Introduction
Suicide is a global phenomenon and accounts for 1.4% of all deaths worldwide (World Health Organization, 2021). Nearly 800 000 people die due to suicide annually (World Health Organization, 2021). Unlike many causes of death, suicide is not a result of a single process of disease (Gunnell & Lewis, Reference Gunnell and Lewis2005), it is an outcome of a complex multiple interaction, involving biological (such as genetics), psychological (such as certain personality traits), clinical (such as comorbid psychiatric illness), social and environmental factors (Turecki et al., Reference Turecki, Brent, Gunnell, O'Connor, Oquendo, Pirkis and Stanley2019).
Serious mental illness is a diagnosable mental, behavioral, or emotional disorder that causes serious functional impairment and substantially interferes with or limit one or more major life activities (SAMHSA, 2020). People with serious mental illness live socially excluded, subject to the problems of impairment, discrimination, diminished social roles, unemployment, and lack of social networks (Richter & Hoffmann, Reference Richter and Hoffmann2019). Additionally, early-onset serious mental illness substantially worsens lifetime outcomes in the USA, leading to 10 fewer quality-adjusted life years, 24% higher medical spending and 48% lower earnings (Seabury et al., Reference Seabury, Axeen, Pauley, Tysinger, Schlosser, Hernandez and Goldman2019). Serious mental disorders also bring high-income countries and low- and middle-income countries great societal costs, with losses equivalent to 0.3–0.8% of total national earnings (Levinson et al., Reference Levinson, Lakoma, Petukhova, Schoenbaum, Zaslavsky, Angermeyer and Kessler2010).
A recent US study (Schmutte, Costa, Hammer, & Davidson, Reference Schmutte, Costa, Hammer and Davidson2021) reported a marked excess of suicide deaths in people with serious mental illness, compared to those with other or no known mental illness. A meta-analysis of suicide rates after discharge from psychiatric facilities has reported that the suicide rates for patients with affective disorder, psychosis, and mixed and other diagnosis were 524 per 100 000 person-years, 599 per 100 000 person-years, and 463 per 100 000 person-years, respectively (Chung et al., Reference Chung, Ryan, Hadzi-Pavlovic, Singh, Stanton and Large2017). However, there are no accepted benchmarks for suicide rates among people with serious mental illness.
Considering the severity of the problem, an in-depth and comprehensive review of the current status is urgent, which will make an impact on suicide prevention at a global level. A synthesis of the existing literature about suicide rates would help quantify the extent of this issue and guide future research and clinical guidance. This meta-analysis focuses on epidemiological evidence for suicide rates among people with serious mental illness (including bipolar disorder, major depression, or schizophrenia). We aimed to calculate a pooled estimate of suicide rate and determine the suicide rates regarding continents, psychiatric diagnosis, duration of follow-up, sex, and suicide methods.
Method
This systematic review and meta-analysis was conducted according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) (Stroup et al., Reference Stroup, Berlin, Morton, Olkin, Williamson, Rennie and Thacker2000) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher, Liberati, Tetzlaff, & Altman, Reference Moher, Liberati, Tetzlaff and Altman2009) standard.
Search strategy
PubMed and Web of Science were searched for relevant articles published in English from 1 January 1975 to 10 December 2020, with the various combinations of the terms bipolar disorder, schizophrenia, major depression, serious mental illness, severe mental illness, and suicid*, mortalit*, death* (online Supplementary eTable 1). Reference lists of relevant review articles and all included articles were searched for additional eligible papers. Gray literature was not reviewed. Two investigators independently assessed titles, abstracts, and full-text publications. Any disagreements were resolved by discussion with a third investigator.
Inclusion and exclusion criteria
In this review, serious mental illness included bipolar disorder, major depression, and schizophrenia. We included studies that reported the number of suicides among people with bipolar disorder, major depression, or schizophrenia, and the number of person-years in which the suicides occurred. Studies were also considered eligible if they contained data from which the suicide rate could be derived using the reported rate, the mean length of patient follow-up, or the duration of follow-up. Eligible studies had to recruit at least 50 participants. There was no restriction on age. Studies of suicide attempts were excluded. When two studies reported overlapping samples from the same national registers, the study with earlier enrollment period was excluded. Case studies, case series, randomized controlled trial, cross-sectional study, qualitative studies, systematic reviews, and abstracts were not eligible.
Data extraction
Data were extracted by two investigators to ensure consistency, again with any discrepancies resolved by discussion with a third investigator. Key study characteristics included author names, year of publication, country of study, enrollment period, study design, age, proportion of female, psychiatric diagnosis, and sample size. For the calculation of suicide rates, the number of suicides and the person-years were extracted. In some publications, the number of person-years could be estimated using the number of suicides and reported suicide rate, or the reported duration of follow-up.
Quality assessment
Two raters independently appraised study quality. The quality of included articles was assessed using a tool specifically designed to assess bias in prevalence studies (Hoy et al., Reference Hoy, Brooks, Woolf, Blyth, March, Bain and Buchbinder2012). This chosen tool addressed four domains of bias, including selection bias, nonresponse bias, measurement bias, and bias related to the analysis. It consists of 10 items, which are scored positively or negatively. According to the total score, each study was rated as low, moderate, or high risk of bias. Studies at high risk of bias were excluded from this meta-analysis.
Statistical analysis
Stata version 12.0 (StataCorp) was used to generate meta-analysis for suicide rates among people with serious mental illness. The suicide rate per person-year was the effect size measure. The pooled effect size was calculated using the metaprop command (Nyaga, Arbyn, & Aerts, Reference Nyaga, Arbyn and Aerts2014), which allows for the inclusion of studies with 0% or 100% prevalence proportions and avoids confidence intervals exceeding the 0–1 range. The Freeman-Tukey double arcsine transformation was performed to stabilize the variances (Nyaga et al., Reference Nyaga, Arbyn and Aerts2014). Study-specific 95% confidence intervals (CIs) were generated using the exact method. Random-effects meta-analysis was used due to the high expected heterogeneity between studies. The Q tests and I 2 statistics were used to assess heterogeneity across all studies (Higgins, Thompson, Deeks, & Altman, Reference Higgins, Thompson, Deeks and Altman2003). Publication bias was assessed by visual inspection of funnel plots and Begg's Test.
Subgroup analyses were conducted, using the following categorical study characteristics: (1) study of continents (Africa, Asia, Europe, North America, or Oceania); (2) psychiatric diagnosis (bipolar disorder, major depression, or schizophrenia); (3) duration of follow-up (0–10, >10–20, or >20 years); (4) sex (male or female); and (5) suicide methods (jumping, hanging, poisoning, or other). Changes in follow-up time and suicide rates were analyzed using a locally weighted scatter-plot smoothing (LOESS) curve, which produces a smooth fit to the data and reduces the influence of extreme outliers (Cleveland, Reference Cleveland1979). For assessments of differences in suicide rates by sex, suicide rate ratio was estimated. Univariate meta-regression models were also conducted to assess the association between study characteristics (year of publication, mean age, proportion of female) and the pooled suicide rate estimate. Statistical tests were two-sided and a significance level of p < 0.05 was used throughout.
Results
A total of 5 014 records were identified through databases and reference searches, as shown in the PRISMA flow diagram (Fig. 1). After the removal of irrelevant title, abstracts, and duplicates, 354 articles remained for full review. Ultimately, 313 articles were excluded, leaving 41 that met eligibility (Abdel-Baki et al., Reference Abdel-Baki, Lesage, Nicole, Cossette, Salvat and Lalonde2011; Allebeck & Wistedt, Reference Allebeck and Wistedt1986; Almeida, Hankey, Yeap, Golledge, & Flicker, Reference Almeida, Hankey, Yeap, Golledge and Flicker2018; Antolín-Concha et al., Reference Antolín-Concha, Lähteenvuo, Vattulainen, Tanskanen, Taipale, Vieta and Tiihonen2020; Björkenstam, Björkenstam, Hjern, Bodén, & Reutfors, Reference Björkenstam, Björkenstam, Hjern, Bodén and Reutfors2014; Black & Fisher, Reference Black and Fisher1992; Brown, Inskip, & Barraclough, Reference Brown, Inskip and Barraclough2000; Carlborg, Jokinen, Nordström, Jönsson, & Nordström, Reference Carlborg, Jokinen, Nordström, Jönsson and Nordström2010; Ceskova, Prikryl, & Kasparek, Reference Ceskova, Prikryl and Kasparek2011; Coryell & Young, Reference Coryell and Young2005; Crump, Sundquist, Winkleby, & Sundquist, Reference Crump, Sundquist, Winkleby and Sundquist2013; Dennehy et al., Reference Dennehy, Marangell, Allen, Chessick, Wisniewski and Thase2011; Díaz-Fernández, Frías-Ortiz, & Fernández-Miranda, Reference Díaz-Fernández, Frías-Ortiz and Fernández-Miranda2020; Dutta et al., Reference Dutta, Boydell, Kennedy, Jim VAN, Fearon and Murray2007; Hansson et al., Reference Hansson, Joas, Pålsson, Hawton, Runeson and Landén2018; Hayes, Marston, Walters, King, & Osborn, Reference Hayes, Marston, Walters, King and Osborn2017; Høye, Jacobsen, & Hansen, Reference Høye, Jacobsen and Hansen2011; Isometsä, Sund, & Pirkola, Reference Isometsä, Sund and Pirkola2014; Kaplan, Harrow, & Clews, Reference Kaplan, Harrow and Clews2016; Kim et al., Reference Kim, Jang, Chun, Lee, Han and Park2017; Kiviniemi et al., Reference Kiviniemi, Suvisaari, Koivumaa-Honkanen, Häkkinen, Isohanni and Hakko2013; Limosin, Loze, Philippe, Casadebaig, & Rouillon, Reference Limosin, Loze, Philippe, Casadebaig and Rouillon2007; Lin, Chung, Chen, & Chien, Reference Lin, Chung, Chen and Chien2019; Loas, Azi, Noisette, Legrand, & Yon, Reference Loas, Azi, Noisette, Legrand and Yon2009; Lui, Reference Lui2009; Newman & Bland, Reference Newman and Bland1991; Olfson, Gerhard, Huang, Crystal, & Stroup, Reference Olfson, Gerhard, Huang, Crystal and Stroup2015; Oquendo et al., Reference Oquendo, Bongiovi-Garcia, Galfalvy, Goldberg, Grunebaum, Burke and Mann2007; Osby, Brandt, Correia, Ekbom, & Sparén, Reference Osby, Brandt, Correia, Ekbom and Sparén2001; Østergaard, Nordentoft, & Hjorthøj, Reference Østergaard, Nordentoft and Hjorthøj2017; Persons et al., Reference Persons, Coryell, Solomon, Keller, Endicott and Fiedorowicz2018; Plans, Nieto, Benabarre, & Vieta, Reference Plans, Nieto, Benabarre and Vieta2019; Ran et al., Reference Ran, Chan, Chen, Mao, Hu, Tang and Conwell2009; Schneider, Philipp, & Müller, Reference Schneider, Philipp and Müller2001; Simon, Hunkeler, Fireman, Lee, & Savarino, Reference Simon, Hunkeler, Fireman, Lee and Savarino2007; Teferra et al., Reference Teferra, Shibre, Fekadu, Medhin, Wakwoya, Alem and Jacobsson2011; Tsai, Lee, & Chen, Reference Tsai, Lee and Chen1999; Tseng, Cheng, Lee, & Lee, Reference Tseng, Cheng, Lee and Lee2006; Tsoi & Wong, Reference Tsoi and Wong1991; Webb, Långström, Runeson, Lichtenstein, & Fazel, Reference Webb, Långström, Runeson, Lichtenstein and Fazel2011; Wiersma, Nienhuis, Slooff, & Giel, Reference Wiersma, Nienhuis, Slooff and Giel1998).

Fig. 1. Flowchart of searches for studies reporting rates of suicide among people with serious mental illness.
Study characteristics
The key characteristics are summarized in Table 1. The 41 studies reported 7 852 suicides during 6 531 931 person-years. The mean age of participants was reported in 26 studies, ranged from 21.9 to 72.3 years. The proportion of female participants in the study sample was reported in 36 studies, with a total of 640 277 female participants among 1 359 503 participants. The median duration of follow-up was 10.0 years (range 1.2–24.6 years; interquartile range 5.0–14.0 years). Two studies only enrolled adult men (Almeida et al., Reference Almeida, Hankey, Yeap, Golledge and Flicker2018; Ceskova et al., Reference Ceskova, Prikryl and Kasparek2011).
Table 1. Key characteristics of the included studies

The largest study (Olfson et al., Reference Olfson, Gerhard, Huang, Crystal and Stroup2015) in this meta-analysis included 1 138 853 cases, and the smallest study (Tseng et al., Reference Tseng, Cheng, Lee and Lee2006) identified 67 cases. Many studies captured a representative sample using nationwide databases. The most frequently studied diagnostic outcome was schizophrenia (n = 24), followed by bipolar disorder (n = 16) and major depression (n = 4). The 41 studies included data from 18 countries and all studies were done in a single country. Seven samples were from Asian countries, 23 from mainland Europe, and nine from North America. There was one sample each from Africa and Oceania. Overall, no studies were deemed to be at high risk of bias, 15 (36.6%) were at moderate risk of bias, and 26 (63.4%) were at low risk of bias (online Supplementary eTable 2).
Meta-analysis
The pooled suicide rate among people with serious mental illness was 312.8 per 100 000 person-years (95% CI 230.3–406.8 per 100 000 person-years), with substantial heterogeneity (I 2 = 99.4%; p < 0.001) (Fig. 2). Visual inspection of the funnel plot symmetry and Begg's Test (p = 0.238) suggested an absence of publication bias (online Supplementary eFig. 1). Meta-regression analysis found publication year (p = 0.454), mean age (p = 0.870), or proportion of female (p = 0.687) was not significantly associated with the pooled suicide rate (online Supplementary eFig. 2).

Fig. 2. Forest plot of pooled suicide rate among people with serious mental illness.
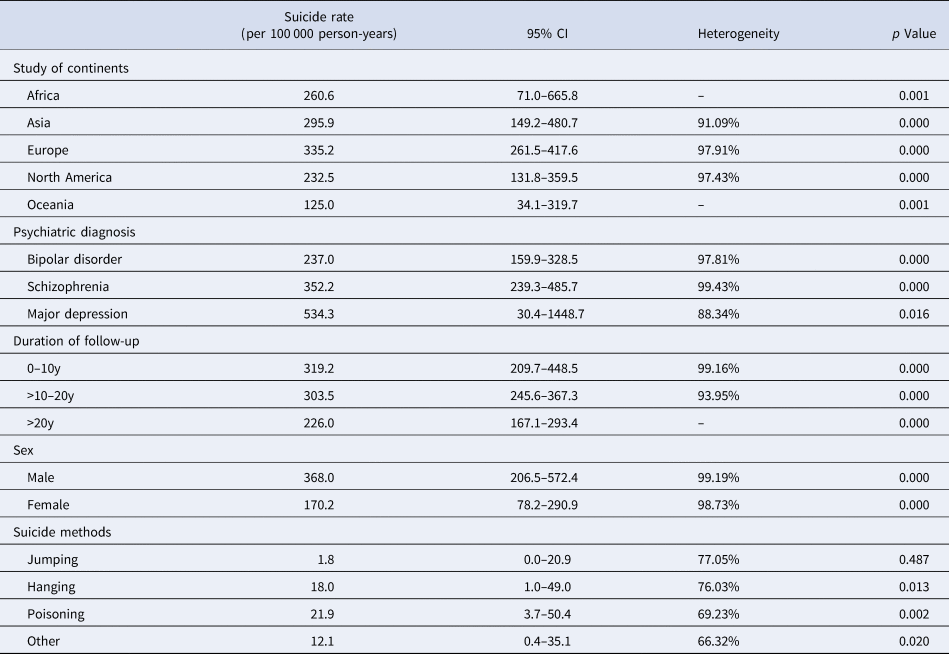
Europe was reported to have the highest pooled suicide rate [335.2 per 100 000 person-years (95% CI 261.5–417.6 per 100 000 person-years)], followed by Asia [295.9 per 100 000 person-years (95% CI 149.2–480.7 per 100 000 person-years)], Africa [260.6 per 100 000 person-years (95% CI 71.0–665.8 per 100 000 person-years)], North America [232.5 per 100 000 person-years (95% CI 131.8–359.5 per 100 000 person-years)], and Oceania [125.0 per 100 000 person-years (95% CI 34.1–319.7 per 100 000 person-years)] (Table 2).
Table 2. Subgroup analyses according to study characteristics

The suicide rates of bipolar disorder were available from 16 studies and varied from 125.0 per 100 000 person-years (95% CI 34.1–319.7 per 100 000 person-years) in Oceania to 291.9 (95% CI 198.4–403.0 per 100 000 person-years) in Europe, with a pooled estimate of 237.0 per 100 000 person-years (95% CI 159.9–328.5 per 100 000 person-years). The suicide rates of major depression were available from four studies and varied from 180.3 per 100 000 person-years (95% CI 116.2–256.2 per 100 000 person-years) in North America to 1282.1 (95% CI 32.5–6937.3 per 100 000 person-years) in Asia, with a pooled estimate of 534.3 per 100 000 person-years (95% CI 30.4–1448.7 per 100 000 person-years). The suicide rates of schizophrenia were available from 24 studies and varied from 260.6 per 100 000 person-years (95% CI 71.0–665.8 per 100 000 person-years) in Africa to 421.1 (95% CI 244.3–642.6 per 100 000 person-years) in Asia, with a pooled estimate of 352.2 per 100 000 person-years (95% CI 239.3–485.7 per 100 000 person-years) (Table 2; online Supplementary eFig. 3).
The pooled suicide rate with a follow-up of 10 years or less was 319.2 per 100 000 person-years (95% CI 209.7–448.5 per 100 000 person-years) and decreased thereafter in studies with follow-up of 10–20 years [303.5 per 100 000 person-years (95% CI 245.6–367.3 per 100 000 person-years)] and over 20 years [226.0 per 100 000 person-years (95% CI 167.1–293.4 per 100 000 person-years)] (Table 2). Figure 3 showed a downward trend in the suicide rate estimates over time.

Fig. 3. Suicide rate estimates among people with serious mental illness over follow-up time.
Seventeen studies reported suicide rates in males, with a pooled suicide rate of 368.0 per 100 000 person-years (95% CI 206.5–572.4 per 100 000 person-years). Fifteen studies reported suicide rates in females, with an estimate of 170.2 per 100 000 person-years (95% CI 78.2–290.9 per 100 000 person-years) (Table 2). For all serious mental illness, suicide rate ratios in males compared with females were available from 14 studies, with a pooled suicide rate ratio of 1.90 (95% CI 1.60–2.25). Excess risk in males was found for bipolar disorder [1.88 (95% CI 1.37–2.59)] and schizophrenia [2.01 (95% CI 1.60–2.53)] (online Supplementary eFig. 4).
There were 10 studies presenting data on suicide methods. The most common suicide method was poisoning [21.9 per 100 000 person-years (95% CI 3.7–50.4 per 100 000 person-years)], followed by hanging [18.0 per 100 000 person-years (95% CI 1.0–49.0 per 100 000 person-years)], other [12.1 per 100 000 person-years (95% CI 0.4–35.1 per 100 000 person-years)], and jumping [1.8 per 100 000 person-years (95% CI 0.0–20.9 per 100 000 person-years)] (Table 2).
Discussion
This study presented a meta-analysis of suicide among people with serious mental illness from 41 studies. The results of this meta-analysis indicated a pooled suicide rate estimate of 312.8 per 100 000 person-years. A previous study had found that the postdischarge suicide rate was 484 per 100 000 person-years (Chung et al., Reference Chung, Ryan, Hadzi-Pavlovic, Singh, Stanton and Large2017), which is higher than our study. This is reasonable because the immediate risk of suicide after discharge is high (Haglund, Lysell, Larsson, Lichtenstein, & Runeson, Reference Haglund, Lysell, Larsson, Lichtenstein and Runeson2019). However, people with serious mental illness have excess suicide rate relative to the general population. Compared with the general population, age-and-sex-standardized mortality ratio for suicide is increased by 5–10 times among people with serious mental illness (Das-Munshi et al., Reference Das-Munshi, Chang, Dutta, Morgan, Nazroo, Stewart and Prince2017). The suicide rate in the US general population is only 11.54 per 100 000 person-years (Nie et al., Reference Nie, O'Neil, Liao, Lu, Aune and Wang2021). Even among cancer patients, the suicide rate is only 39.72 per 100 000 person-years (Du et al., Reference Du, Shi, Yu, Liu, Jin, Yan and Chen2020), highlighting the importance of addressing the mental health needs of this population. Additionally, we also found a downward trend in the suicide rate estimates over follow-up time and this result is consistent with Chung et al.'s research (Chung et al., Reference Chung, Ryan, Hadzi-Pavlovic, Singh, Stanton and Large2017).
In our study, major depression has the highest pooled suicide rate while bipolar disorder has the lowest suicide rate. A systematic review and meta-analysis also found that the mean prevalence of bipolar disorder among suicide victims is markedly lower than the mean prevalence of major depressive disorder (Cho, Na, Cho, Im, & Kang, Reference Cho, Na, Cho, Im and Kang2016). There are observed variations in suicide rates by continents, and Europe is leading in this comparison. The highest suicide rate in Europe is reasonable because this continent has the highest prevalence of heavy alcohol use (Peacock et al., Reference Peacock, Leung, Larney, Colledge, Hickman, Rehm and Degenhardt2018), which is a potent risk factor for suicide (Edwards, Ohlsson, Sundquist, Sundquist, & Kendler, Reference Edwards, Ohlsson, Sundquist, Sundquist and Kendler2020; Foster, Reference Foster2013). Wide cross-national variations could be partly attributed to variations in the organization and provision of mental health service (Shah, Bhandarkar, & Bhatia, Reference Shah, Bhandarkar and Bhatia2010) and underreporting and misclassification of suicide (partly related to legal and cultural factors) (Jacob et al., Reference Jacob, Sharan, Mirza, Garrido-Cumbrera, Seedat, Mari and Saxena2007).
Generally, males were found to have an excess risk of suicide in our study. Connecting suicidal individuals to mental health service is a critical component of suicide prevention efforts, but a previous study (Walby, Myhre, & Kildahl, Reference Walby, Myhre and Kildahl2018) has found that compared with females, males had significantly less contact with inpatient or outpatient mental health services. Conformity to traditional masculine norms and mental health-related stigma may be key deterrents for them to seek help (Clement et al., Reference Clement, Schauman, Graham, Maggioni, Evans-Lacko, Bezborodovs and Thornicroft2015; Seidler, Dawes, Rice, Oliffe, & Dhillon, Reference Seidler, Dawes, Rice, Oliffe and Dhillon2016). Moreover, a lack of perceived need for services, preference for self-management, fear of hospitalization, and structural factors, such as time and finances, are also identified as barriers to mental health service utilization (Hom, Stanley, & Joiner, Reference Hom, Stanley and Joiner2015).
It was also observed that poisoning is the most common suicide method for people with serious mental illness. Suicide methods often reflect specific socio-cultural, economic, and religious situations (Wu, Chen, & Yip, Reference Wu, Chen and Yip2012). The agricultural Green Revolution introduces highly hazardous pesticides into poor rural communities and pesticide self-poisoning becomes the leading cause of suicide in low-income and middle-income countries (Karunarathne, Gunnell, Konradsen, & Eddleston, Reference Karunarathne, Gunnell, Konradsen and Eddleston2020), accounting for 14–20% of all global suicides (Mew et al., Reference Mew, Padmanathan, Konradsen, Eddleston, Chang, Phillips and Gunnell2017). However, in the USA, firearms were the most commonly used suicide method among males with serious mental illness, while self-poisoning accounted for a majority of suicide deaths in females (Schmutte et al., Reference Schmutte, Costa, Hammer and Davidson2021). Jumping was found to be the most common method of suicide among psychiatric patients in Korea (Park et al., Reference Park, Ahn, Na, Kim, Yoon, Park and Hong2013). Therefore, comparisons by continents and other characteristics are needed in further study.
Although publication year was not the source of heterogeneity from meta-regression, a downward trend in the suicide rate estimates was observed in recent decades. Similarly, a previous study (Naghavi, Reference Naghavi2019) also revealed that age-standardized mortality rates for suicide have greatly reduced since 1990. In many countries, the government has realized the importance of suicide prevention and launched national prevention programs to encourage research, detection, treatment, and management of people at risk (Mann et al., Reference Mann, Apter, Bertolote, Beautrais, Currier, Haas and Hendin2005; van der Feltz-Cornelis et al., Reference van der Feltz-Cornelis, Sarchiapone, Postuvan, Volker, Roskar, Grum and Hegerl2011; Zalsman et al., Reference Zalsman, Hawton, Wasserman, van Heeringen, Arensman, Sarchiapone and Zohar2016). As the science of suicide prevention progresses and the number and quality of studies increase (Bolton, Gunnell, & Turecki, Reference Bolton, Gunnell and Turecki2015), more and more nonpharmacologic and pharmacologic interventions are performed to prevent suicide and reduce suicide behaviors in at-risk people (D'Anci, Uhl, Giradi, & Martin, Reference D'Anci, Uhl, Giradi and Martin2019).
Social support is a social network's provision of psychological and material resources, which can make individuals more resilient when they are exposed to traumas (Southwick et al., Reference Southwick, Sippel, Krystal, Charney, Mayes and Pietrzak2016). Family members should help young patients with first-episode psychosis to seek treatment (Martin et al., Reference Martin, Ciccone Giacon, Giacchero Vedana, Guidorizzi Zanetti, Fendrich and Frari Galera2018). In addition, most individuals have health system contact prior to suicide, which means opportunities for suicide prevention in primary care or medical specialty settings (Ahmedani et al., Reference Ahmedani, Simon, Stewart, Beck, Waitzfelder, Rossom and Solberg2014). Therefore, it is important to introduce various service changes related to ward safety, community services, training, and policy and guidance (Kapur et al., Reference Kapur, Ibrahim, While, Baird, Rodway, Hunt and Appleby2016; Leung, Chow, Ip, & Yip, Reference Leung, Chow, Ip and Yip2019).
Strengths
Our study has a number of strengths. First, this is the first systematic review and meta-analysis of suicide rates among people with serious mental illness to have been conducted. Given the poor lifetime consequences of this disease and high risk of suicide of this population, a comprehensive picture of existing evidence of the suicide deaths among this population is extremely valuable. Second, several methods were employed to ensure the quality of this review. Databases were searched using a thorough string of keywords, along with the screening reference lists to limit the number of eligible articles missed. Articles were quality assessed using a valid and reliable checklist tool and were excluded if they were not of sufficient quality, ensuring that only the best quality articles were included.
Limitations
However, limitations in the review must be noted. First, substantial statistical heterogeneity was found across the included studies. Although subgroup analyses and meta-regression analyses were conducted, the source of heterogeneity was unable to be explained, which might be attributable to factors that were not reported in the primary research. Second, almost all the research came from high-income economies of Asia, Europe, and North America, and our results might not be representative of suicide in low- and middle-income countries. Third, only four of the included studies reported suicide rates of major depression, limiting the generalizability of the suicide rate estimates. Fourth, the number of articles that reported suicide method is too small, so we cannot make further comparisons by continent or other study characteristics. Finally, there is a lack of reporting of age data in the majority of the included studies, which needs further research in this topic.
Conclusions
This study found that people who have serious mental illness were at great risk of suicide, calling for the implementation of psychological assessment and monitoring. Measures to prevent suicidal pesticide ingestions are required to reduce the risk of self-poisoning. To better understand the epidemiology of suicides in this population, additional work is necessary to delineate region and age differences in suicide deaths among people with serious mental illness.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721001549.
Author contributions
Xue-Lei Fu developed the search strategy, drafted the published protocol, led data extraction and critical appraisal, and drafted the final manuscript. Yan Qian and Xiao-Hong Jin contributed to the article screening and critical appraisal and critically reviewed the manuscript. Hai-Rong Yu and Hua Wu contributed to the data extraction and critically reviewed the manuscript. Lin Du contributed to the design of the study interpretation of analyzed data and statistical calculations.
Hong-Lin Chen and Ya-Qin Shi contributed to the design of the study, was the guarantor, developed the search strategy, performed, supervised and refereed data extraction, reviewed data analysis, contributed to drafting the manuscript, and critically reviewed the final manuscript. Hong-Lin Chen and Ya-Qin Shi are corresponding authors of this study. All authors approved the final manuscript as submitted.
Financial support
This study was supported by the Humanities and Social Sciences Research Planning Fund Project of the Ministry of Education (Project Number 20YJAZH007). This study was supported by the Social and People's Livelihood Technology in Nantong city-General Project (Project Number MS12019038).
Conflict of interest
None.