



Introduction
Although there have been improvements in under-five child mortality rates over the last two and a half decades, these continue to be high in low- and middle-income countries (LMICs) (Lawn et al., Reference Lawn, Blencowe, Oza, You, Lee and Waiswa2014; United Nation, 2015a; Wang et al., Reference Wang, Bhutta, Coates, Coggeshall, Dandona and Diallo2016). Among 139 LMICs, only 24 nations met the Millennium Development Goals’ (MDG) target to reduce child mortality by two-thirds (United Nation, 2015a; Wang et al., Reference Wang, Bhutta, Coates, Coggeshall, Dandona and Diallo2016). The under-five mortality ratio is 1 in 147 in high-income countries, whereas in sub-Saharan Africa and Southern Asia, the ratio is 1 in 12 and 1 in 19, respectively. The current UN Sustainable Development Goal 3 (SDG-3) continues the global commitment, beyond the MDGs, to reduce under-five mortality to 25 deaths per 1000 live births by 2030 (United Nation, 2015b). According to the 2016 Global Burden of Disease (GBD) study, diarrhoea was the third leading cause of under-five child mortality in 2015 (GBD 2016 Cause of Death Collaborators, 2017) and continues to be the major cause of death among under-five children in low-income countries (WHO, 2017). In Africa and South Asia, over 80% of all under-five deaths were due to diarrhoeal diseases (UNICEF, 2012).
Benin had the fourth highest rate of childhood diarrhoea-related case fatalities in Africa in 2015 after Lesotho, Mali and Sierra Leone – accounting for an estimated 16 deaths per 10,000 children (Reiner et al., Reference Reiner, Graetz, Casey, Troeger, Garcia and Mosser2018). Diarrhoeal disease-related case fatality rates increased between 2000 and 2016 in Benin, from 15 deaths per 10,000 to 16 deaths per 10,000 children, respectively (Reiner et al., Reference Reiner, Graetz, Casey, Troeger, Garcia and Mosser2018). More recently, the 2018 CDC report published that diarrhoeal disease is fourth in the list of top ten causes of disease in Benin (CDC, 2018).
Efforts to address child mortality have focused on tackling immediate causes such as diarrhoea and pneumonia (Liu et al., Reference Liu, Oza, Hogan, Chu, Perin and Zhu2016). Several proximal and distal factors for childhood diarrhoeal disease (i.e. presence of latrine facility, waste disposal system, personal hygiene, income, maternal education) have been explored (Mihrete et al., Reference Mihrete, Alemie and Teferra2014; Teklemichael et al., Reference Teklemichael, Mohammed and Wondwosen2014; Dessalegn et al., Reference Dessalegn, Kumie and Tefera2014; Mossie et al., Reference Mossie, Tadesse and Kassa2014; Alambo et al., Reference Alambo2015; Liu et al., Reference Liu, Oza, Hogan, Chu, Perin and Zhu2016). However, the distal factors of gender equality and women’s empowerment that fuel the immediate causes have received little attention (Marmot, Reference Marmot2005). Evidence shows that women’s empowerment is a function of both demographic and socioeconomic factors in a society (Ndaimani et al., Reference Ndaimani, Mhlanga and Dube-Mawerewere2018). Empowerment of women is the process of enabling them to have the power to navigate life’s challenges in all areas of their lives (Mahmud et al., Reference Mahmud, Shah and Becker2012). It is the process of enabling women with less influence or power to make informed choices in all matters that affect their health and well-being and that of their children (Doku et al., Reference Doku, Bhutta and Neupane2020).
Gender equality and women’s empowerment are key components of the development agenda worldwide (United Nation, 2015b). Efforts towards achieving MDG-3, which sought to promote gender equality and women’s empowerment, have led to some significant gains over the last two decades (United Nation, 2015a). The UN’s SDG-5 continues the call to achieve gender equality and empower all women and girls by 2030 (UN Women, 2021). Among the indicators of women’s empowerment, women’s decision-making power and attitude towards wife-beating are two key components (Kishor & Subaiya, Reference Kishor and Subaiya2008; Jennings et al., Reference Jennings, Cherewick, Hindin, Mullany and Ahmed2014; Hanmer & Klugman, Reference Hanmer and Klugman2016).
Conceptual framework
For a clearer understanding of the possible mechanisms and factors associated with how women’s empowerment could affect child health, a heuristic model was created to organize key findings to date (Figure 1). Women’s empowerment enhances the likelihood of maternal health services utilization such as antenatal care, health facility delivery and postnatal care services (Furuta & Salway, Reference Furuta and Salway2006; Nguyen et al., Reference Nguyen, Hoang and Nguyen2014; Wado, Reference Wado2018). Women’s health autonomy (i.e. making decisions about own health care and not needing permission to seek medical help) and health care service utilization are positively associated with childhood services such as immunization and the treatment of fever and acute respiratory infections (Ariyo & Jiang, Reference Ariyo and Jiang2020). Additionally, women’s empowerment has been shown to have a positive influence on water, sanitation and hygiene related interventions (Dery et al., Reference Dery, Bisung, Dickin and Dyer2019).

Figure 1. Theoretical framework for the association between women’s empowerment and childhood diarrhoea.
Throughout the world, women are predominantly responsible for taking care of children in a household (Treas & Drobnič, Reference Treas and Drobnič2010). To fulfil this responsibility, women need adequate resources within the home and a degree of control over the use of these (Alemayehu et al., Reference Alemayehu, Theall, Lemma, Hajito and Tushune2015). In other words, women with decision-making power (i.e. on use of household income) may also have influence over the quantity and quality of food purchased and consumed by her children (IFPRI, 2014; Abate & Belachew, Reference Abate and Belachew2017; Mekonnen et al., Reference Mekonnen, Odo, Nigatu, Sav and Abagero2021).
As for women’s wife-beating attitude, women who disagree with or refuse to justify wife-beating tend to have a stronger role in decision-making (Ebrahim & Atteraya, Reference Ebrahim and Atteraya2018). They are more likely to participate in decisions regarding income allocated to purchase items for themselves and their children, particularly on food and feeding practices, which affect children’s health. Furthermore, they are not forced to provide foods that are only available in the home, which can be less expensive but less nutritious (Mekonnen et al., Reference Mekonnen, Odo, Nigatu, Sav and Abagero2021). Studies have shown that the mothers who have decision-making authority, and access to and sufficient control over economic resources, have a positive impact on their children’s health (Richards et al., Reference Richards, Theobald, George, Kim, Rudert, Jehan and Tolhurst2013; Budu et al., Reference Budu, Seidu, Armah-Ansah, Sambah, Baatiema and Ahinkorah2020). A systematic review by Pratley (Reference Pratley2016) showed that women’s empowerment had a positive association with the uptake of childhood immunization and good child feeding practices in developing countries. Furthermore, studies from sub-Saharan Africa have demonstrated that the children of mothers with inadequate decision-making capability on health care are more likely to suffer from malnutrition and related childhood morbidity and mortality (Fantahun et al., Reference Fantahun, Berhane, Wall, Byass and Högberg2007; Alemayehu & Meskele Reference Alemayehu and Meskele2017). Recent work has found that women’s socio-demographic factors –age, place of residence, ethnicity, religion, region, educational level, employment status, economic status and media exposure – influence both childhood diarrhoea (Woldeamanuel, Reference Woldeamanuel2020) and women’s empowerment (MOWCY et al., 2019).
The few studies that have looked at women’s empowerment and child health have focused on child nutrition (Cunningham et al., Reference Cunningham, Ruel, Ferguson and Uauy2015; Yimer & Tadesse, Reference Yimer and Tadesse2015; Jones et al., Reference Jones, Haardörfer, Ramakrishnan, Yount, Miedema and Girard2019; Kuche et al., Reference Kuche, Moss, Eshetu, Ayana, Salasibew, Dangour and Allen2019; Abreha et al., Reference Abreha, Walelign and Zereyesus2020). There is little evidence on the role of women’s empowerment on childhood mortality, and in particular, the correlation between women’s empowerment and childhood diarrhoea is largely unknown. As a result, this study examined the role of women’s empowerment in the reduction of childhood diarrhoea prevalence in Benin using 2017/18 Benin Demographic and Health Survey data. It was hypothesized that women who make decisions on household, health and visiting family, as well as those who do not agree with any of the reasons to justify wife-beating, are less likely to have a child under five years of age who had diarrhoea in the weeks before the survey.
Methods
The health system in Benin
Located in West Africa, Benin has been one of the most politically stable countries in Africa following its democratic election in 1991 (Jhpiego, 2012; USAID, 2016). It had a population of close to 11.5 million in 2018 (World Bank, 2019). The UNDP 2019 Human Development Index report ranks Benin 163 out of 189 countries (UNDP, 2019), with two-fifths (40%) of the population estimated to be living in poverty and within-country disparities and inequities resulting in non-inclusive economic growth (African Development Bank Group, 2020).
Historically, the focus of Benin’s health system has been on the public sector, with stringent governing processes and centralized decision-making (SHOPS Project, 2013). The country’s twelve departments are divided into 34 health zones, each containing 1–4 communes managed by health zone committees and management teams (USAID, 2016). Each zone has department health centres, community health centres and a hospital. A health zone office oversees all public and private health entities within a given zone, including private and public hospitals, clinics and pharmacies. The existence of a private health sector in Benin is a relatively new development that is quickly growing as a result of several factors, including accelerated urbanization and poor access to, and quality of, public services. Human resources for health are a major health system problem in Benin, particularly in regard to quantity, quality and distribution, and this adversely affects health service quality throughout the country (USAID, 2016).
Data sources
Data for analysis were extracted from the 2017/18 Benin Demographic and Health Survey (BDHS). This is the fifth in a series of DHS carried out in the country since 1996, except the 2018 Multiple Indicator Cluster Survey (MICS). The BDHS is a nationally representative survey with the aim of collecting data on many topics, including antenatal care, skilled delivery service, postnatal care, child immunizations services, maternal death, child death, nutritional status of women and their children, and HIV/AIDS. The survey was carried out with the technical assistance of Inner-City Fund (ICF) International provisioned through the USAID-funded MEASURE DHS Program. A two-stage stratified cluster sampling technique was applied. Large geographic settings (enumeration areas) were selected in the first stage through probability proportional to size (PPS). Then, fixed numbers of households were selected from each EA in the second stage using systematic sampling technique. Details of the methodology can be found in the 2017/18 BDHS final report (INSAE & ICF, 2019). The individual recode file (KR) was used for analysis. This study included data for 7979 currently married women aged 15–49.
Dependent variable
The outcome variable was ‘childhood diarrhoea’. The passage of three or more loose or watery stools per day is considered diarrhoea (or more frequent passage than is normal for the individual) (WHO, 2017). In the DHS, women with under-five children are asked: ‘has [child name] had diarrhoea in the last 2 weeks?' (INSAE & ICF, 2019, p. 521). Hence, analysis for this study included children under age five who were reported to have had diarrhoea in the 2-week period preceding the survey (WHO & UNICEF, 2013; Rutstein et al., Reference Rutstein, Staveteig, Winter and Yourkavitch2016). Childhood diarrhoea was a binary variable, with children under five who had diarrhoea in the 2 weeks preceding the survey coded ‘1’ and those who did not coded ‘0’.
Independent (women’s empowerment) variables
Women’s empowerment is a key component for strategies promoting health and combating poverty in development work. No widely accepted measurement indicator exists because of the continued debate over the meaning of women’s empowerment and multiple underlying theoretical perspectives (i.e. feminist, political philosophy, psychology, community development) (Gram et al., Reference Gram, Morrison and Skordis2019). Following Gram et al.’s (Reference Gram, Morrison and Skordis2019) pragmatic approach, it was determined that the best measures of women’s empowerment that make ‘the most sense for [our] own context’ (p. 1368) were decision-making and wife-beating attitude. The former is an objective measure and the latter a subjective measure. These are the two main indicators of women’s empowerment used in research (Kishor & Subaiya, Reference Kishor and Subaiya2008). In order to assess empowerment, a decision-making gradient was used (moderately empowered or highly empowered) while attitude towards wife-beating provided a subjective measure to consider the cultural context.
A woman’s decision-making power was assessed from whether they make specific decisions, either alone or jointly with their husband, on: 1) their own health care; 2) large household purchases and; 3) visits to family or relatives. If a woman did not make decision on any of the three decision-making parameters, either alone or with her husband, i.e. if all decisions were made by her husband or another member of the family, she was considered to have no decision-making power (i.e. not empowered). If a woman decided, either alone or jointly with her husband, on two of the three decision-making parameters, she was considered to have some decision-making power and coded ‘1’ (moderately empowered). Finally, if a woman made decisions, either alone or together with her husband, on all three decision-making parameters, she was considered to have high decision-making power and coded ‘2’ (highly empowered).
A woman’s attitude to wife-beating was assessed from whether they disagreed with specific reasons for justifying wife-beating, i.e. burning food, arguing with husband, going out without telling husband, neglecting the children and refusing to have sexual intercourse with husband. If a woman disagreed with/did not justify all five wife-beating parameters, she was coded as ‘disagrees/does not justify’ wife-beating. If a women agreed it was justified or acceptable to beat a wife for any of the five stated reasons as a normal healthy part of life, she was coded as ‘accepts/justifies’ wife-beating (Kishor & Subaiya, Reference Kishor and Subaiya2008).
Control variables
Several individual- and community-level factors, based on previously available literature (Kishor & Subaiya, Reference Kishor and Subaiya2008; Mahmud et al., Reference Mahmud, Shah and Becker2012; Dessalegn et al., Reference Dessalegn, Kumie and Tefera2014; Mihrete et al., Reference Mihrete, Alemie and Teferra2014; Teklemichael et al., Reference Teklemichael, Mohammed and Wondwosen2014; Alambo et al., Reference Alambo2015; Oyediran, Reference Oyediran2016; Gurmu & Endale, Reference Gurmu and Endale2017; Doku et al., Reference Doku, Bhutta and Neupane2020; Astutik et al., Reference Astutik, Efendi, Sebayang, Hadisuyatmana, Has and Kuswanto2020), were considered as confounder variables and controlled for their influence on the outcome and independent variables (see Figure 1). The socio-demographic factors included maternal age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49); woman’s education (no formal education, primary school, secondary school, higher); husband’s education (no formal education, primary school, secondary school, higher); woman’s employment for cash (no, yes); religion (Vodoun, Islam, Catholic, Protestant Methodist, Other Protestant, Celestes, Other Christian, No Religion, Other); region (Alibori, Atacora, Atlantic, Borgou, Collines, Couffo, Donga, Littoral, Mono, Oueme, Plateau, Zou); place of residence (urban, rural); ethnicity (Adja and related, Bariba and related, Dendi and related, Fon and related, Yoa-Lokpa and related, Betamaribe and related, Peulh and related, Yoruba and related, Other Beninois, Other); and husband’s occupation (not working, professional/technical/managerial, sales, agricultural self-employed, agricultural employee, services, skilled manual, other). The DHS wealth index was used to categorize respondents into poorest, poorer, middle, richer, richest wealth quintiles.
Statistical analysis
STATA version-14 software was used for data analysis. Editing and imputation of missing data were conducted by the DHS Programme before data were released for use (Rutstein & Rojas, Reference Rutstein and Rojas2006; Croft et al., Reference Croft, Aileen, Marshall and Allen2018). The DHSs in LMICs are prone to being incomplete as well as having partial or inconsistent reporting of responses for different questions because of the complexity of the questionnaires. The purpose of data editing and imputation in the DHS is to accurately reflect the population studied and makes it useable for analysis (Rutstein & Rojas, Reference Rutstein and Rojas2006; Croft et al., Reference Croft, Aileen, Marshall and Allen2018). Missing values on who usually make specific decisions were assumed to be someone other than the respondent and excluded from the numerators (Kishor & Subaiya, Reference Kishor and Subaiya2008; Rutstein & Rojas, Reference Rutstein and Rojas2006; Croft et al., Reference Croft, Aileen, Marshall and Allen2018).
Descriptive statistics provided measures of frequencies and dispersion to provide a socio-demographic profile of the sample population using the exploratory variables. Inferential statistics were completed through non-parametric bivariate analysis using Pearson’s chi-squared test between each of the independent variables and prevalence of childhood diarrhoea. This resulted in the unadjusted effect of the explanatory variables on the prevalence of childhood diarrhoea. A multicollinearity test was carried out using the variance inflation factor (VIF) to check for collinearity between explanatory variables; the results revealed no evidence of multicollinearity (VIF Mean = 1.20, VIF Max = 1.66, VIF Min = 1.02). Multivariable Logistic Regression (MLR) was used to determine the effect of women’s decision-making power and wife beating attitude on the reduction in childhood diarrhoea, controlling for confounding variables and resulting in Adjusted Odds Ratios (aOR), using a 95% Confidence Intervals (CI) and testing for significance.
To account for the complex sampling design used to collect DHS data, the svyset and subpop STATA commands were used to weight the sample and reflect the population of married women (i.e. sampling clusters, strata and sub-population were appropriately considered).
Results
Background characteristics of respondents
Table 1 presents the socioeconomic characteristics of married Beninese women by prevalence of childhood diarrhoea. Of the 7979 currently married women included in the study, about 5.5% and 17.6% were in the age groups 15–19 and 20–24 years, respectively. More than three-fifths (60.3%) were rural residents, and nearly 66.3% of the women and 54.1% of their husbands had no formal education. About 27.3% had no decision-making power, either alone or together with their husbands, on any of the three decision-making parameters (own health, large purchases and visiting relatives), whereas 36.4% and 36.3% had decision-making power on two and three of the parameters, respectively. About 65.4% of the women disagreed with all five wife-beating justifications, and the rest (34.6%) justified or accepted at least one of the reasons. About 13.6% of the under-five children of currently married women had diarrhoea.
Table 1. Socioeconomic characteristics of married Beninese women by prevalence of childhood diarrhoea, 2017/18 Benin DHS, N = 7979

a Weighted.
b All main categories include related ethnicities.
Prevalence of childhood diarrhoea by explanatory variables
The prevalence of diarrhoea in under-five children varied by explanatory variables (Table 1). For instance, about 13.7% of the under-five children of mothers with no formal education had diarrhoea, and the percentage decreased to 4.3% for those of mothers who attained higher education. Notably, a 19.3 percentage point difference in the prevalence of childhood diarrhoea was evident among children residing in the Atacora (25.9%) and Zou (6.6%) regions. Bivariate analysis showed all the variables included in the model were significantly associated with under-five childhood diarrhoea in Benin: woman’s age and education, husband education and occupation, household wealth index, religion, ethnicity and urbanity/rurality, as well as the women’s empowerment variables of decision-making and justification of wife-beating.
Women’s empowerment as a predictor of childhood diarrhoea
Decision-making was found to be significantly associated with childhood diarrhoea (Table 2). The odds of childhood diarrhoea among children whose mother had decision-making power on all three decision-making parameters were lower (i.e. 26% less chance) compared with children whose mother had no decision-making power on any of the parameters (aOR = 0.74, 95% CI: 0.57–0.96). Furthermore, women’s age (20–24 years: aOR = 1.94, 95% CI: 1.20–3.15; 25–29 years: aOR = 2.06, 95% CI: 1.25–3.40, 30–34 years: aOR = 1.78, 95% CI: 1.07–2.97), women’s educational level (primary school: aOR = 1.36, 95% CI: 1.06–1.73), wealth index (richest: aOR = 0.67, 95% CI: 0.45–0.99) and region (Borgou: aOR = 0.42, 95% CI: 0.28–0.63; Zou: aOR = 0.40, 95% CI: 0.19–0.82) were all associated with childhood diarrhoea.
Table 2. Multivariable logistic regression analysis of association between women’s decision-making power and prevalence of childhood diarrhoea, 2017/18 Benin DHS
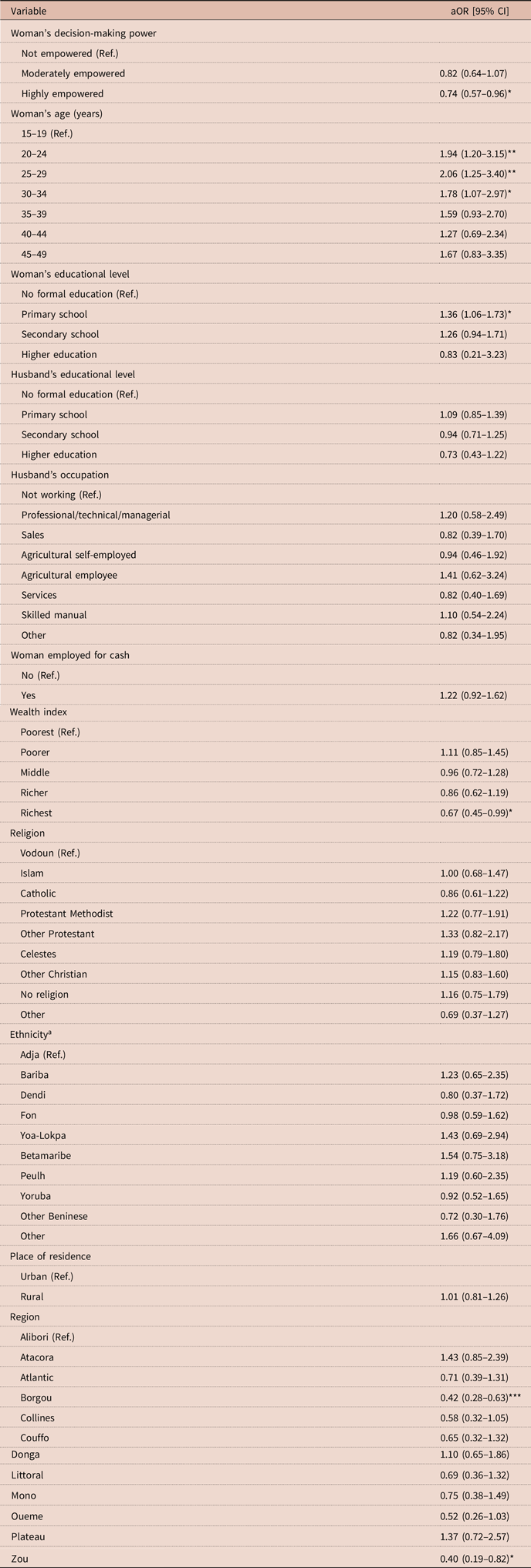
a All main categories related ethnicities.
Ref. = reference category.
*p < 0.05; **p < 0.01; ***p < 0.001.
Another main finding from the current study was the significant association between the wife-beating attitude of the women and the prevalence of childhood diarrhoea. More specifically, under-five children whose mothers did not agree with, or justify, wife-beating for any of the five parameters (burning food, arguing with husband, going out without telling husband, neglecting the children, refusing to have sexual intercourse with husband) had a 21% lower chance of diarrhoea compared with those whose mothers thought that at least one of the wife-beating parameters was justified or acceptable (aOR = 0.79, 95% CI: 0.65–0.96) (Table 3).
Table 3. Multivariable logistic regression analysis of association between women’s wife-beating attitude and prevalence of childhood diarrhoea, 2017/18 Benin DHS

a All main categories include related ethnicities.
Ref. = reference category.
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
In low- and middle-income countries like Benin, childhood mortality remains high (Lawn et al., Reference Lawn, Blencowe, Oza, You, Lee and Waiswa2014; Wang et al., Reference Wang, Bhutta, Coates, Coggeshall, Dandona and Diallo2016). Confronting the immediate causes of mortality alone is not enough, and addressing other indirect socio-demographic factors such as women’s empowerment is vital to reduce childhood mortality (Marmot, Reference Marmot2005). To the best of the authors’ knowledge, this is the first study in the African context to assess the role of women’s empowerment on reducing childhood diarrhoea using a large population-based sample.
As hypothesized, the study confirmed that women’s decision-making power can reduce the prevalence of childhood diarrhoea. Consistent with a recent study in Indonesia (Astutik et al., Reference Astutik, Efendi, Sebayang, Hadisuyatmana, Has and Kuswanto2020), there was a significant difference in childhood diarrhoea reduction between women who had decision-making power compared with their counterparts who did not. Usually, women are the principal caregivers for children, the sick and families overall (Dimbuene et al., Reference Dimbuene, Amo-Adjei, Amugsi, Mumah, Izugbara and Beguy2018). If women were not empowered to make decisions, this can lead to adverse health outcomes for children, woman themselves and other family members (Godha et al., Reference Godha, Hotchkiss and Gage2013; Dimbuene et al., Reference Dimbuene, Amo-Adjei, Amugsi, Mumah, Izugbara and Beguy2018). Women’s empowerment is highly linked with child health outcomes (Pratley, Reference Pratley2016).
An empowered woman is more likely to protect her child and herself by adopting good health behaviours through prevention measures such as hygiene and sanitation, and access to, and utilization of, health care services, immunization, vaccination and good nutrition (Kabeer, Reference Kabeer2012). Studies in Myanmar (Mie et al., Reference Mie, Hnin and Khaing2019) and Bangladesh (Mainuddin et al., Reference Mainuddin, Bagum, Rawal, Islam and Islam2015) have demonstrated a higher likelihood of accessing health care services (including child health services) among empowered women compared with non-empowered women. Moreover, studies conducted in several developing countries, i.e. Ethiopia (MOWCY et al., 2019), Nigeria and India (Ibrahim et al., Reference Ibrahim, Tripathi and Kumar2015), have shown that empowered women who actively participate in decision-making in the household are more likely to have a positive influence on child health outcomes.
This study found that women’s attitude to wife-beating was associated with childhood diarrhoea. Previous studies have shown low health care service uptake among women who accept wife-beating as a healthy part of life in Bangladesh (Yount et al., Reference Yount, Halim, Schuler and Head2013; Khan & Islam, Reference Khan and Islam2018). It is possible that these women have less awareness of their rights (Khan & Islam, Reference Khan and Islam2018). A woman who disagrees with or does not justify wife-beating, may have higher self-esteem and stand up for herself and what she believes in, to the benefit of her children (Caruso et al., Reference Caruso, Stephenson and Leon2010). She will often have control over financial resources, and have the confidence and intention to invest in her children’s health, i.e. by correct feeding and hygiene practices and other related activities that lead to a decreased likelihood of childhood diarrhoea (Caruso et al., Reference Caruso, Stephenson and Leon2010).
Intimate partner violence (IPV) could be intergenerational (Hines & Saudino Reference Hines and Saudino2002; Martin et al., Reference Martin, Moracco, Garro, Tsui, Kupper and Chase2002; Vung et al., Reference Vung, Ostergren and Krantz2008). Female children who witness their mothers in defeated and violent situations are more likely to accept wife-beating in their adult life (Vung et al., Reference Vung, Ostergren and Krantz2008). In a community where wife-beating is socially customary, IPV is more prevalent. However, IPV is less likely among women who are empowered, either socially, economically or educationally (Jewkes, Reference Jewkes2002).
Previous findings on the factors affecting the association between maternal age and the odds of childhood diarrhoea are inconclusive and seem to be context-specific. Studies in Tanzania (Edwin & Azage, Reference Edwin and Azage2019), Kenya (Samwel et al., Reference Samwel, Eddison, Faith, Richard, Elizabeth and Dougals2014), sub-Saharan Africa (Adedokun & Yaya, Reference Adedokun and Yaya2020) and elsewhere (Vasconcelos et al., Reference Vasconcelos, Rissin, Figueiroa, Lira and Batista Filho2018) have shown that the children of older women have lower odds of childhood diarrhoea than those of adolescents or younger women. This could be because of their experience from having other children or their knowledge acquired from neighbours, relatives or health professional (Vasconcelos et al., Reference Vasconcelos, Rissin, Figueiroa, Lira and Batista Filho2018; Edwin & Azage, Reference Edwin and Azage2019). The present study showed an association between women’s age and the likelihood of childhood diarrhoea, with higher odds among the children of adult women (20–34 years) compared with those of younger women (15–19 years). Also, having more children may mean reduced attention and care and availability of proper, nutritional food with an increased number of siblings sharing resources and maternal support (Sonneveldt et al., Reference Sonneveldt, Plosky and Stover2013).
Findings regarding the association between mother’s age and use of child health services are mixed. The utilization of some maternal and child health services (i.e. institutional delivery) among younger women has been shown to be higher than among older women in India (Mondal et al., Reference Mondal, Karmakar and Banerjee2020). The decrease in utilization of health services by experienced or older mothers may be due to previous experience of non-compassionate health facility services or belief that they have sufficient knowledge from their previous pregnancies, deliveries or related conditions and do not think they need the services (Zegeye et al., Reference Zegeye, El-Khatib, Ameyaw, Seidu, Ahinkorah and Keetile2021). It may also be linked to the burden of management of large families, which leads to resource shortage and lesser likelihood of using health services (Sonneveldt et al., Reference Sonneveldt, Plosky and Stover2013; Zegeye et al., Reference Zegeye, El-Khatib, Ameyaw, Seidu, Ahinkorah and Keetile2021). Reynolds et al. (Reference Reynolds, Wong and Tucker2006) explored adolescent women’s use of maternal and child health services in 15 developing countries; in general, they found no variation in maternal child health care use by mother’s age. However, findings from India, Indonesia and Peru showed that adolescents 16 years or younger were less likely than their slightly older counterparts (17–24) to use health care services (Reynolds et al., Reference Reynolds, Wong and Tucker2006). Women’s status and power, relative to their male partner, tend to be lower with young/adolescent mothers in developing countries, and may play a role in their health care seeking behaviour (Reynolds et al., Reference Reynolds, Wong and Tucker2006; Smith et al., Reference Smith, Ramakrishnan, Ndiaye, Haddad and Martorell2003).
Consistent with a prior study in Tanzania (Edwin & Azage, Reference Edwin and Azage2019), this study found higher odds of childhood diarrhoea among married women who attended primary education compared with those who had no formal education. However, this finding contradicts prior studies in Nigeria (Desmennu et al., Reference Desmennu, Oluwasanu, John-Akinila, Opeyemi and Ayo2017) and Ethiopia (Woldu et al., Reference Woldu, Bitew and Gizaw2016). Variations in the prevalence of childhood diarrhoea among women with no formal education and those who attended primary education may be due to differences in other unknown risk factors for diarrhoea and need further exploration.
This study found lower odds of childhood diarrhoea among women in the wealthiest households compared with the poorest. Prior studies in Ethiopia reported similar findings (Gebru et al., Reference Gebru, Taha and Kassahun2014; Gedefaw et al., Reference Gedefaw, Takele, Aychiluhem and Tarekegn2015; Woldu et al., Reference Woldu, Bitew and Gizaw2016). Wealthy households can afford the necessities of hygiene and sanitation, including soap and hand sanitizer (Woldu et al., Reference Woldu, Bitew and Gizaw2016). Furthermore, there was an association between region and childhood diarrhoea, and comparable findings have been reported in Tanzania (Edwin & Azage, Reference Edwin and Azage2019), Ethiopia (Bogale et al., Reference Bogale, Gelaye, Degefie and Gelaw2017; Atnafu et al., Reference Atnafu, Sisay, Demissie and Tessema2020) and SSA (Yourkavitch et al., Reference Yourkavitch, Burgert-Brucker, Assaf and Delgado2018). This regional variation could be explained by the differences in factors affecting childhood diarrhoea such as improved latrine utilization coverage, access to and utilization of safe drinking water (Mengistie et al., Reference Mengistie, Berhane and Worku2013; Clasen et al., Reference Clasen, Alexander, Sinclair, Boisson, Peletz and Chang2015; Atnafu et al., Reference Atnafu, Sisay, Demissie and Tessema2020), weather conditions, socioeconomic status and access to, and utilization of, hygiene and sanitation facilities (Edwin & Azage, Reference Edwin and Azage2019). Since factors affecting childhood diarrhoea are multidimensional, exploring region-specific factors and designing region-specific intervention may be required to address this issue in highly vulnerable populations (Atnafu et al., Reference Atnafu, Sisay, Demissie and Tessema2020).
The study provides valuable evidence on the associations between women’s empowerment and child health, considering the demographic and socioeconomic factors that interact with women’s access to, and utilization of, health resources that can impact child health in Benin. It used recent, nationally representative population-based data that are comparable across countries. However, it had its limitations. First, as women’s empowerment has no standardized measure, two indicators recommended by the DHS guidelines had to be used (Kishor & Subaiya, Reference Kishor and Subaiya2008). Second, as cross-sectional data were used, causal inference could not be made. Finally, some bias might have occurred due to self-reporting by the women during the interview process.
The government of Benin needs to prioritize women’s empowerment by educating women through the adult education programmes, and economically empowering them through women-centred micro-finance schemes. Moreover, legal protection, as well as democratic and human rights awareness, must be considered to reduce accepted attitudes towards wife-beating to empower Beninese women. Together, these interventions will help reduce childhood diarrhoea and other childhood negative health outcomes in Benin.
Acknowledgments
The authors thank the MEASURE DHS project for their support, and free access to their original data. More details regarding DHS data and ethical standards are available at: http://goo.gl/ny8T6X. Data for this study were sourced from the Demographic and Health surveys (DHS) and are available here: http://dhsprogram.com/data/available-datasets.cfm.
Funding
This research received no specific grant from any funding agency, commercial entity or not-for-profit organization.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Ethics Approval
This study used publicly available data from DHS. Informed consent was obtained from participants prior to the survey. The DHS Program follows ethical standards for ensuring the protection of respondents’ privacy. ICF International ensures that the survey complies with the US Department of Health and Human Services regulations for the respect of the right of human subjects. No further approval was required for this study since the data were secondary and available in the public domain.
Author Contributions
SY contributed to the study design and conceptualization. SY, BZ and DIW reviewed the literature, performed the analysis and critically reviewed the manuscript for its intellectual content. SY had final responsibility to submit for publication. All authors read and amended drafts of the paper and approved the final version.




