


Diet and nutrition are important in maintaining health and preventing chronic diseases( 1 ). According to the WHO, unhealthy diets, along with smoking and sedentary lifestyles, are the most important modifiable CVD risk factors( 2 ). Among other unhealthy dietary behaviours, high sodium intake is closely associated with elevated blood pressure and adverse cardiovascular health( Reference Appel, Champagne and Harsha 3 , Reference Sacks, Svetkey and Vollmer 4 ). Given the high sodium intake at a global level and the high prevalence of hypertension( Reference Lawes, Vander Hoorn and Law 5 , 6 ), it is important to develop effective intervention strategies to reduce sodium intake( Reference Bibbins-Domingo, Chertow and Coxson 7 ).
Because of modern lifestyles, many populations depend on foods prepared outside the home, and Koreans are no exception. In South Korea, the proportion of energy and nutrients consumed while eating out has increased along with economic changes and the growth of the food-service industry. Recent data show that food eaten away from home accounted for more than half of daily total protein, fat and sodium intakes( Reference Kwon and Ju 8 ). Among these eating-out meals, catered lunches and dinners at worksites play a pivotal role because of the long working hours in South Korea( 9 ).
The importance of worksite settings as a health promotion venue is well understood( Reference McLeroy, Bibeau and Steckler 10 , Reference Almeida, Wall and You 11 ). Intervening in worksites has shown the potential to improve employees’ dietary behaviours( Reference Beresford, Thompson and Feng 12 ), physical activity( Reference Auweele, Boen and Schapendonk 13 , Reference Harden, Peersman and Oliver 14 ), smoking cessation( Reference Armitage 15 ) and obesity status( Reference Anderson, Quinn and Glanz 16 ). Specifically, previous studies of employees showed positive outcomes in improving their nutritional knowledge and motivation to choose healthier diets through education and support sessions( Reference Levin, Ferdowsian and Hoover 17 – Reference Shin, Lee and Jun 19 ).
In addition to working with employees at an individual level, the social ecological model (SEM) provides a theoretical framework for working with the environments in which employees make health decisions. The SEM emphasizes the interrelationships among various factors at individual and environmental levels( Reference Stokols 20 ). A number of environmental interventions based on this model have been attempted to improve the nutritional status of target populations( Reference Engbers, van Poppel and Chin A Paw 21 ). However, most of the previous intervention studies targeted fruit and vegetable intake and fat intake( Reference Beresford, Thompson and Feng 12 , Reference Steenhuis, Van Assema and Van Breukelen 22 ). Very few studies included sodium components( Reference Geaney, Harrington and Fitzgerald 23 , Reference Perlmutter, Canter and Gregoire 24 ).
Given the importance of lowering sodium intake in most world populations( Reference Brown, Tzoulaki and Candeias 25 ), there is a serious gap in previous worksite environmental interventions. Two qualitative formative studies mainly assessed employees’ perceptions of their worksite food environments( Reference Devine, Nelson and Chin 26 , Reference Ahn, Kim and Kim 27 ). These previous studies mentioned that employees supported healthier cafeteria and catering options and changes to make healthful foods more available and more clearly labelled. However, the difficulties catering companies face in serving healthier meals, especially reduced-sodium meals (RSM), remain unknown.
The high prevalences of hypertension and CVD along with the high levels of sodium in dishes at food-service establishments( Reference Park, Jeong and Lee 28 – Reference Brewster, Berentzen and van Montfrans 30 ) have necessitated special action from the government, restaurants and food catering companies in many developed countries( Reference Scourboutakos and L’Abbe 31 – Reference Webster, Dunford and Hawkes 34 ). In 2011, the central and local governments in South Korea began programmes and policies that aimed to effectively alter food environments, specifically the sodium content in away-from-home foods( 35 ). The central government, mainly the Korea Ministry of Food and Drug Safety, recruited major food catering companies and franchise restaurants to initiate voluntary sodium-reduction programmes( Reference Hong, Lee and Kim 36 , Reference Kim 37 ).
For worksite cafeterias, which are the main focus of the current paper, the Korea Ministry of Food and Drug Safety has been conducting workshops for introducing possible environmental strategies to reduce the sodium content of cafeteria meals. These strategies include: (i) replacing regular soup with other low-sodium alternatives at least once per week; (ii) exchanging large soup bowls with smaller ones to reduce portion size; (iii) removing salt shakers from tables; (iv) providing more raw vegetables and fruits with high potassium; (v) adding extra spices to provide more flavours when cooking; and (vi) using low-sodium kimchi (fermented pickled cabbage) and other basic ingredients in Korean cuisine (e.g. red pepper paste and soyabean paste). Educational materials targeting cafeteria customers were also distributed, if requested( 35 ). The resulting lower-sodium meals were not specific to any type of meal and varied by site.
After one year of voluntary programmes, the government funded the present study to learn from the on-site food-service personnel who have been participating in those programmes. The aim was to learn how to design and implement more effective policies for lowering sodium intake among working populations. Using in-depth interviews with dietitians and headquarters managers, we aimed to understand the issues surrounding serving RSM in commercial worksite cafeterias. The main research questions of the present paper are as follows: (i) What are the facilitators of and barriers to serving RSM in commercial worksite cafeterias? (ii) Based on these facilitators and barriers, what are the potential policies or programmes that need to be developed for lowering sodium content in meals served in worksite cafeterias?
Methods
General study design and theoretical framework
We employed in-depth interviews with key personnel of catering companies as a first step in expanding RSM in worksite cafeterias. We used the SEM as a guiding framework( Reference McLeroy, Bibeau and Steckler 10 , Reference Glanz, Rimer and Viswanath 38 ) when preparing the interview guide (Fig. 1 and Table 1). For example, we attempted to understand both the individual and environmental factors that enabled or hindered serving RSM in worksite cafeterias. Table 1 presents the interview guide that was used for the study.
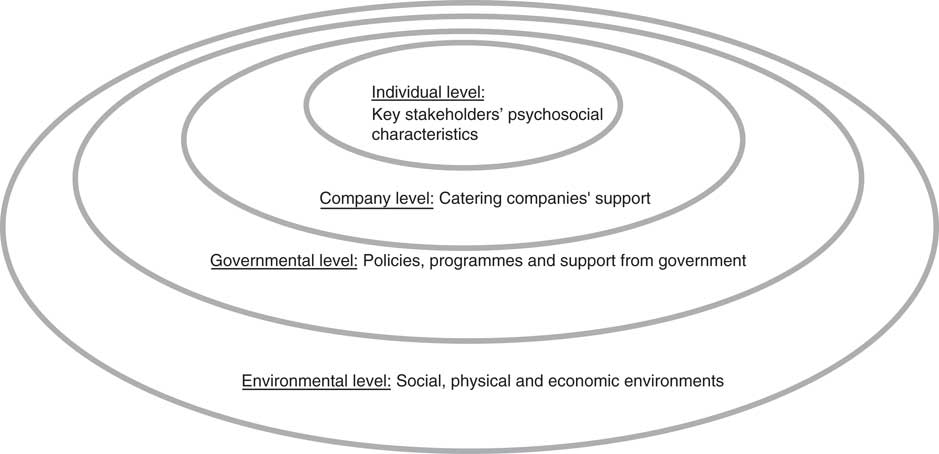
Fig. 1 The social ecological model as a theoretical framework for understanding barriers to and facilitators of serving reduced-sodium meals in worksite cafeterias in South Korea
Table 1 Interview guide for in-depth one-on-one interviews and natural group interviews for understanding barriers to and facilitators of lowering sodium content in worksite cafeterias in South Korea

In the current manuscript, we use the terms ‘reduced-sodium’ and ‘less sodium’ interchangeably. For cafeteria meals, the Korea Ministry of Food and Drug Safety recommends 1300 mg/meal for the sodium level in RSM in response to the high current sodium levels (2200–2800 mg/meal) in cafeteria meals( Reference Park, Jeong and Lee 28 ). At this early stage of the government initiative, however, we defined RSM as any meals that had lower sodium levels than conventional meals.
Recruitment and interview process
A total of nineteen interviews with twenty-five participants from ten catering companies were conducted between May and September 2014. Among the nineteen interviews, fourteen were one-on-one and five were group interviews with dietitians and headquarters managers. Sixteen on-site dietitians (employed by catering companies) and nine managers from the companies’ headquarters participated in the interviews. The list of interviews and participants is shown in Table 2.
Table 2 Interview overview and participant information
F, female; M, male; NA, not applicable.
The Korea Ministry of Food and Drug Safety provided the contact information of managers at ten major catering companies with the highest sales in the market and the managers at each company suggested two customer sites where on-site dietitians had attempted to serve RSM for the past year. These purposefully selected participating sites involved customers who reported being more open to RSM. We chose on-site head dietitians and headquarters managers as our key informants because they are responsible for menu planning, choosing recipes for the planned menus and purchasing ingredients. In addition to these roles, head dietitians maintain many other responsibilities related to cafeteria management and therefore may be more appropriately described as ‘managers’. However, the most important qualification for this job is having a dietetic licence, so they are referred to conventionally as ‘dietitians’. Both head dietitians and managers had at least 4 years of college education in dietetics along with food-service management subjects, and headquarters managers often had previous experience as on-site dietitians before becoming managers at headquarters.
All of the interviews with on-site dietitians occurred either in the cafeteria halls or in the dietitians’ offices, which were mostly adjacent to kitchens or cafeteria halls. For the managers at the headquarters, the interviews occurred either in the managers’ offices or at one of the customer sites that the managers oversaw. The type of cafeterias that the catering companies served varied from hospital cafeterias to cafeterias in department store buildings. The types of all the participating customer sites are presented in Table 2.
The majority of interviews were scheduled immediately after the peak lunch time (11.30–13.30 hours) and the interviewers (the authors) briefly observed each site while lunch was being served. We aimed for one-on-one interviews with all of the participants, but when the interviewee wanted to talk with other participants for administrative reasons, mostly time constraints, we conducted group interviews. We encouraged the on-site dietitians to speak their own thoughts and give suggestions when the managers from headquarters were present during the interviews (interviews #6, #15 and #18).
All interviews took approximately 40 min to 1 h to complete and written consent forms were obtained from all participants. The interviews were digitally recorded for transcription when the participants approved. All of the protocols for the study were approved by the Institutional Review Board of Hanyang University. Once we transcribed the interviews verbatim, the interviewers reviewed the transcripts for accuracy.
Analysis
The SEM and preselected constructs from the theoretical model guided the coding of the interviews (Fig. 1). Based on the preselected constructs from the theoretical model, we developed a codebook, a guideline and a manual for coding text-based data( Reference Pope, Ziebland and Mays 39 ). Two authors (S.P. and J.L.) coded the data using the codebook, reviewed the codes and discussed them until final codes and themes were determined. During this process, we used a text-based data analysis package for data management (ATLAS.ti version 6·0; Scientific Software Development GmbH, Berlin, Germany).
Results
Facilitators of and barriers to serving RSM were summarized into four major themes from the perspectives of the SEM (Fig. 2). We began with individual-level factors, such as the psychosocial characteristics of key stakeholders (Theme 1) and food-service personnel’s skills and techniques related to preparing RSM (Theme 2). Then, we moved to various policy and environmental factors for Themes 3 and 4.
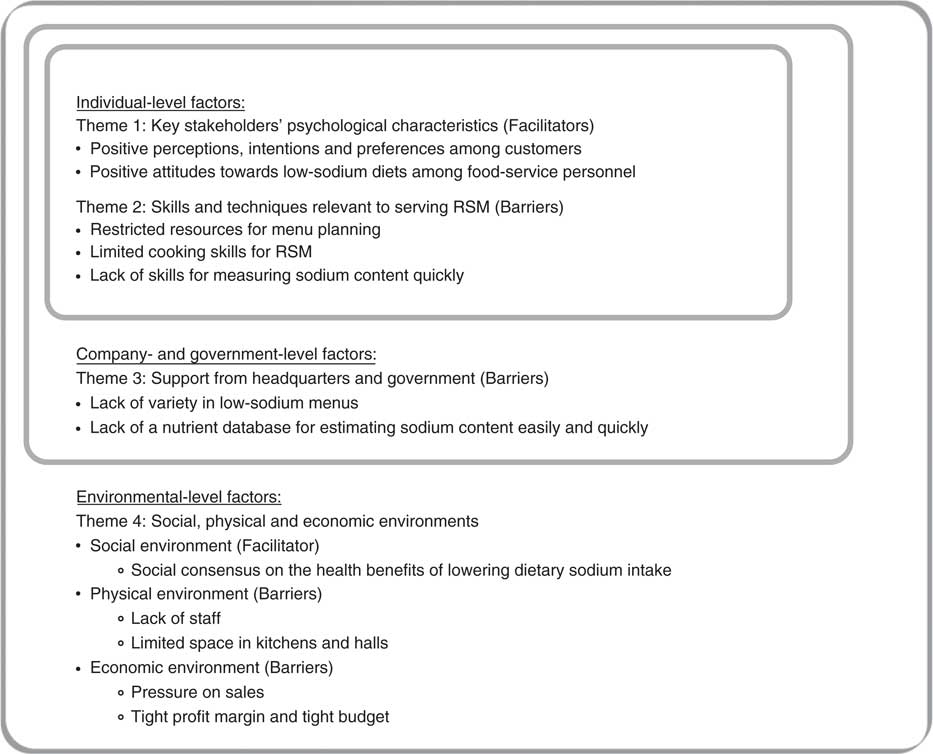
Fig. 2 Key barriers to and facilitators of serving reduced-sodium meals (RSM) in worksite cafeterias in South Korea
Theme 1: Key stakeholders’ psychosocial characteristics
Perceptions, intentions and preferences among customers
The key stakeholders in this setting include customers (mostly office workers and some manual workers, as well as some executives) and food-service personnel. Interviewees mentioned that the customers’ perceptions, intentions and preferences regarding RSM are among the most important factors that enable the provision of less salty meals. If the customers do not perceive the importance of eating less salty foods and do not choose them, it is impossible to serve reduced-sodium foods despite dietitians’ good intentions (quote #1 in Table 3).
Table 3 Selected quotations from the interviews
In contrast, if customers want reduced-sodium foods, dietitians see no reasons not to serve the foods. In particular, when high-level customers, such as company executives, understand the importance of sodium content in the food for their employees, it is very likely that the company will officially request reduced-sodium foods from the catering company.
Most office workers and some manual workers understand the health benefits of reduced-sodium foods. However, knowledge regarding RSM does not always align with the practice of choosing them at mealtime. From dietitians’ observations, low-sodium lunches remain difficult to sell to many customers, with the exception of young women and older customers. Other than age and gender, as the dietitians mentioned, perceptions and preferences can vary by job type. Low-sodium diets could be more acceptable to and preferred by office workers compared with manual workers (quote #2 in Table 3).
Attitudes towards low-sodium diets among food-service personnel
Knowledge and attitudes towards RSM among food-service personnel also may affect the provision of these foods in cafeterias. Most on-site dietitians and managers expressed the importance of providing RSM in worksite cafeterias. This positive attitude towards reduced-sodium diets is a good facilitator for providing healthier menus in cafeterias. One dietitian mentioned that the feeling of self-satisfaction was the best reward when she served RSM (quote #3 in Table 3).
However, when the dietitians work with other food-service personnel who do not see low sodium as important, it can sometimes be challenging to persuade them to do the extra work that can be associated with preparing reduced-sodium recipes compared with conventional recipes. The extra work typically involves making dishes from scratch, such as sauces, dressings, dumplings, meat products and pickled vegetables (e.g. kimchi).
Theme 2: Skills and techniques relevant to serving reduced-sodium meals
In addition to psychosocial factors, the interviewees mentioned some technical difficulties. When the dietitians and managers at headquarters attempted to serve foods that have lower sodium content, they often found it very challenging to maintain the palatability of the food. Without sacrificing taste, it is not easy to serve nutritionally balanced, low-sodium meals within their budgets and resources. Therefore, they mentioned that they would like to have resources for menu planning and training sessions on skills for preparing low-sodium meals.
Another difficulty in providing RSM was that most of the dietitians and food-service personnel did not know an accurate way to measure sodium content. They knew that it was best to blend all of the foods served except for clear soups and to follow the protocols as they would in laboratories, but when they had more than one hundred and sometimes more than one thousand customers to serve within two hours, the task of monitoring the actual sodium content of every dish seemed impossible (quote #4 in Table 3).
Theme 3: Support from headquarters and government
Lack of variety in low-sodium menus
Along with the lack of skills and techniques among on-site personnel, interviewees mentioned that more support is needed from the headquarters and the government. The most frequently mentioned issue was the low variety in the RSM. As mentioned earlier in the Methods and in Theme 1, for the on-site dietitians, there are many tasks involved in running a cafeteria in addition to menu planning and lowering sodium content. In South Korea, dietitians at food-service establishments are entirely responsible for running a cafeteria. The interviewed dietitians said that the title dietitian can be misleading because planning nutritionally balanced meals is only one of their many responsibilities.
Hence, if there are no pre-tested reduced-sodium recipes that chefs can use immediately, it is difficult for on-site staff to develop these recipes. Moreover, depending on the characteristics of the customers, standard menu recipes may need to be modified. This task can be difficult without sufficient staff or time. Many of the interviewed dietitians stated that given the limited number of low-sodium recipes and limited staff, simply reducing the amount of salt in the regular standard recipes was the only thing they could try. If this approach is used, there could be many complaints from customers that ‘the food is too bland and not tasty’. The dietitians understood that they should modify the whole recipe, but for most of the dietitians who participated in the interviews, this approach was beyond their capabilities because of their many other roles and responsibilities.
The managers who are responsible for developing new menus at catering companies’ headquarters also expressed some difficulties. For smaller companies, only one or two workers develop the menus for entire cafeterias (mostly hundreds) and reduced-sodium foods are only one type of needed menu item (seasonal menus and other healthy menus also should be updated regularly). Larger catering companies reported better conditions (seven to ten professional cooks to develop new menus). However, they are hesitant to make low-sodium versions of popular menu items because they might lose customers because of the taste (quote #5 in Table 3).
Lack of a nutrient database for estimating sodium content easily and quickly
Another issue that the dietitians mentioned is the lack of a reliable database for estimating sodium content. As mentioned in Theme 2, actual measurement is not easy. The interviewees also requested a method to estimate sodium content using recipes and nutrient databases, but there are no reliable systems currently available (quote #6 in Table 3).
Theme 4: Social, physical and economic environments
Finally, there are some factors that can be categorized as environmental-level facilitators and barriers. We further specified the frequently mentioned factors related to social, physical and economic environments.
Social environment
Owing to central and local governments’ ongoing efforts to reduce sodium intake, the interviewees mentioned a social consensus on the health benefits of lowering dietary sodium intake. As a result, some customers had begun to appreciate RSM in the cafeterias. Most of the catering companies we interviewed mentioned that serving healthier menus with fewer calories, low salt and more fresh ingredients is essential for surviving in the competitive catering market (quote #7 in Table 3).
In addition, managers at catering companies’ headquarters mentioned that more dietitians at their customer sites had begun to request low-sodium menus. From these interviews, we observed that the social environment is changing in a positive direction and that this change clearly helps to improve the food environments in worksite cafeterias.
Physical environment
In contrast to social environments, which are changing positively, the physical surroundings in food-service establishments are not as conducive to serving RSM. For example, many interviewees mentioned that if there were more staff and more space in their kitchens and halls, they would attempt to serve RSM more actively. One of the more extreme cases was a cafeteria that served employees at a department store in a busy district in Seoul. Because of the limited number of parking spaces at the store, the company decided to take some of the employee cafeteria space to make more parking spots. This space reduction resulted in a decrease from two menus to one lunch menu for their employees. Consequently, the dietitian at that cafeteria could not serve RSM more frequently because she had to accommodate customers who would not eat them.
Dietitians at other sites also expressed similar thoughts that if they had more menus to serve, they could ‘experiment’ with RSM more often to establish what is popular among their customers. If they have only one menu for all customers, it is safer to serve the most conventional menu items to prevent losing sales.
Economic environment
According to the dietitians, the most frequently reported barriers to serving RSM involved economic constraints. As was mentioned previously, one of the most significant roles for on-site dietitians is attracting many customers to the cafeteria and increasing sales. Dietitians also need to receive good reviews from customers to have their contracts renewed every two to three years. Therefore, in many cases, ‘experimenting with low sodium dishes is too risky’ (quote #8 in Table 3).
Because of this issue of profit margins, most of the cafeterias serve foods on a tight budget. This strategy affects investments in ingredients and staffing, which can be essential in reducing the sodium content of meals. For example, many cafeterias choose some packaged foods, such as frozen processed meats, sauces and dressings, because of their budget and personnel limitations. Serving foods that are freshly made on site with less salt, in many cases, tends to be more expensive and labour intensive.
Another example of economic difficulties involves investments in serving containers, such as soup bowls. In Korean food culture, a substantial amount of sodium is regularly consumed through soups. Experts have suggested that decreasing the size of soup bowls can help to reduce the amount of liquid (and, thus, sodium) consumption because of the decreased serving size. However, many dietitians that we interviewed said that it is difficult to buy new smaller soup bowls because of budget issues (quote #9 in Table 3).
Discussion
In the present qualitative research study, we examined the key barriers to and facilitators of serving RSM in worksite cafeterias as perceived by food-service personnel. To our knowledge, the present study is the first to examine the supply side, which should be taken into account when attempting to lower sodium intake among employees at worksite food-service establishments. Interviews with on-site dietitians and catering company managers revealed that there are many individual and environmental factors that enabled or hindered the provision of RSM.
To implement successful sodium-reduction interventions in worksite cafeterias, interviewees mentioned that changing customers’ and food-service personnel’s knowledge and perceptions is important. This statement aligns with previous intervention studies that showed customers’ food choices and nutrient intake can be improved by changing the food environment at worksite cafeterias and providing group education sessions( Reference Lowe, Tappe and Butryn 40 ). Another pilot intervention study revealed that working with food-service personnel to modify salt levels in worksite canteens was successful in changing employees’ salt intake( Reference Geaney, Harrington and Fitzgerald 23 ). From these findings, we learned that providing education and support to both customers and food-service personnel is crucial in improving employees’ diets in worksite cafeterias.
The results also showed that special attention should be given to different types of employee when improving customers’ knowledge, perceptions and intentions. As a number of interviewees mentioned, office workers are more likely to try RSM and tend to be more interested in healthy eating compared with manual workers. Therefore, when working with different types of employee, different consideration should be given to accommodating the target groups’ physiological needs and motivation levels. For example, interviewees mentioned that during summers in cafeterias that mostly serve customers working in hot environments, customers tend to eat more salty foods to compensate for sodium lost through sweating. In this situation, RSM may not be as appropriate. In other cases in which employees’ physiological need for sodium is not increased, the relatively lower levels of knowledge and motivation among manual workers should be addressed through targeted education.
In previous literature, we showed that current perceptions, intentions and behaviours regarding sodium intake varied by gender and age in the general population( Reference Park, Lee and Kwon 41 ). That previous study did not show differences between types of job, but it did show that sociodemographic factors are associated with sodium intake-related psychosocial factors. Therefore, future studies should examine the various psychosocial and behavioural factors in different target groups that are related to sodium intake patterns.
The present study explored various environmental barriers to serving RSM in worksite cafeterias, which has not been a main focus in previous studies in the literature. One review study that was published in 2005 summarized thirteen studies that had nutrition components in their worksite interventions( Reference Engbers, van Poppel and Chin A Paw 21 ). Most of the reviewed interventions focused on increasing fruit and vegetable availability and providing low-fat menus in canteens and vending machines. A relatively recent pilot intervention that was conducted in Ireland studied two public hospitals to assess the impact of a structured catering initiative on food choices( Reference Geaney, Harrington and Fitzgerald 23 ). However, in that study, the authors did not examine how to implement sustainable environmental changes for serving RSM.
One study reviewed various policy interventions that promoted healthy eating and concluded that changing school and work environments is more effective than improving knowledge or providing information( Reference Brambila-Macias, Shankar and Capacci 42 ). In working with food providers, it is necessary to know the barriers to and facilitators of developing effective programmes and policies. Various policy implications can be drawn from the present study. Because nearly all participants stressed the economic constraints involved in providing RSM, a variety of approaches to reducing this burden should be developed. One study conducted in Denmark found a positive relationship between corporate financial support and the availability of healthy meal options in worksite canteens( Reference Thorsen, Lassen and Andersen 43 ). Marking healthy food items is also an effective way of changing consumers’ perceptions of the healthfulness of foods served in worksite cafeterias( Reference Resnick, Gregoire and Lafferty 44 ). Lowering the economic barriers to serving RSM and marketing RSM with targeted messages to customers can involve a combination of successful strategies.
In addition to economic constraints, one of the most frequently mentioned barriers by the participants was the lack of skills and techniques related to preparing RSM (Themes 2 and 3). The areas in which the support is needed are as follows: (i) developing low-sodium menus that are acceptable to customers; (ii) strengthening cooking skills for low-sodium menus; and (iii) measuring and estimating the sodium content of foods.
Because taste is one of the foremost factors in food choice( Reference Furst, Connors and Bisogni 45 ), governments need to provide technical support for caterers in developing highly palatable RSM. In addition, workshops and training sessions for preparing RSM targeting food-service personnel can be a valuable investment, as many on-site food personnel stated they would like to learn more about cooking food with less salt (Theme 2). Finally, many interviewees mentioned they did not feel competent in measuring the sodium content of foods accurately in a busy kitchen, and they requested an easier way to monitor the sodium content of foods.
Empowering key stakeholders can be an important strategy for sustainable environmental interventions in healthy eating( 33 ). When a childhood obesity prevention programme was developed at schools, the researchers found that working with food-service personnel was important in modifying school nutrition environments( Reference Gittelsohn, Evans and Helitzer 46 , Reference Caballero, Davis and Davis 47 ). For sodium-reduction initiatives, it would be important not only to change food-service personnel’s perceptions but also to improve their skills to facilitate sustainability of the interventions.
Finally, as interviewees mentioned (Theme 1), if customers want RSM, they have no reason not to serve the foods. The simple economic rule of ‘supply and demand’ can play an important role in this matter. Catering companies are profit-driven institutions; if they make more profits by serving RSM, they may come up with solutions to lower the barriers. Therefore, various forms of education and promotion targeting customers should be implemented to make customers choose more RSM at cafeterias. Previous research on vegetable consumption in Japan( Reference Kushida and Murayama 48 ) and energy, sodium and fat consumption in Canada( Reference Vanderlee and Hammond 49 ) showed that customers’ food intake could be improved with proper educational messages at worksite cafeterias.
Recommendations for future policies and programmes
Based on these interviews on barriers to and facilitators of lowering the sodium content of meals served in worksite cafeterias, we summarize five future directions for successful sodium-related policies and programmes.
First, it is essential to provide technical support to food-service personnel for measuring and estimating the sodium content of foods. In addition, potentially easier methods of estimating sodium content, such as databases within acceptable measurement errors, should be established and tested. Another type of needed support is investment in expanding the variety of palatable RSM that can be easily prepared in large-scale worksite cafeterias within reasonable budgets.
Second, the government should try to improve knowledge, perceptions and intentions regarding eating less sodium in the daily diets of the general population. It would be difficult to change people’s preferences in taste and seasoning levels within a short period of time; however, continuing public campaigns and broadcasting advertisements through various media channels would be extremely helpful. In addition to educating the general public, educating food-service personnel is essential to lowering the sodium content of the foods served in worksite cafeterias.
Third, various types of monetary incentives or other types of compensation would lower the barriers to serving RSM. Because most worksite cafeterias require profits to exist, at this initial phase of the programme and policy formulation, providing smaller soup bowls, salimeters, and educational posters and pamphlets for food-service personnel and customers may incentivize sodium reduction. Providing tax benefits based on cafeterias’ performance could be another incentive to facilitate this process( Reference Brambila-Macias, Shankar and Capacci 42 ).
Fourth, working with food ingredient suppliers can address the deeper roots of the high sodium content in cafeteria foods. As was mentioned in the interviews (Theme 4, economic environment), many cafeterias depend on pre-packaged foods for quicker and more economical food preparation. Therefore, sodium-reducing strategies utilized by the food manufacturing companies that make sauces, dressings, noodles and frozen dishes can significantly lower the sodium content in cafeteria menus. In addition to food-service establishments’ ingredient suppliers, regular food entities (e.g. restaurants and other food manufacturers that sell packaged foods) should be encouraged to lower the sodium content of their products. This initiative will help to change the general population’s tastes over the long term.
Lastly, programmes and policies for lowering sodium content in commercial cafeterias should use different approaches from food safety regulations. Listening to the obstacles from catering companies and setting reasonable goals with people in the food business will be the key to success in lowering sodium content in food-service operations. The government should encourage caterers and food manufacturers to participate in policy-making processes and give them ownership and responsibilities as public health entities. Positive incentives for caterers and other companies to provide healthier options to their employees can be more effective than controlling them with strict rules and regulations.
Limitations of the study
The present study provided important information; however, there are some limitations to note. First, we attempted to conduct one-on-one interviews because there could have been sensitive issues that interviewees were not willing to share in front of their colleagues. Despite our efforts, for three interviews, we interviewed on-site dietitians and their supervisors (headquarters managers) together. We encouraged participants speak as though they were being interviewed by themselves by probing when we observed non-verbal signs during the interviews. However, we acknowledge that there could have been differences if they had been interviewed alone. Second, because of the lack of time and resources, we did not interview chefs or employees with other food-service positions. Future research can include data on employees with other positions in the industry or other customers to gather richer experiences from various perspectives. Finally, all of the participants were selected based on their previous experiences in serving RSM for the past year and the results should be interpreted with this purposeful sampling scheme in mind.
Conclusions
The present qualitative study revealed that there are many facilitators of and barriers to providing RSM at worksite cafeterias. Addressing multiple barriers at individual and environmental levels is essential when implementing successful worksite interventions to lower sodium intake among workers. Key barriers in providing RSM that the study found included limited skills and techniques required to serve RSM, a restricted number of tasty low-sodium menus and economic constraints due to tight budgets and pressure to maintain profit margins. Therefore, to expedite the effort to lower sodium intake among working populations, it is necessary to lower these barriers with multifaceted approaches from government, catering companies and customers. Other countries can learn from the present study when designing environmental interventions and developing policy. If we know how to work with catering sectors effectively, we can successfully the lower sodium content in meals served in worksite cafeterias and further apply this concept to restaurants and other food outlets.
Acknowledgements
Acknowledgements: The authors would like to acknowledge the study participants and Ms Jieun Chang for the support throughout the data collection. Financial support: This work was supported by the Korea Ministry of Food and Drug Safety. The Korea Ministry of Food and Drug Safety initially helped the research team to recruit the study participants but had no role in design, analysis or writing of this article. Conflict of interest: There are no conflicts of interest. Authorship: S.P. coordinated and conducted the research, analysed the data and drafted the manuscript; J.L. conducted the research, provided guidance in writing the manuscript and reviewed the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human participants were approved by the Institutional Review Board at Hanyang University. Written informed consent was obtained from all participants.





