



Introduction
To address the global challenge of dementia (Alzheimer's Disease International, 2018; World Health Organization, 2018), many international policy directives have sought to create ‘dementia-friendly communities’ (Alzheimer's Disease International, 2017). These consist of people who will ‘be aware of and understand dementia, and people with dementia will feel included and involved, and have choice and control over their day-to-day lives’ (Alzheimer's Society, 2013: 10). These initiatives emphasise the need to raise dementia awareness throughout communities and provide a more holistic or biopsychosocial understanding of the condition. This includes outlining the neurological/biological difficulties (e.g. memory loss, communication and navigational problems) and psychological challenges (e.g. apathy, agitation, depression and changing sense of identity) associated with dementia, as well as the social structures (e.g. lack of dementia services, limited signage in communities and poor public transport) and ‘discursive factors’ (e.g. the way we talk to or about people with the condition and engage with them) that can influence people's experiences of living with the condition (Kitwood, Reference Kitwood1997; Ward, Reference Ward2009; Spector and Orrell, Reference Spector and Orrell2010). Raising dementia awareness will ensure that the public and professionals feel better equipped with the knowledge, skills, understanding and attitudes to support the wellbeing and social inclusion of people with dementia and their care partners, thereby resulting in the reduction of societal stigma and fear associated with the condition (Alzheimer's Disease International, 2019).
Literature from the dementia field (Mukadam and Livingston, Reference Mukadam and Livingston2012) and the wider mental health arena (Corrigan et al., Reference Corrigan, River, Lundin, Penn, Uphoff-Wasowski, Campion, Mathisen, Cagnon, Bergman, Goldstein and Kubiak2001; Corrigan and Watson, Reference Corrigan and Watson2002) suggest there are two common strategies to raise awareness of stigmatised conditions such as dementia; these are education and contact. Education involves providing factual information on conditions to attempt to replace inaccurate stereotypes and beliefs, and increase affirming attitudes. Within the United Kingdom (UK), this learning approach is typified by the Alzheimer's Society's Dementia Friends programme, where community-based, lecture-style information sessions are provided by Dementia Champions. To date, the initiative has created over 3 million ‘dementia friends’ in the UK, although the limited evaluative research of the programme suggests it may have negligible impact on dementia attitudes, specifically in adolescents (Farina et al., Reference Farina, Hughes, Jones, Parveen, Griffiths, Galvin and Banerjee2020).
Contact, either direct or indirect, involves providing learners with the opportunity to interact with people living with stigmatising conditions. These ‘experiential learning’ approaches seek to enable the learner to take on the perspective of another and so better understand their situation, mind-sets and actions, rather than solely have a knowledge of their condition (Batson et al., Reference Batson, Early and Salvarani1997). Learning can occur at a cognitive level, where a person aims to know what another person is thinking and feeling, and at an affective level where they can feel what another person is feeling (Chmil et al., Reference Chmil, Turk, Adamson and Larew2015). Both of these may be important mechanisms for enabling people to generate a sense of empathy towards others (Batson et al., Reference Batson, Early and Salvarani1997). The innovative Time for Dementia initiative embodies an experiential learning approach that draws on the concept of ‘perspective-taking’ (Banerjee et al., Reference Banerjee, Farina, Daley, Grosvenor, Hughes, Hebditch, Mackrell, Nilforooshan, Wyatt, de Vries, Haq and Wright2017). The educational programme enables pairs of medical students to visit a person with dementia and their care partner at their home every three months for two years (during their five-year training) and engage in a range of activities designed to provide them with insight into living with dementia. Daley et al. (Reference Daley, Feeney, Grosvenor, Hebditch, Morley, Sleater, Wright and Banerjee2020) report on a recent qualitative evaluation of the initiative from the perspective of 77 health-care students, suggesting they welcomed the opportunity to develop deep, open and honest relationships with families living with dementia. This process of relational learning provided them with an insight into the condition and the emotions that can be experienced by the individual and their families throughout the dementia journey that is unlikely to have been achieved through lectures. Students reported that this insight enabled them to develop a better holistic understanding of dementia, to challenge some of the stigma they held around the condition, and to improve their dementia care skills such as communication techniques and person-centred care practices. Despite its apparent benefits, it is important to recognise the considerable financial and time resources that are required to set up and implement such a programme and, particularly given the current global context during the COVID-19 pandemic and the shielding of vulnerable, older populations, it is unclear whether or how its widespread adoption throughout the UK will continue. Consequently, in these unprecedented times and with fiscal restraints, it is important to consider more cost-effective, alternative initiatives that can provide these experiential learning opportunities. This is where virtual reality (VR) has an important role to play.
VR and dementia awareness
Virtual realities aim to immerse users into virtual environments that can appear and feel similar to the physical world (Weiss et al., Reference Weiss, Kizony, Feintuch, Katz, Selzer, Cohen and Gage2014).Footnote 1 The concept of immersion is integral to the success of VR experiences and relies on a user perceiving that they are physically present within a non-physical world. The perception is created by surrounding users with images, sound or other stimuli that provide an absorbing environment. Through these media, individuals can feel a sense of ‘presence’ or connection with a virtual scene, and so associate themselves with a persona that is not their own (Lee, Reference Lee2004) and experience the narrative as though they were the protagonist (Adefila et al., Reference Adefila, Graham, Clouder, Bluteau and Ball2016). To generate a sense of presence and authenticity, it has been posited that certain criteria must be achieved through the technology, including: a wide field of view (80° or better); adequate resolution; low pixel persistence; low latency; and global display where all pixels are illuminated simultaneously (Falconer, Reference Falconer2013). These VR experiences can also offer an element of simulation, which is a technique designed to replicate substantial aspects of real-world experiences in a fully interactive fashion (Gaba, Reference Gaba2007). Research has demonstrated that immersive VR can offer effective learning experiences for health professionals (Kyaw et al., Reference Kyaw, Saxena, Posadzki, Vseteckova, Nikolaou, George, Divakar, Masiello, Kononowicz, Zary and Car2019). For instance, a review by Wan and Lam (Reference Wan and Lam2019) highlights a positive relationship between VR simulation and the enhancement of health professionals’ empathy, attitudes and knowledge relating to mental illness. This suggests the potential for VR to provide an experiential learning opportunity that can enhance education around stigmatised health conditions.
The use of VR in dementia care education continues to develop, although it has been noted that this is an emerging field, and more robust and controlled studies are warranted (Hirt and Beer, Reference Hirt and Beer2020). The current literature highlights a range of immersive VR technologies that have focused on placing the user at the centre of the imagined experience and simulating through perceptions and/or bodily movements the challenges of living with dementia, thereby aiming to provide them with a better awareness of the condition. It is important to note, however, that dementia is a broad umbrella term encompassing many different conditions, and people's experiences of living with these can vary greatly (Górska et al., Reference Górska, Forsyth and Maciver2018). Therefore, whilst these technologies can provide important insights into the lived experience of dementia, they will only represent a sample of the wider population.
One of the earliest examples of these VR technologies was the Virtual Dementia Tour (VDT) (Beville Reference Beville2002, Reference Beville2014) that aimed to provide users with the perspective of living with moderate dementia. This is achieved through manipulating physical (wearing yellow tinted goggles to mimic effects of eye disease) and cognitive (noise delivered via headphones to induce a chaotic mental state) elements of the participants’ experience as they perform simple tasks such as pairing together socks. Additionally, to enhance learning, participants are invited to observe others perform the tasks to consider verbal and non-verbal reactions to the experience, as well as attend a reflexive debriefing session. Beville (2002) reported that VDT positively impacted on health-care professionals’ awareness of the emotional needs of people with dementia as well as their ability to recognise the symptoms of dementia and understand why people with dementia may exhibit certain behaviours. A more recent qualitative study that engaged 18 health-care staff and family carers with the VDT reported that the participants found it a useful experience that enabled a cognitive, moral and behavioural reflection to occur, which in turn was important for developing an empathic awareness of dementia (Slater et al., Reference Slater, Hasson, Gillen, Gallen and Parlour2019). Other research has highlighted the capabilities of alternative VR dementia simulation devices to create experiential learning opportunities for informal care partners (Jütten et al., Reference Jütten, Mark, Janssen, Rietsema, Dröes and Sitskoorn2017, Reference Jütten, Mark and Sitskoorn2018; Wijma et al., Reference Wijma, Veerbeek, Prins, Pot and Willemse2018) and students from varied health and social care professions (Adefila et al., Reference Adefila, Graham, Clouder, Bluteau and Ball2016). Similar to the current study, Adefila et al. (Reference Adefila, Graham, Clouder, Bluteau and Ball2016) and Wijma et al. (Reference Wijma, Veerbeek, Prins, Pot and Willemse2018) both used VR headsets to immerse students and informal care partners, respectively, into the perspective of a person with dementia. Whilst Wijma et al. (Reference Wijma, Veerbeek, Prins, Pot and Willemse2018) played users a simulation movie of daily situations faced by a person with dementia, with audio voice reflecting their inner thoughts, Adefila et al. (Reference Adefila, Graham, Clouder, Bluteau and Ball2016) provided a more interactive experience by tasking users to complete various activities of daily living such as making tea or having a shower whilst in a virtual residential home. The tasks were intended to evoke a sense of confusion (e.g. the milk is not initially in the fridge but after looking around the kitchen for it, participants return to the fridge to find it there) and so offer a glimpse into what it may be like to live with dementia. Following the tasks, participants were debriefed and encouraged to reflect on their experiences and consolidate their learning. Preliminary findings from these studies suggest that the VR experience can offer an experiential learning opportunity for users that may improve their competence, confidence and empathy when engaging with people with dementia (Adefila et al., Reference Adefila, Graham, Clouder, Bluteau and Ball2016; Wijma et al., Reference Wijma, Veerbeek, Prins, Pot and Willemse2018). To date, however, these VR applications are not commercially available and so this may hinder their ability to contribute to the ‘dementia-friendly communities’ agenda. Finally, Morganti et al. (Reference Morganti, Palena, Savoldelli and Greco2020) have drawn on the concept of ‘dementia-friendly communities’ in Italy to report on the benefits of the ViveDe project. Similar to the current study, the researchers use 360° videos, watched through reality eyeglasses, to present everyday situations that can be encountered by a person with dementia and hear their voice as though it was their own thoughts. Evaluation of the device with 170 members of the public (aged between 13 and 75) suggested the experience provided them with a deeper understanding of the impact of dementia on the individual as well as changed their beliefs about the needs and autonomy of people living with the condition.
Whilst the above provides an illustrative rather than exhaustive overview of the emerging literature within the dementia care field, it highlights the potential for VR to enhance dementia awareness amongst informal care partners, the general public and medical students. However, there is currently limited research that explores the use of commercially available and portable VR devices with UK care home practitioners. This is an important oversight to address as they will be a key player in driving forward the ‘dementia-friendly communities’ directive, given that around 280,000 people with dementia in the UK reside in care homes (Alzheimer's Society, 2016) and 80 per cent of all people living in UK care homes have some form of dementia or severe memory impairment (Knapp et al., Reference Knapp, Comas-Herrera, Wittenberg, Hu, King, Rehill and Adelaja2014). As such, it is important that care home practitioners are engaged in a range of training initiatives that enable them to develop high levels of dementia awareness. Furthermore, as Surr et al. (Reference Surr, Gates, Irving, Oyebode, Smith, Parveen, Drury and Dennison2017) have highlighted, health and social care staff welcome dementia educational programmes that provide an opportunity for experiential sessions. Therefore, the use of a portable, freely available VR tool that situates the user within the perspective of someone with dementia may be an engaging as well as cost-effective method to support dementia awareness training within this population. Through this exploratory study, we seek to address the research questions:
• What are care home practitioners’ experiences of engaging with the ‘A walk through dementia’ VR tool?
• What are their views on the potential for this VR device to be used as a dementia awareness-raising tool?
Design and methods
Research approach
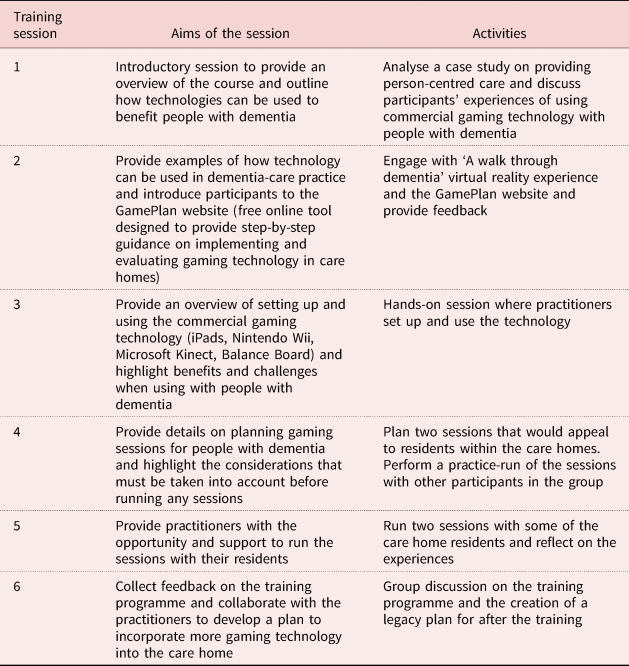
This paper reports on an exploratory, descriptive qualitative study. The data were collected as part of a wider project that aimed to increase care home staffs’ knowledge and practical skills on using commercially available digital gaming technology such as iPads, Nintendo Wii and Microsoft Kinect as a means to enhance the wellbeing of people with dementia. This sought to develop and evaluate collaboratively an online information resource for care home staff called ‘GamePlan’ and an accompanying face-to-face training programme led by BH. The training consisted of six weekly sessions, each lasting around two hours, and was undertaken across four care homes in the south-west of England. An overview of the training programme is presented in Table 1 and a paper detailing its development is currently in preparation. The VR tool discussed within the current study was used within Session 2 of this training programme, which was designed to provide the care staff with a flavour of the different types of commercially available gaming/technological products that were being developed and used within the dementia care arena. Ethical approval for the research was granted by Bournemouth University.
Table 1. Overview of technology training course
The VR tool
The VR tool was developed by Alzheimer's Research UK and VR specialists VISYON, in collaboration with people with various forms of dementia and their spouses who supported the development of the story and identified some of the key challenges they encountered in their everyday lives that could be represented in the VR scenarios (for an overview of the development of the scenarios, see https://www.youtube.com/watch?v=nW1Y3Fnv7Mw). The finished product is called ‘A walk through dementia’ and can be downloaded on to any android or iPhone free of charge from http://www.awalkthroughdementia.org/. The application uses the widely available Google Cardboard headset to immerse users virtually into the ‘shoes’ of a person with dementia, who is voiced by Dame Harriet Walter. The application combines computer-generated environments and 360° video sequences to provide an experiential account of some of the challenges that may be faced by someone with dementia whilst engaging in activities of daily living. Over three scenarios, users are tasked with buying ingredients from a supermarket, walking home while accompanied by their son and then making a cup of tea for the family. Each scenario is designed to highlight specific neurological difficulties people may have to contend with, such as counting money, wayfinding and memorising instructions, as well as challenges that can be imposed through social encounters. The supermarket scenario, which is digital based, offers an interactive element to it, as the user is tasked with selecting the appropriate food to put in the shopping basket. The other two scenarios are lifelike video sequences and are more passive, with the user taken on the physical and mental (as the character voices her internal monologue) journey with the person with dementia whilst they negotiate the tasks at hand. Sound effects have also been added at various points, such as an audibly quick heart rate when the character is anxious, to simulate some of the physiological responses to the psychological stressors.
Participant recruitment
Four local care homes in Dorset, south-west England were approached by the lead author (BH) through Bournemouth University's Ageing and Dementia Research Centre network to take part in the wider GamePlan training programme. The training was offered to the care homes free of charge and all agreed to participate on the proviso they could provide at least four care staff who would attend throughout the entire six weeks. A purposive sample of 20 care practitioners were recruited across the four care homes to participate in the programme. During Session 2, all of the participants, when offered the opportunity to engage with the VR tool, agreed to do so and provide their feedback on the experience. As such, all participants were conveniently sampled from the wider training programme and no screening processes were undertaken prior to them interacting with the VR tool; although all of them were made aware of their rights to withdraw from the activity at any point. Table 2 outlines the demographic data of the participants, which was collected during Session 1 of the GamePlan training programme. The majority were female (18) and were typically aged between 45 and 54 years old. They were all employed full-time at the care homes and predominantly in activity co-ordinator or care assistant roles.
Table 2. Demographic details of the focus group participants

Notes: VR: virtual reality. DNR: did not respond.
Research methods
The second training session was designed to provide the participants with an insight into the types of commercially available technology that was being used in the dementia care field. The VR activity was one such device that the participants were encouraged to engage with in the latter part of the training session at each care home, after they had interacted with other gaming technological devices. A group discussion was held immediately after the VR activity to collect data for the current study and provide the opportunity for the participants to reflect on their learning experience. Focus groups were deemed to be the most appropriate method to elicit participants’ views as they provided a platform for them to discuss and share their experiences among the wider group, as well as ensured that the data collection could occur within the two-hour time period allocated for each session.
The focus groups were undertaken by BH who has a PhD and extensive experience conducting qualitative research. He was supported by a post-doctoral researcher, who noted down key ideas suggested by each of the participants that were revisited during the analysis process. BH was also responsible for delivering the training programme and had developed a rapport with the participants prior to running the VR activity. This encouraged them to speak openly and honestly during the discussions. Furthermore, as the participants worked together within the care home on a daily basis they were familiar with each other and accustomed to exchanging ideas. As such, the focus groups were relaxed and participants showed few signs of apprehension when disagreeing with views that were expressed.
A semi-structured focus group schedule was used flexibly and the questions aimed to elicit participants’ perceptions and experiences of each of the scenarios and the VR tool more generally, as well as ascertain any insights it may have provided them into living with dementia, how it compared to previous dementia-awareness training they may have undertaken and its future potential as an educational tool in the dementia care arena. The feedback from this first formal evaluation of the VR device with care home staff was sought to provide Alzheimer's Research UK more insight into improving or extending the virtual scenarios, funding permitted, as well as greater understanding of the feasibility and acceptability of using the device to form the basis of a wider public dementia-awareness training programme; something the charity was actively discussing at this time with university partners. Prompts were used throughout the discussions to garner more detailed data on the participants’ experiences and perceptions, and to establish whether other members of the group were in agreement with the views put forward. These included: ‘could you elaborate on that?’, ‘why do you say that?’, ‘could you give me an example of that please?’ or ‘what do others think about this suggestion?’ The focus groups ranged in length from 32 to 45 minutes.
Researcher's reflexivity
As dictated by qualitative research, it is important to acknowledge the lead researcher's assumptions and personal biases that may have influenced the data collection and analysis processes (Flick, Reference Flick2014). Having successfully used off-the-shelf gaming technology as a psychosocial initiative for people with dementia, the lead researcher (BH) is an advocate of this medium within the dementia care field. This may have influenced the way he delivered the research questions and led on the data analysis procedure. Equally, the participants were predominantly open to the use of technology within dementia care and keen to develop their skills with this medium. This is likely to have created a very pro-technology environment during the data collection process that may have influenced the research outcomes.
Data analysis
Focus group recordings were transcribed, anonymised and uploaded on to NVivo 10 to manage the data analysis process. Pseudonyms preserved individuals’ identity. A six-phase thematic approach (Braun and Clarke, Reference Braun and Clarke2006) was used to analyse the data, which was undertaken by BH, IK and KM. This involved first reviewing the data to ensure familiarity with it. Following this, an inductive analytical approach was adopted to ground the initial codes in the participants’ own words. The researchers kept an open mind throughout the coding process and used both semantic and latent coding to identify as many potential themes/patterns as possible, on occasions placing individual extracts of the data into numerous codes. Elements of the discussions that did not necessarily fit with the emerging dominant story were also coded. Researchers’ reflexions were included in comment boxes and used to guide the development and testing of the themes later in the analysis process. Once all of the codes were identified, they were labelled with a short description and then organised into theme-piles. Mind-maps were developed to illustrate how the different codes could potentially combine to form an overarching theme and these were used to facilitate discussions between the three researchers. Any initial codes that did not seem to fit anywhere were labelled as ‘miscellaneous’ and then revisited throughout the analysis. During Stage 4 of the analysis process, the research team discussed how the themes sat together meaningfully and whether there was a clear and identifiable distinction between them (Braun and Clarke, Reference Braun and Clarke2006). This involved re-reading each of the themes to ensure they formed a coherent pattern, and where applicable certain data extracts were removed and either applied to another theme or discarded from the analysis. Once there was agreement between the three researchers on the final themes created, the dataset was re-read to allow the coding of any additional data within themes that had been missed in earlier coding stages.
Findings
The findings demonstrated that predominantly the care practitioners welcomed the VR tool as engaging and novel within their field. Even those with previous experience of VR had never encountered it within the context of dementia. Three themes constructed from the data suggested the participants perceived it to be a convincing immersive experience that was insightful and evocative, and provided ‘next-level’ dementia-awareness training. These themes, along with their sub-themes will be discussed in more detail below. Key quotes have been provided within the text to enhance the narrative flow, however, additional quotes that support the themes have been outlined in Table 3.
Table 3. Supplementary quotes from analysis

Note: VR: virtual reality.
A convincing immersive experience
The majority of participants were enthusiastic about the VR experience and saw it as a ‘fantastic tool’ (CH2, P2). When discussing their experiences, most of them reported positively on the immersive qualities of the VR tool and they welcomed the opportunity to adopt the perspective of a person with dementia, or ‘tune in again to [their] experiences’ (CH1, P6). Interestingly, this sense of immersion was also felt by the two male participants (CH3), despite the fact they had been tasked with virtually situating themselves into the perspective of a female protagonist.
Generating feelings of immersion, where the participants bought into the scenarios and felt that they were simulating the experiences of someone with dementia, was integral to the success of the VR experience. This sensation was created through the toolkit itself, with the participants wearing the headsets and earphones, which provided audio commentary on the mind-set of the protagonist, as well as the solitary nature of the activity. These components ensured practitioners were ‘sent into the world’ (CH1, P6) and engulfed in the experience and their attention was not diverted, thereby forcing them to engage fully within the world of someone living with dementia and not ‘zone out’ (CH1, P1):
Yeah, the fact that you're closed off from the rest of the room completely, you can't see anyone else … all I could really hear was her. You are in that scenario with no help you are actually feeling every part of it. (CH2, P1)
This experience was viewed by practitioners in CH1 as something different to the usual dementia training they attended that was predominantly group-based and whilst ‘a bit of a laugh’ (CH1, P2), this environment could distract them from immersing themselves fully into the activities, and so potentially lessen the impact of the learning.
The realistic and convincing nature of the scenarios was also paramount to creating a sense of immersion and engaging the practitioners. This realism was generated through two means. Firstly, the graphics were important for producing a scenario that was visually convincing to the practitioners, and it was often the case that the two scenarios that were filmed (on the street and making the cup of tea) were perceived as being more real and so preferred to the supermarket scenario that was digital based:
P4: Mmm yeah the visuals. I think made the difference for me. It made the difference because it was real.
P6: Yeah the shop one almost looked fake.
P4: Like a game. (CH1)
Secondly, creating a scene that the practitioners could recognise from their personal lives and/or work experiences helped to ensure that they were convinced by it. Across the care homes, as participants discussed the scenarios they reflected on instances where they had supported people with dementia who had encountered similar challenges or family members who had displayed similar behaviours as those that were presented during the VR experience. This ensured that practitioners bought into the scenarios and could therefore allow themselves to be immersed within it:
I think the tea one reminded me of our patient. (CH1, P3)
P3: That's what a lot of families are like aren't they? You know you see husbands or daughters or sons kind of you know?
P1: Yeah they aren't doing well with it.
P2 and P3: No. (CH4)
Indeed, on occasions where elements of the scenario were perceived as unrealistic (such as an empty supermarket), this seemed to detract from practitioners’ generally positive experiences of them.
This finding suggests that the VR tool created a convincing and immersive experience for the majority of practitioners. However, during the discussions, it was evident that for some participants a number of challenges arose that hindered their sense of immersion and so detracted from their positive experience.
Challenges for immersion
Only two participants reported that they did not feel some degree of immersion when engaging with the VR tool. They both worked in CH4 and chose not to wear the headsets, opting instead to watch the scenarios whilst holding the smartphone in their hand. It was evident during discussions that the VR experience had a limited impact on them as they felt it was ‘unrealistic’ (CH4, P2).
Furthermore, P2 in CH4 perceived the VR scenarios to be ‘pointless’, suggesting that this was not the way that living with dementia should be described to people. Consequently, this further added to her ambivalence towards the VR exercise:
If you want to explain dementia to someone, that [VR] wasn't the way. It's like sitting in a room and things are taken away. And more and more things are taken away. You are left with yourself. That's how it is, that's how it should be put in the training… (CH4, P2)
For those participants who wore the headsets, there were still challenges that some were tasked with overcoming before they could absorb themselves within the experience. These concerned their physiological responses as they engaged with the VR experience as well as issues associated with the toolkit. One participant (CH3, P4) who was new to VR reported feeling apprehensive initially about the immersive experience and others across all care homes discussed feeling temporarily disorientated, dizzy or slightly nauseous. Fortunately, over time, as participants became accustomed to the immersion, these sensations subsided.
Participants also reported other barriers associated with the VR interface that detracted from their sense of immersion. These included the cardboard headsets, which participants felt were uncomfortable to wear and did not allow you to adjust the focus on the screen, and the smartphones (both commercially available androids and iPhones) that were used to play the VR scenarios, which on occasions were dirty or slightly cracked and so reduced the clarity of the picture. One participant, a self-proclaimed ‘tech-nerd’, emphasised how overcoming these issues was important for creating an engaging immersive experience, however, he did acknowledge that for VR beginners this would still be a beneficial tool:
I remember the very first time I experienced VR and it was much more overwhelming, and much more immersive … just little things like light coming in from the side … if it was totally black you would feel you were really inside it … Little things like some of the human people in it looked a little bit blocky and animated. They didn't really feel like it was a real person … I'd imagine the more expensive the kit, the greater reality, but yeah, I could imagine if you've never done a VR and you haven't got much experience of working with people with dementia, it could really help you understand. (CH3, P4)
This finding highlights there were a number of challenges that could hinder or prevent users from fully immersing themselves in the VR scenarios and so detract from the overall learning experience. Some of these may be overcome as participants have more interactions with VR experiences, although others associated with the VR toolkit may be more difficult and expensive to address.
Insightful and evocative: an experience for the mind and body
The VR experience provided the practitioners with a better understanding (mind) and feeling (body) of what it may be like to live with dementia.
For the mind
Across all care homes, the practitioners discussed how the VR experience had been ‘eye-opening’ (CH3, P3) for them and through its immersive qualities had offered them an insight into some of the challenges people living with dementia may experience and the feelings that these may evoke:
It's just a little window into dementia … It always makes you more aware … knowing the challenges that face people with dementia on a daily basis. (CH2, P2)
A few of the practitioners discussed some of the neurological challenges of dementia that they were previously unaware of, which were depicted in the VR experience. In particular, they reflected on the supermarket and street scenarios that highlighted the disorientation and perception difficulties encountered by the protagonist as she attempts to decipher items on the shelves (supermarket scenario) or navigate around a puddle that she believes to be a hole in the ground (street scenario). Experiencing these challenges from the perspective of this person with dementia appeared to provide them with more insight and a better understanding of their impact:
P1: It makes you aware a lot more.
P2: Yeah that disorientation was horrible … and I've never really sort of been aware of that before.
P1: No I haven't. It's a completely new experience. (CH3)
However, the majority of the practitioners discussed how the VR experience had emphasised the social or ‘discursive’ barriers (Ward, Reference Ward2009) that were encountered by the protagonist in their daily life. These barriers are concerned with the actions that people undertake and the language they use when interacting with people with dementia. Practitioners noted the detrimental behaviours that were evident across all three scenarios, as well as the instances where people's positive behaviours could enhance the psychological wellbeing of the person with dementia:
I like the way the daughter handled it. When the friends were like ‘oh I've got no milk in my tea’, and she was like ‘oh yeah it's okay’ sort of thing. Like reassuring her mum … That was attentive. I think people need to be more like the daughter really, not the son (laughter) who wasn't caring. He didn't seem bothered at all. (CH3, P1)
During discussions, it was evident that the immersive qualities of the VR experience were integral to the positive impact of this learning. Through enabling the practitioners to adopt the position of someone with dementia, or ‘be in their skin’ (CH2, P1), it provided them a better insight or cognitive awareness of how it might feel to encounter neurological and discursive challenges:
P2: It just opens people's eyes and mind. Realise what goes on. How they feel sometimes sort of.
P3: You get a better feeling and insight into how people living with dementia must feel. (CH1)
As one practitioner highlighted, experiencing the challenges first-hand was more insightful for her than any words that could be used to describe the challenges:
…it does give you different insights than people just telling you because no matter how much someone tells you something, you can't really understand how it feels and it does give you another level of experiencing that. I wouldn't say that was distressful for me … but it does give me a better insight into how people can become distressed. (CH3, P4)
This finding suggests that the VR experience provided the care practitioners with the opportunity to bring to the forefront of their mind the daily challenges that someone with dementia may face and, in particular, those that are created during interactions with other people. Whilst, given their background and training, many were already knowledgeable about these challenges, the immersive qualities of the VR experience provided them with a better insight into the impact these barriers can have on the psychological wellbeing of a person with dementia. Furthermore, for some practitioners it was also apparent that during these experiences they engaged in a process of emotional transference.
For the body: emotional transference
Practitioners discussed how the immersive qualities of the VR tool highlighted the emotional impact of dementia but also enabled them to begin to feel what it might be like when encountering and attempting to overcome the neurological and discursive barriers. Through a process of emotional transference, participants across all care homes (with the exception of the two who chose not to use the headsets) reported feeling similar emotions, and in some instances displaying similar physiological responses, as that of the protagonist. For some, this was particularly difficult to deal with:
I could only watch one because it freaked me out. I don't know about the rest of you, I couldn't handle it. Seeing someone, hearing someone when they're distressed, distressed me. (CH4, P1)
The emotional transference appeared to be achieved through multiple mechanisms. The VR toolkit, through its audio (narration of the protagonist's thoughts along with her physiological responses such as a rapid heartbeat) and visuals (e.g. blurring of the screen), created an environment that for some practitioners evoked a similar emotional response to that of the protagonist:
I couldn't get over how scary it was. Because everything was slightly echoey. And then not being able to see people until they were quite close and so she thought it was her son coming towards her in the road, when it actually wasn't. So yeah quite frightening for me actually. (CH1, P6)
During the shopping scenario, where practitioners were tasked with engaging with the environment, unlike the other two scenarios where they passively watched, the design of this activity also evoked negative emotions as participants unsuccessfully attempted to find and place items in their shopping basket. For other practitioners who described a sensation of emotional transference, this appeared to be achieved through the realism of the scenes and practitioners’ ability to immerse themselves within them and then relate to how it would make them feel emotionally if they ever encountered these difficulties in the physical world. Consequently, this then triggered them to experience these actual emotions:
I got a bit of anxiety when I was in the supermarket … Well I don't like supermarkets anyway, I get a bit claustrophobic. So to go in there I could actually feel I was getting a bit panicky. I just gathered myself, some deep breaths. I could really feel but didn't like it. (CH2, P3)
This finding suggests that the immersive and realistic qualities of the VR tool resulted in some practitioners engaging in a process of emotional transference. This meant that not only did they better understand some of the emotional challenges encountered by the protagonist they were also able to feel them, thereby amplifying their learning experience.
‘Next-level’ dementia awareness
Having been through the VR experience the practitioners engaged together in a process of reflection, both inwardly (personal) and outwardly (wider dementia field).
Inward reflection
As practitioners discussed the insights and emotions they experienced, they began to reflect on their own practices both in the workplace and in wider society. Some practitioners highlighted instances during their career where they had supported people with dementia facing similar challenges as those depicted in the VR scenarios. They reported that the immersive qualities of the VR experience had provided them with a greater awareness and emotional understanding of some of these difficulties and they could bring this new learning into their practice:
That was actually quite an eye opener because some of the things I do without even thinking. And actually that can be such a negative thing for people in my care … Like we see it as a puddle, but it makes you realise why they don't cross certain paths, not to rush them because they're finding it really difficult. (CH3, P3)
Interestingly, two care homes discussed residents whom they were currently supporting and how the VR experience provided them with insights into and the opportunity to reflect on how they could address the challenges these residents encountered. In CH2, the practitioners reported on the need to amend some of their behaviours when facilitating one resident who enjoyed making cups of tea for the home. Practitioners in CH3 considered their learning around distorted perceptions to understand why a recent solution to support a resident in using the toilet had been so successful:
We've tried to assist him in the bathroom, he wouldn't stay on the toilet and we couldn't understand why and someone suggested black toilet seat and then he sat down on it … So to watch the VR thing, that was quite an eye opener and … made me realise, he couldn't see there was actually a seat to sit on. So putting the black seat he could differentiate the seat from the toilet. (CH3, P3)
One practitioner also reflected on how she could apply the learning outside her work practice, by pausing and offering more time to people who may be struggling with certain activities such as finding their change in a busy supermarket.
Interestingly, all these practitioners had numerous years within the care field and so it was positive and noteworthy that the VR experience was still able to provide them with new insights into dementia that they could inwardly reflect on for their own practice.
This finding suggests that the insights into the challenges and emotions of living with dementia that were offered by the immersive VR experience enabled some practitioners to reflect on their work and social practices, and so consider ways they might be enhanced. Unsurprisingly, given these positive experiences, the practitioners were keen to advocate the use of the VR toolkit as a dementia-awareness training package for other care practitioners, family members and the public.
Outward reflection
The majority of practitioners welcomed the suggestion that the VR toolkit could be used as a novel dementia-awareness training device as it ‘really raises the game’ (CH3, P3) and takes the field to a ‘whole different level’ (CH3, P1). As such, they believed the experiential learning opportunity would make a useful addition to training packages such as Dementia Friends, as well as to the general teaching provided in their care settings:
And using it as part of Dementia Friends training in business, it would be good for them as well to be able to experience what you are trying to explain to people. (CH1, P3)
They highlighted the need to enhance understandings of dementia community-wide and challenge some of the negative attitudes that are prevalent throughout society, and believed the VR tool would be a useful device for achieving this goal. As three care homes discussed, it might be particularly pertinent to target younger people, so as to address the stigma of ageing and dementia, as well as encourage them to consider and value careers in care.
As they reflected on their own experiences of engaging with the tool, practitioners felt that offering the wider community the opportunity to experience it would be beneficial as:
It says more than words! There's only so much you can be taught but it's nothing compared to being put in their shoes. (CH3, P1)
Through this experiential approach, they believed the general public and family carers would be able to gain first-hand insight into some of the barriers and emotional difficulties encountered by some people with dementia, as well as potentially feel those emotions themselves. This may help them to have more understanding, compassion and empathy for people with dementia and so be more willing and considerate when supporting them:
Because if you can start to feel what it is like … for someone who is living with dementia, then you can start having more compassion and if you've got more compassion for someone then your whole way of caring is going to be different. (CH1, P6)
However, as practitioners in CH1 and CH2 warned, it was important that any person who engaged with the VR tool was provided time, space and support to reflect on their experiences, particularly if it evoked strong emotional responses.
This finding highlights practitioners’ enthusiastic responses to using the VR toolkit as part of a dementia-awareness training package for care staff and all community members. They suggested the experiential approach could provide something different to what was currently on offer as well as impart important insights and evoke emotional responses that may result in more compassion towards people living with dementia.
Discussion
This is the first study that has explored the experiences of UK care home practitioners when engaging with the ‘A walk through dementia’ VR application. Adopting a descriptive qualitative design and eliciting the views from 20 care home practitioners using focus groups, our research set out to address two main questions: What are care home practitioners’ experiences of engaging with the VR tool? and What are their views on the potential for this VR device to be used as a dementia awareness-raising tool?
Our findings, constructed from an inductive analysis of the data, will be discussed below in relation to these questions and situated within the context of the wider academic literature. Based on these findings, we also offer recommendations for educators and VR software developers who wish to engage with this agenda.
What are care home practitioners’ experiences of engaging with the VR tool?
The majority of care practitioners welcomed the opportunity to use the VR tool and perceived it positively. Part of its appeal was attributed to its novelty within the dementia educational field, with all of the practitioners, including those with many years of experience and training in dementia care, highlighting that they had never encountered something like this previously within their work. This is unsurprising, given the academic literature acknowledges that VR is an emerging area of interest within the dementia field (Hirt and Beer, Reference Hirt and Beer2020), and therefore warrants further investigation into how and where the tools can be applied and the impact they may have. Promisingly, our findings suggest that there is scope to use VR as an educational tool with care home practitioners as even those practitioners with more familiarity of higher-quality VR toolkits and scenarios were positive about their experience and recognised the benefits that this free and portable device could provide within their field.
Practitioners perceived that the main appeal and success of the VR application stemmed from its ability to transport and immerse them virtually into the perspective of someone living with dementia. This was achieved by practitioners wearing the VR headset and speakers and so engulfing themselves within the solitary VR experience, thereby enabling them to concentrate fully on each of the scenarios. Indeed, it is telling that the two practitioners, both in the same care home, who did not appear to enjoy or gain from the experience chose not to use the headsets and speakers, highlighting the importance of immersion for generating this positive learning experience. Furthermore, and crucial to creating this sense of immersion, was the ability for the VR toolkit to construct a feeling of presence where the practitioners felt as if they were situated in the position of someone with dementia. This was achieved through using scenarios that the practitioners perceived as realistic and could relate to from their years of experience working within the dementia-care field. Interestingly, both male participants reported this sense of presence despite the narrative being delivered by a female protagonist. Potentially, it was the immersive qualities of the toolkit and the relatability of the scenarios that helped them to overcome the juxtaposition between their gender and that of the protagonist, and so enable them to benefit from feeling a sense of presence. Therefore, generally our findings are in accordance with other scholars who highlight the benefit of VR for dementia education (Adefila et al., Reference Adefila, Graham, Clouder, Bluteau and Ball2016; Wijma et al., Reference Wijma, Veerbeek, Prins, Pot and Willemse2018; Morganti et al., Reference Morganti, Palena, Savoldelli and Greco2020) as well as the wider VR literature (Falconer, Reference Falconer2013) that points to the importance and benefits of creating a sense of immersion and presence within virtual scenarios; suggesting this can still be achieved through relatively low-specification devices, particularly with audiences that may have limited experience of VR applications. Furthermore, our findings provide valuable evidence to justify the decision to consult with people with dementia whilst creating the virtual scenarios, thereby ensuring that they accurately portrayed a realistic account of some of their lived experiences. This supports scholars who have highlighted the importance of collaborating with people with dementia throughout the design, implementation and evaluation of technological devices to ensure they are fit for purpose (Kenigsberg et al., Reference Kenigsberg, Aquino, Bérard, Brémond, Charras, Dening, Droes, Gzil, Hicks, Innes, Nguyen, Nygard, Pino, Sacco, Salmon, van der Roest, Villet, Villez, Robert and Manera2019), and suggests these principles should continue to be adopted within the field of VR for dementia care and/or education.
Despite practitioners generally reporting a sense of immersion and presence throughout the VR experience, it is important to acknowledge that this was not universal for all virtual scenarios and there were some challenges that practitioners had to overcome to achieve this sensation. For instance, some practitioners reported that their sense of presence was disrupted by their adverse reactions to immersing themselves within the virtual landscape, as they began to feel dizzy or nauseous, and on occasions these feelings may have been exacerbated by the smartphone screen if it was cracked or dirty. These side-effects are widely recognised within the VR literature (LaViola, Reference LaViola2000) and may be more prevalent within the current participants given their inexperience with using this technology. As these issues were not reported by those who were more accustomed to VR, it is likely that over time and with further engagement with the technology these undesirable feelings will dissipate in novice VR care home practitioners. However, it is important that educators seeking to use these tools within care homes are wary that this is likely to be a novel experience for many, and whilst immersion should be encouraged as it can enhance the appeal of the activity, it is important that they are mindful of, and seek ways to mitigate against, any detrimental impact to participants’ health. Guidance on ways to achieve this, such as providing break-out spaces where people can sit and recuperate and ensuring the smartphones displaying the VR scenarios are clean and fully functioning, would be valuable if these applications are to become more widespread within care homes and further afield. Future research in this field may also wish to screen participants prior to engaging them with VR technology and so filter out those people who may have an adverse reaction to it.
Furthermore, some practitioners reported that the quality of the graphics on some scenarios, particularly the supermarket, looked ‘fake’ (CH1, P6) and, as such, they preferred the more graphically realistic scenarios on the street and making the cup of tea. The VR literature has set out guidelines for creating VR landscapes that can generate a sense of immersion and presence (Falconer, Reference Falconer2013). It is important that software developers looking to use VR as a tool to enhance dementia awareness pay heed to these recommendations and allocate their resources accordingly to this task. Developing virtual scenarios that are perceived to be unrealistic due to the quality of their graphical content is likely to impact detrimentally on the users’ overall experience with the technology and therefore potentially lessen the educational messages that are being communicated. Over time, as these technologies improve, it is possible that the cost of creating these high-quality scenarios will reduce.
What are care home practitioners’ views on the potential for this VR device to be used as a dementia awareness-raising tool?
It is a welcomed finding in itself that, given many of the practitioners were well accustomed to dementia training courses, they almost unanimously felt that the VR toolkit offered something new, different and informative. However, as many of the practitioners had attended numerous training programmes, it was unsurprising that only a limited number felt the VR toolkit provided them greater knowledge of some of the neurological/biological issues that can be encountered by people with dementia. In audiences with less experience of dementia and dementia-awareness training then the VR scenarios may be more informative at this level. However, what was more promising from our findings was that the majority of care home practitioners reported that the immersive qualities of the VR experience provided them a greater understanding into the psychological and/or emotional challenges of living with dementia and, consequently, they began to reflect inwardly on some of their practices, both in their work and wider daily lives. For many of them, this learning occurred at a cognitive level, as they highlighted how the scenarios offered them a deeper understanding of how it may feel to live with dementia than can be depicted through traditional taught training methods. However, for some practitioners this learning occurred at an affective level, as they reported that their own bodies began to mimic the physiological responses of the protagonist such as their increased heart rate, and so they began to feel what it might be like for them to live with dementia. Having a greater understanding of the emotional impact of stigmatised conditions, as well as knowledge about them, is a key aim of experiential or contact learning approaches (Batson et al., Reference Batson, Early and Salvarani1997) and will be integral for fully realising the ‘dementia-friendly communities’ agenda (Alzheimer's Disease International, 2017). This suggests that the VR toolkit can provide an experiential learning experience that may compliment other dementia education training initiatives that are more fact-based, such as the Alzheimer's Society's Dementia Friends courses, and this may have a positive impact for many audiences and particularly those with less experience and training in dementia.
Furthermore, based on their experiences, the practitioners discussed how the tool may provide the public, and in particular younger people, with an engaging format to develop empathy or compassion for people with dementia, as well as appreciate how their actions (or lack of) can detrimentally impact on the wellbeing of these people. Addressing both of these components will be imperative for developing ‘dementia-friendly communities’ where people with dementia feel understood and enabled to contribute (Alzheimer's Disease International, 2017). For instance, research has demonstrated that creating empathy for a person, where we understand and except another person's experiences, is an integral step in providing compassionate support for them, which acknowledges their challenges and responds accordingly (Cunico et al., Reference Cunico, Sartori, Marognolli and Meneghini2012; Digby et al., Reference Digby, Williams and Lee2016). Furthermore, to provide this compassionate support, it is essential that people are mindful of how their actions and language can enhance or worsen people's abilities to contribute and to live well with the condition (Kitwood, Reference Kitwood1997; Ward, Reference Ward2009). This is in accordance with the social model of disability (Oliver, Reference Oliver2013) and the social citizenship agenda (Bartlett and O'Connor, Reference Bartlett and O'Connor2010), which seek to reframe the challenges and responsibilities of dementia away from the individual level to a societal one. Our findings suggest, therefore, that similar to other experiential training programmes within the dementia field (Banerjee et al., Reference Banerjee, Farina, Daley, Grosvenor, Hughes, Hebditch, Mackrell, Nilforooshan, Wyatt, de Vries, Haq and Wright2017) and other VR research (Adefila et al., Reference Adefila, Graham, Clouder, Bluteau and Ball2016; Jütten et al., Reference Jütten, Mark and Sitskoorn2018; Slater et al., Reference Slater, Hasson, Gillen, Gallen and Parlour2019), this VR toolkit may enable users to develop a level of empathy for people living with dementia and furthermore provide them with a broader, biopsychosocial understanding of the condition, meaning it is likely to contribute positively to the ‘dementia-friendly communities’ agenda. As the tool is free and widely available for download on to any android or Apple smartphone, it may be particularly welcomed in these unprecedented times of physical distancing and where restricted financial resources may limit the implementation of other more expensive experiential training initiatives and VR devices that simulate the experience of living with dementia.
It is important to note, however, that all of the scenarios depicted people struggling to live with dementia. Whilst this can be effective at raising awareness of the challenges of dementia, it can inadvertently perpetuate the ‘tragedy discourse’ that is prevalent throughout society, where the losses associated with the condition are emphasised and prioritised, thereby resulting in a greater stigmatisation of the condition and a tendency to view people with dementia with despair (Behuniak Reference Behuniak2011; McParland et al., Reference McParland, Kelly and Innes2017). To truly realise the ‘dementia-friendly communities’ agenda, researchers have posited the need for more ‘dementia-positive’ attitudes to be fostered throughout societies, where people with dementia are perceived as equal contributors (Lin and Lewis, Reference Lin and Lewis2015). It is important, therefore, that software developers are mindful of this and seek to develop virtual scenarios where people with dementia are portrayed in a more empowering way. Linked to this, the practitioners also highlighted that the scenarios predominantly depicted the negative actions and behaviours of others that exacerbated the challenges faced by the protagonist. To provide a more complete learning experience and demonstrate how people can be more ‘dementia-aware’, it would be beneficial to find ways to depict or outline the positive actions that others can take to support people with dementia to live well and undertake their activities of daily living. One way potentially to achieve this is to incorporate the VR toolkit into a wider training programme, where the scenarios are reflected upon and discussed by the learners. This work is currently under way through collaborations with Alzheimer's Research UK and university partners who are discussing how the VR tool can be integrated alongside follow-up discussions with educational takeaway messages that are tailored towards various audiences with differing knowledge and experience of dementia (Board et al., Reference Board, Mitchell, Phipps and Murphy2018). The findings from this research can be used to inform these conversations and help to develop the format and learning materials for a future educational programme based around ‘A walk through dementia’ VR activity.
Limitations of the research and areas for future consideration
Whilst this study has provided the first insights into the experiences of care home practitioners to using the ‘A walk through dementia’ VR toolkit, the number of participants in the study was conveniently sampled from those who had a prior interest in using gaming technology within their working practice. Their views may therefore be more biased towards the adoption of these pieces of technology within the dementia field. Future research would benefit from sampling more widely to include care home practitioners who may not be as open to using gaming/VR technology within the workplace to establish whether the device still appeals and is positively reviewed by this population. Furthermore, whilst there was an indication that the VR experience enabled the care practitioners to reflect on their attitudes and behaviours, the research was not designed to check systematically any changes in the participants cognitive and affective awareness of dementia or follow up to ascertain how and whether this translated into their work practices. More longitudinal and experimental research is required to examine and measure any impacts over time. It would be beneficial to conduct this work alongside evaluating other mainstream dementia-awareness educational programmes such as the Alzheimer's Society's Dementia Friends programme to ascertain how they compare both on cost-effectiveness and long-term impact for the learner.
Conclusion
Our findings suggest that the ‘A walk through dementia’ VR application has the potential for providing an appealing, immersive and realistic experience that can afford care home practitioners insight into the lived emotional accounts of a person with dementia. In accordance with other research, the findings also provide further evidence of the possibilities of using VR as an experiential tool to benefit dementia awareness (Adefila et al., Reference Adefila, Graham, Clouder, Bluteau and Ball2016; Jütten et al., Reference Jütten, Mark and Sitskoorn2018) and so take the educational agenda to the ‘next level’. However, to realise the potential of the VR application fully it is likely that some challenges will need to be addressed and guidance provided to educators to ensure it can be successfully incorporated within a wider care home training programme to support the ‘dementia-friendly communities’ agenda.
Acknowledgements
The researchers would like to thank the care home practitioners who participated in the discussions and the wider training programme. BH would like to thank Bournemouth University which provided him with Higher Education Innovation Funding (HEIF) to conduct the research whilst he was a lecturer at the university.
Funding
This research and the wider training programme was conducted using funding obtained from Bournemouth University's Higher Education Innovation Funding (HEIF).
Ethical standards
Ethical approval for the research was granted by Bournemouth University.



