder were enrolled through advertisements in local newspapers.
These participants were followed up 12 months and 30 months after the baseline evaluation. On each occasion they were invited for the follow-up interview in writing. Those who did not respond were contacted again in writing up to three times and repeated attempts were also made to establish contact by telephone. Ten participants who did not participate in a face-to-face interview at the second follow-up assessment were interviewed by telephone, a procedure that has been shown to be an acceptable alternative when diagnosing Axis I and II disorders (Reference Rohde, Lewinsohn and SeeleyRohde et al, 1997).
Almost three-quarters (74%) of the participants (n=205) were reassessed 12 months after baseline, of whom 192 were also reassessed at 30 months (69% of the baseline sample). One participant died during the course of the study. The proportion of participants who were reassessed did not differ significantly between the three DSM–IV eating disorder diagnostic categories of anorexia nervosa, bulimia nervosa and eating disorder not otherwise specified (EDNOS). However, non-participation was associated with younger age (z=2.5, P=0.012) and a shorter duration of eating disorder (z=3.3, P=0.001). Comparisons of participants recruited through the different sources indicated that the groups differed in age (Kruskal–Wallis χ2=31.2, d.f.=3, P<0.001) and duration of eating disorder (χ2=23.7, d.f.=3, P<0.001) with those recruited from the in-patient unit being the youngest (mean age 23.5 years, s.d.=5.8) and those with the shortest eating disorder duration (mean 6.4 years, s.d.=4.7), followed by those recruited as out-patients (mean age 27.1 years, s.d.=7.2; mean disorder duration 10.4 years, s.d.=7.3). Participants recruited through self-help groups (mean age 31.3 years, s.d.=7.3; mean disorder duration 14.7 years, s.d.=8.6) and newspaper advertisements (mean age 30.8 years, s.d.=8.1; mean disorder duration 13.1 years, s.d.=8.6) were older and had a longer duration of eating disorder.
The 192 participants who took part in both follow-up assessments comprised 55 women with anorexia nervosa (mean body mass index (BMI) 15.3 kg/m2, s.d.=1.5), 108 with bulimia nervosa (mean BMI 21.7 kg/m2, s.d.=4.0) and 29 with EDNOS (mean BMI 22.4 kg/m2, s.d.=6.3). Twentynine (53%) of the anorexia nervosa cases were of the restrictive subtype and 26 (47%) were of the binge–purge subtype. Of the bulimia nervosa cases, 103 (95%) were of the purging subtype and 5 (5%) of the non-purging subtype. The characteristics of the EDNOS group were as follows: 1 (3%) met all the diagnostic features of anorexia nervosa except amenorrhoea; 8 (28%) met all the features of bulimia nervosa except the frequency or duration criteria. Other forms of EDNOS were present in 20 participants (69%) – binge-eating disorder and ‘mixed’ states (Reference Fairburn and BohnFairburn & Bohn, 2005), in which the features of eating disorders were combined in a way that differed from anorexia nervosa and bulimia nervosa but were of clinical severity.
The mean age of the participants at study entry was 28.6 years (s.d.=7.9), with those with anorexia nervosa (mean age 26.6 years, s.d.=7.4) and bulimia nervosa (mean age 28.9 years, s.d.=8.1) being younger than those with EDNOS (mean age 31.6 years, s.d.=7.3); z=2.9, P=0.004 and z=2.2, P=0.032, respectively. The average age at onset of the eating disorder was 17.1 years (s.d.=4.1) and this did not vary between the diagnostic groups. The duration of eating disorder of the anorexia nervosa cases (mean 9.3 years, s.d.=7.2) was shorter than that of the bulimia nervosa cases (mean 11.7 years, s.d.=8.0) and the EDNOS cases (mean 14.4 years, s.d.=9.4); z=2.0, P=0.041 and z=2.4, P=0.015, respectively.
During the course of the study 88% of participants who completed the study (n=169) made contact with out-patient treatment providers and 34% (n=65) received in-patient treatment; 11% (n=21) received neither out-patient nor in-patient treatment.
Assessments
Eating disorders were diagnosed using the German version of the Structured Clinical Interview for Axis I of the DSM–IV (SCID; Reference Wittchen, Zaudig and FydrichWittchen et al, 1997), conducted by four psychologists (interrater reliability k=0.8) who had no contact with the participants other than the interviews for the study. In line with DSM–IV principles, a diagnosis of EDNOS was given if eating disorder features were present and resulted in a clinical degree of physical or psychosocial impairment yet the state did not fulfil diagnostic criteria for anorexia nervosa or bulimia nervosa (Reference Fairburn and BohnFairburn & Bohn, 2005). The European Cooperation in the Field of Scientific and Technical Research COST Action B6 structured interview (European Commission Directorate-General Science, Research and Development, 2005) was used to assess participants’ eating disorder features, history and secondary impairment. At each follow-up assessment the procedure for making the eating disorder diagnoses was the same as that used at the baseline. At all three time points every eating disorder diagnosis was checked by a psychiatrist who had extensive experience in evaluating patients with eating disorders (G.M.). In addition, at each assessment an interview was used to identify any treatment contact made in connection with the eating disorder, either before or during the study.
Statistical analyses
The data were analysed using descriptive procedures and w2 tests. The variables age, duration of eating disorder and age at onset were skewed and thus were analysed using non-parametric tests (Kruskal–Wallis and Mann–Whitney U tests). All tests were two-tailed and the minimum alpha level was set at 5%.
RESULTS
A subset of 192 participants had complete data-sets (i.e. they were assessed at all three time points). Their baseline diagnoses were as follows: 28.6% (n=55) anorexia nervosa, 56.3% (n=108) bulimia nervosa and 15.1% (n=29) EDNOS. Table 1 shows the distribution of their diagnoses at the two follow-up points classified by baseline diagnosis.
Table 1 Eating disorder diagnoses at 12-month and 30-month reassessments classified by baseline diagnosis
| Diagnosis at baseline | n | Diagnosis at 12-month follow-up | Diagnosis at 30-month follow-up | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anorexia nervosa | Bulimia nervosa | EDNOS | No eating disorder | Anorexia nervosa | Bulimia nervosa | EDNOS | No eating disorder | ||||||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | ||
| Anorexia nervosa | 55 | 31 | (56.4) | 9 | (16.4) | 10 | (18.2) | 5 | (9.1) | 27 | (49.1) | 5 | (9.1) | 11 | (20.0) | 12 | (21.8) |
| Bulimia nervosa | 108 | 7 | (6.5) | 55 | (50.9) | 20 | (18.5) | 26 | (24.1) | 6 | (5.6) | 40 | (37.0) | 29 | (26.9) | 33 | (30.6) |
| EDNOS | 29 | 5 | (17.2) | 7 | (24.1) | 8 | (27.6) | 9 | (31.0) | 4 | (13.8) | 1 | (3.4) | 9 | (31.0) | 15 | (51.7) |
| Total | 192 | 43 | (22.4) | 71 | (37.0) | 38 | (19.8) | 40 | (20.8) | 37 | (19.3) | 46 | (24.0) | 49 | (25.5) | 60 | (31.3) |
Remission from an eating disorder
There was considerable diagnostic instability. Taking the sample as a whole (i.e. all those with a DSM–IV ‘eating disorder’), only 55 participants retained the same diagnosis across all three assessment points, representing 28.6% of the whole sample (or 32.9% when cases with a stable remission at the two follow-up assessments were excluded). In part this instability was due to remission, although overall the remission rate was low. In all, just 20.8% (n=40) of participants were in remission at the 12-month follow-up (i.e. they had no clinical eating disorder), this figure increasing to 31.3% (n=60) at the 30-month assessment. The remission rates at both points varied significantly between the three diagnostic categories (χ2=7.1, d.f.=2, P=0.029; χ2=8.0, d.f.=2, P=0.019, respectively), with those with EDNOS having the highest remission rate (31% and 52% at the first and second follow-up points respectively), followed by those with bulimia nervosa (24% and 31%) and anorexia nervosa (9% and 22%). However, remission was not a stable state, either; of the 40 participants who were in remission at 12 months, less than two-thirds (n=25) were in remission at the second follow-up. Just 13% (n=25) of the sample were in remission at both assessment points.
Migration between eating disorder diagnoses
Although remission from an eating disorder was not common, migration between the eating disorder diagnoses occurred in over half the cases. Thus, taking the sample as a whole, but excluding those who no longer had an eating disorder at one or both follow-up points, 62 (53%) crossed over from one eating disorder diagnosis to another. This diagnostic migration was evident in all three diagnostic groups. Thus, of the 55 individuals with an initial diagnosis of anorexia nervosa, only 31 (56%) retained the diagnosis at 12 months and just 27 (49%) still had the diagnosis at 30 months. Twenty-three participants with an initial diagnosis of anorexia nervosa (48%) retained this diagnosis at both reassessments. Change in eating disorder diagnosis was even more evident among those with bulimia nervosa. Of the 108 participants with bulimia nervosa at baseline, only 55 (51%) had this diagnosis at the first reassessment and just 40 (37%) had it at the second. Only 29 (27%) of the women with an initial bulimia nervosa diagnosis retained this diagnosis at both reassessments. Diagnostic instability also characterised those with EDNOS. Of the 29 participants with EDNOS at baseline, just 8 (28%) still had the diagnosis at 12 months and 9 (31%) at 30 months, and only 3 (10%) had EDNOS at both reassessments. The rate of retention of an anorexia nervosa diagnosis was similar for the two subtypes of anorexia nervosa (restrictive subtype: first follow-up n=17, 57%, second follow-up n=14, 48%; binge–purge subtype: first follow-up n=14, 54%, second follow-up n=13, 50%). With regard to crossover between eating disorder diagnoses, marginally more anorexia nervosa cases changed to bulimia nervosa (20%, n=11) at either or both follow-up points than vice versa (9%, n=10); χ2=3.7, d.f.=1, P=0.053. Overall, 37% (n=60) of the participants with a baseline diagnosis of anorexia nervosa or bulimia nervosa were given a diagnosis of EDNOS at either or both follow-up points, a rate that did not differ between the two original diagnoses.
Change of diagnosis (including remission to no eating disorder) could theoretically have occurred in 384 instances (n=19262). In order to examine the dynamics of diagnostic change, we assessed the frequency of all possible changes. Figure 1 illustrates the identified patterns. Stability of diagnosis was highest for anorexia nervosa, followed by bulimia nervosa and then EDNOS. Bulimia nervosa showed fluctuation, both to and from the other eating disorder diagnoses and to and from the ‘no eating disorder’ category. The least stable diagnosis was EDNOS.
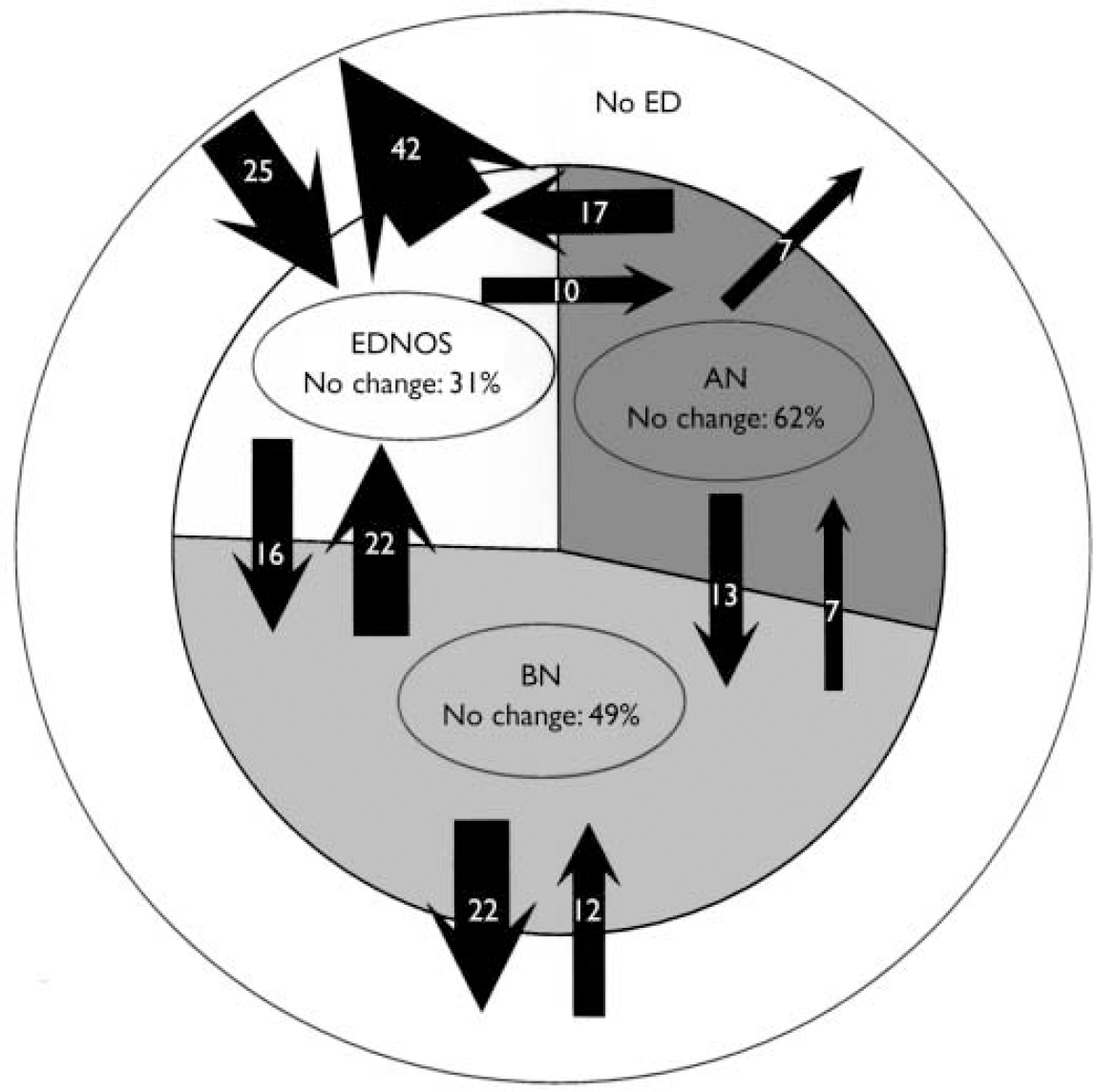
Fig. 1 Changes in DSM–IV eating disorder diagnoses over 30 months (AN, anorexia nervosa; BN, bulimia nervosa; EDNOS, eating disorder not otherwise specified). The figure illustrates changes of diagnoses on instance (rather than person) level. The areas in the pie chart represent the frequencies with which the respective eating disorder diagnoses occurred during all three assessment times; of all such diagnoses 28.4% were AN, 47.3% BN and 24.4% EDNOS. Figures in arrows are percentages based on the number of possible changes for each diagnosis.
Illness duration and diagnostic stability
Table 2 shows the duration of eating disorder at study entry for each diagnosis broken down by diagnosis at 30-month follow-up. For those who had anorexia nervosa, eating disorder duration was associated with retention of the diagnosis at 30 months (χ2=9.3, d.f.=3, P=0.026); specifically, women who retained their diagnosis had a significantly longer eating disorder history at study entry than those who were in remission at 30 months (z=3.0, P=0.002). Similarly, women with a baseline diagnosis of anorexia nervosa who showed a stable remission (no eating disorder at both reassessments) had a shorter history (mean 1.8 years, s.d.=1.5) at study entry than those who did not experience a remission at either or both time points (mean 9.9 years, s.d.=7.2; z=2.8, P=0.002) and than those who retained an anorexia diagnosis at both follow-up points (mean 8.6 years, s.d.=7.2; z=2.6, P=0.007). Those with bulimia nervosa or EDNOS showed no association between eating disorder duration and either change in diagnosis or stable remission. Also, no association emerged between age at onset of the eating disorder and change in diagnostic status, either in the whole sample or within any of the three diagnostic categories.
Table 2 Eating disorder duration at study entry classified by baseline eating disorder diagnosis and diagnosis at 30-month reassessment
| Diagnosis at baseline | Total at study entry | Diagnosis at 30-month follow-up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Duration (years) mean (s.d.) | Anorexia nervosa | Bulimia nervosa | EDNOS | No eating disorder | |||||
| n | Duration (years) mean (s.d.) | n | Duration (years) mean (s.d.) | n | Duration (years) mean (s.d.) | n | Duration (years) mean (s.d.) | |||
| Anorexia rervosa | 55 | 9.3 (7.2) | 27 | 11.0 (6.7) | 5 | 8.2 (7.2) | 11 | 10.6 (9.5) | 12 | 4.6 (4.3) |
| Bulimia nervosa | 108 | 11.7 (8.0) | 6 | 7.8 (5.1) | 40 | 12.4 (7.8) | 29 | 12.2 (8.9) | 33 | 11.1 (8.0) |
| EDNOS | 29 | 14.4 (9.4) | 4 | 13.8 (8.5) | 1 | 8.0 (–) | 9 | 14.7 (7.8) | 15 | 14.8 (11.0) |
| Total | 192 | 11.4 (8.1) | 37 | 10.8 (6.6) | 46 | 11.8 (7.7) | 49 | 12.3 (8.8) | 60 | 10.7 (8.9) |
Treatment contact
Participants’ therapeutic experiences were classified into out-patient treatment contact (psychotherapist, psychologist, psychiatrist or general practitioner) or in-patient treatment contact (psychiatric or psychotherapeutic in-patient unit or day clinic, or a general hospital). At baseline almost all participants had made some contact with out-patient treatment providers because of their eating disorder (97%, n=186). Almost half (49%, n=94) had received in-patient treatment. Only six participants (3%) had received no treatment at all. During the course of the study 88% of participants (n=169) made contact with out-patient treatment providers and 34% (n=65) received in-patient treatment; 11% (n=21) received no treatment. Treatment contact (out-patient v. no out-patient treatment, in-patient treatment v. no in-patient treatment) before study entry or during the study was not associated with stable remission (i.e. no eating disorder diagnosis at both follow-up assessments) either in the whole sample or within the diagnostic subgroups.
Purging behaviour
Participants’ diagnoses at all three assessment points were classified as either purging or non-purging, using the DSM–IV threshold frequency of purging behaviour (vomiting or use of laxatives) occurring at least twice a week. When no eating disorder was diagnosed at follow-up, the state was classed as non-purging. At baseline, 58 (30.2%) diagnoses were classified as non-purging and 134 (69.8%) as purging. After excluding the 25 individuals who experienced a stable remission (i.e. no eating disorder diagnosis at both follow-up assessments), analyses showed that 53.7% (n=65) of 121 participants with a baseline purging eating disorder received at some point (first and/or second follow-up) a non-purging non-purging diagnosis, whereas of 46 participants with a non-purging eating disorder at baseline 17.4% (n=8) subsequently received a purging diagnosis (χ2=17.9, d.f.=1, P<0.001). When considering the rates of stable remission, participants with a non-purging type of disorder at baseline had a significantly higher recovery rate (21%, n=12) than participants with a purging type of disorder (10%, n=13; χ2=4.3, d.f.=1, P=0.038).
DISCUSSION
This study focused on change in eating disorder diagnoses over time, a phenomenon that has received little systematic attention. Its aim was to track over a 30-month period the changes in eating disorder diagnosis in a large sample of clinical cases, noting especially movement between the three DSM–IV eating disorder diagnoses.
Diagnostic instability
There were three main findings. First, diagnostic stability was low. Just a third of participants retained their original diagnosis over the 30 months, when cases with a stable remission were excluded. Second, this was only in part due to remission, since the remission rate was low across all three diagnostic categories and stable remission was unusual (13%). This is of note because this was a naturalistic follow-up study, with 89% of participants having contact with treatment providers. The finding is consistent with the widely held view that eating disorders are self-perpetuating and difficult to treat (Reference Fairburn and HarrisonFairburn & Harrison, 2003), a view that is further bolstered by the fact that the remissions observed were often temporary, with a subsequent return of the eating disorder. The third finding is perhaps the most striking. It is that although the overarching diagnosis of ‘eating disorder’ was relatively stable, there was considerable flux between the three specific eating disorder diagnoses. Indeed, change in diagnosis occurred in over half the cases. All three eating disorder diagnoses showed this tendency. Anorexia nervosa was the most stable diagnosis, followed by bulimia nervosa and then EDNOS. Interestingly, prior course only predicted outcome in anorexia nervosa, where length of history was positively associated with greater diagnostic stability.
There is much published research on the outcome of anorexia nervosa and bulimia nervosa, but few studies have investigated the course of EDNOS or examined it as a possible outcome of anorexia nervosa or bulimia nervosa (Reference Fairburn and BohnFairburn & Bohn, 2005). This is important because recent studies suggest that EDNOS is comparable in severity to the two main eating disorder diagnoses and is often preceded by them (Reference Fairburn and BohnFairburn & Bohn, 2005). The studies on the outcome of bulimia nervosa have produced findings similar to ours. For example, Bulik et al (Reference Bulik, Sullivan and Fear1997) reported that 54% of patients with anorexia nervosa developed bulimia nervosa at some point during a mean follow-up interval of 15.5 years, with the median duration between onset of anorexia nervosa and conversion to bulimia nervosa of 2 years. Sullivan et al (Reference Sullivan, Bulik and Fear1998) reported that in patients who do not recover from anorexia nervosa, crossover to bulimia nervosa was a frequent occurrence. In addition, the results of our study confirmed the clinical impression that during the course of an eating disorder, crossover from bulimia nervosa to anorexia nervosa is also possible.
In line with our findings, the data from a 5-year follow-up study also indicated that there were considerable fluctuations between the eating disorder diagnoses, as well as differences between the categories in stability and remission rates, with anorexia nervosa having the highest stability and lowest remission rates compared with bulimia nervosa and EDNOS (Reference Ben-Tovim, Walker and GilchristBen-Tovim et al, 2001). However, this study assessed outcome only once and the diagnoses were not made using a standardised instrument.
Our results also showed that, after excluding participants with a stable remission, changes between eating disorder categories of the restrictive and the binge–purge type were frequent. In line with other studies (Reference Eckert, Halmi and MarchiEckert et al, 1995; Fichter & Quadflieg, Reference Fichter and Quadflieg1997, Reference Fichter and Quadflied1999; Reference SteinhausenSteinhausen, 2002), we found that participants with a non-purging non-purging eating disorder had a higher recovery rate than those with binge–purge behaviour.
Eating disorders or eating disorder?
The shared and distinctive psychopathology of anorexia nervosa, bulimia nervosa and EDNOS (Reference Fairburn and HarrisonFairburn & Harrison, 2003; Reference Fairburn and BohnFairburn & Bohn, 2005) and the frequent movement of patients between the diagnoses, together with the fact that the average age at onset did not differ between them, strengthens the view that these disorders have so much in common that they might be best viewed as a single entity. They also highlight certain limitations of the current diagnostic scheme: for example, minor changes in weight or eating behaviour can result in a person receiving an entirely different DSM–IV eating disorder diagnosis. Similarities and differences between the eating disorder diagnoses and the classification of eating disorders have been points of discussion for decades. Two recent developments are evident. One is to highlight the similarities between the eating disorder categories rather than focus on their differences. This is the basis of the ‘transdiagnostic’ view of the eating disorders (Reference Fairburn, Cooper and ShafranFairburn et al, 2003). The other trend is to examine the classification of eating disorders from the perspective of predictive validity (e.g. Reference Strober, Freeman and MorrellStrober et al, 1999; Reference Bulik, Sullivan and KendlerBulik et al, 2000; Reference Stice and FairburnStice & Fairburn, 2003; Reference Keel, Fichter and QuadfliegKeel et al, 2004). The findings of this study certainly suggest that the diagnostic migration that occurs between the eating disorders needs to be taken into account in thinking about their classification (Reference Fairburn and BohnFairburn & Bohn, 2005).
Limitations and strengths
Certain limitations of the study are of note. Cases of EDNOS were underrepresented in comparison with their proportion in out-patient eating disorder clinics (Reference Fairburn and BohnFairburn & Bohn, 2005). Most of the participants had some contact with treatment providers and it is conceivable that treatment might have contributed in part to the diagnostic changes observed. Withdrawal from the study was associated with younger age and shorter duration of eating disorder – possibly good prognostic features, thereby contributing to the low remission rate. Another possible limitation is the relatively short duration of follow-up (30 months), but this was not inappropriate since our aim was to study diagnostic fluctuation rather than long-term outcome. Further studies of the course of the full range of eating disorders are clearly needed, ideally with treatment controlled.
Strengths of the study include the broad patient sample, which included participants with anorexia nervosa, bulimia nervosa and EDNOS, and the use of standard diagnostic procedures with clinical severity thresholds.
Implications
Our findings have implications beyond nosology: the clinical reality of shared but distinctive clinical features across the eating disorders, together with diagnostic flux between them, signifies that underpinning the psychopathology of anorexia nervosa, bulimia nervosa and EDNOS are likely to be common biological (Reference Uher, Murphy and BrammerUher et al, 2004) and psychological causal and maintaining processes (Reference Fairburn, Cooper and ShafranFairburn et al, 2003). The implication of this is that transdiagnostic approaches to research on the psychopathology and treatment of these disorders, and their neurobiology, would be of merit.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ The eating disorder diagnoses of anorexia nervosa, bulimia nervosa and eating disorder not otherwise specified are not stable over time, although the overall category of ‘eating disorder’ does show considerable stability.
-
▪ Remission from an eating disorder is unusual even following treatment.
-
▪ Anorexia nervosa is the most stable diagnosis of the three DSM–IVeating disorders.
LIMITATIONS
-
▪ Most of the participants had treatment during the course of the study and this might have influenced the course of the eating disorder.
-
▪ Participants with the DSM–IVdiagnosis of eating disorder not otherwise specified were underrepresented in comparison with their proportion in out-patient eating disorder clinics.
-
▪ The duration of follow-up was relatively short (30 months).
Acknowledgements
The study was supported by the Swiss National Science Foundation (grants 23-51968.97 and 32-63954.00 to G.M.) and by the Federal Department for Education and Science (European Cooperation in the Field of Scientific and Technical Research, COST Action B6 - G.M.), Bern. G.C.F. is supported by a Principal Research Fellowship from the Wellcome Trust, London (046386).




eLetters
No eLetters have been published for this article.