


Studies of children suffering profound institutional privation in infancy and early childhood have shown that it results in major developmental impairment, that there is considerable developmental catch-up following adoption into well-functioning families, and that there are clinically significant sequelae in some of the children (Reference Chisholm, Carter and AmesChisholm et al, 1995; Reference AmesAmes, 1997; Reference Fisher, Ames and ChisholmFisher et al, 1997; Reference ChisholmChisholm, 1998; Rutter et al, 1998, 2001; Reference O'Connor, Rutter and BeckettO'Connor et al, 2000). However, the studies also show that, at least in relation to specific outcomes, there is considerable heterogeneity in response. Thus, in our own study, for children who experienced at least 2 years of institutional privation in infancy, the measured IQ scores at 6 years ranged from the severely retarded range to high superior (Reference O'Connor, Rutter and BeckettO'Connor et al, 2000). Because the published reports all consider outcomes in relation to specific impairments, it is not known whether the children who fare well on one type of outcome also fare well on others. It is necessary to determine the extent to which impairments tend to be pervasive across domains and to ask what proportion of profoundly deprived children achieves generally normal psychological functioning. Equally, it is not known whether profound institutional privation results in a general increase in all forms of psychopathology or whether there are certain behavioural patterns or syndromes that are particularly strongly associated with early privation. The aim of this investigation was to use findings from a follow-up study (to age 6 years) of institution-reared Romanian children who were adopted into UK families to answer these questions on specificity and heterogeneity in children's responses to profound institutional privation.
METHOD
Subjects
The sample comprised 165 children adopted from Romania before the age of 42 months, selected at random from within bands stratified according to age of entry to the UK, and a comparison group of 52 non-deprived within-UK adoptees placed before the age of 6 months (for details see Rutter et al, 1998). Of these, 156 children from Romania and 50 within-UK adoptees had complete data-sets and wee used for analyses where these were required. Four-fifths of the Romanian adoptees had been reared in institutions for most of their life and nearly all had been admitted to institutions in the neonatal period (mean age of admission was 0.34 months). The conditions in the Romanian institutions were generally extremely bad (see Reference Kaler and FreemanKaler & Freeman, 1994; Reference Castle, Groothues and BredenkampCastleet al, 1999; Reference Johnson and NelsonJohnson, 2001); and the condition of most of the children on arrival in the UK was also very poor. Their mean weight was 2.4 standard deviations below the mean (with over half below the third percentile) and the (retrospectively administered) Denver scale produced a mean quotient of 63, with three-fifths functioning in the severely retarded range. By the time the children reached the age of 4 years substantial catch-up had occurred, with the mean weight and Denver quotient both being near normal for UK children (Rutter et al, 1998). Eighty-one per cent of the adoptive parents of Romanian children who were approached to participate in the study agreed to do so.
Measures
The assessments at age 6 years comprised a standardised investigator-based interview that included (among other things) systematic questions on attachment disorder behaviours (O'Connor et al, Reference O'Connor, Bredenkamp and Rutter1999, 2001), completion of parent and teacher versions of the Rutter behavioural scales (Reference Elander and RutterElander & Rutter, 1996; Reference Hogg, Rutter, Richman and SclareHogg et al, 1997) and individually administered McCarthy Scales of Children's Abilities (Reference McCarthyMcCarthy, 1972). In order to assess possible autistic features, the parents completed the Autism Screening Questionnaire (ASQ; Reference Berument, Rutter and LordBerument et al, 1999). In addition, the Autism Diagnostic Interview — Revised (ADI—R; Reference Le Couteur, Rutter and LordLe Couteuret al, 1989; Reference Lord, Rutter and Le CouteurLordet al, 1994) was given by a researcher experienced in its use (M. L. R.) when parental interview reports suggested the possibility of autistic features (see Reference Rutter, Andersen-Wood and BeckettRutter et al, 1999).
In order to obtain a categorical measure of probable dysfunction in each of seven specific domains of functioning, the data were dealt with as follows.
Attachment problems
Three items from the parental interview — definite lack of differentiation between adults; clear indication that the child would readily go off with a stranger; and definite lack of checking back with the parent in anxiety-provoking situations — were scored as 0 for ‘no abnormality’, 1 for ‘probable problem’ and 2 for ‘definite problem’. These were summated to produce a composite score ranging from 0 to 6, and a cut-off of 4 or more was used to indicate dysfunction.
Inattention/overactivity
The Rutter scales completed by mothers and fathers were standardised and then averaged to produce a single parent score (see Reference Kreppner, O'Connor and RutterKreppner et al, 2001). The teachers' scale was similarly standardised. The inattention/overactivity items on the parents' scale were: very restless, has difficulty staying seated for long; squirmy, fidgety child; cannot settle to anything for more than a few moments and inattentive; and easily distracted. The teachers' scale included all the preceding items plus: excessive demands for teacher's attention; and fails to finish things started — short attention span. Using the distribution of scores in the within-UK adoptees sample, three categories were created for the parents' and teachers' scales separately with a score of 0 for a score below the median, 1 for a score between the median and the top 10% cut-off, and 2 for a score in the top 10% of the range. Pervasive inattention/overactivity required a score of 2 on either the parents' or teachers' scale and a score of 1 or 2 on the other scale. Children with a missing score on one scale were not included in the ‘pervasive’ category.
Emotional difficulties
The scores on the Rutter parents' and teachers' scales were standardised in the same way as for hyperactivity. The emotional difficulties items were: has had tears on arrival at school or has refused to go into the building in the past 12 months; gives up easily; often worried, worries about many things; often appears miserable, unhappy, tearful or distressed; cries easily; tends to be fearful or afraid of new things or new situations; stares into space and often complains of aches and pains (see Reference Hogg, Rutter, Richman and SclareHogg et al, 1997). These were dealt with according to the distribution of scores in the within-UK adoptees sample. Children with scores in the top 5% on either or both of the parents' and teachers' scales were treated as having emotional difficulties.
Autistic features
Using the ASQ and the ADI—R, 20 children were diagnosed as showing quasi-autistic features (Reference Rutter, Andersen-Wood and BeckettRutter et al, 1999). As this provided the combination of total screening coverage of both groups and individual diagnoses, this categorisation was used.
Cognitive impairment
The general cognitive index (GCI) of the McCarthy Scales was used as the measure. Children who scored at least 2 standard deviations below the UK sample's mean were treated as showing cognitive impairment. The UK sample mean was 117, with a standard deviation of 18. Twice the standard deviation (36) subtracted from 117 equated to a score of 81; accordingly all children with an IQ of 81 or less were included in this domain of dysfunction.
Peer difficulties
Peer difficulties were assessed through a combination of the Rutter parents' and teachers' scales, together with nine items from the parental interview. The three items in the parents' scale were ‘not much liked by other children’, ‘tends to be solitary’ and ‘does not get on well with other children’. The mother and father scales were combined into a parental composite, using the approach described for inattention/overactivity. The three items in the teachers' scale were ‘not much liked by other children’, ‘tends to be on own’ and ‘cannot work in a small peer group’. The nine parental interview items were: group play; differentiation between children (i.e. clear preferences, with one or more special friends); popularity; age preference of peers; harmony of peer interaction; teased by other children; teases others; picked on/bullied; and picks on/bullies others. Peer group difficulties were regarded as present if the score on any of the three measures was in the top (most deviant) 5% of the distribution for the UK sample.
Conduct problems
The scores on the Rutter parents' and teachers' scales were standardised as for hyperactivity and emotional difficulties. The conduct items were: often destroys own or others' property; frequently fights or is extremely quarrelsome with other children; is often disobedient; often tells lies; has stolen things on one or more occasions in the past 12 months; disturbs other children; bullies other children; blames others for things; is inconsiderate of others; kicks, bites other children (see Reference Hogg, Rutter, Richman and SclareHogg et al, 1997). Children who scored in the top 5% of scores in the UK sample distribution on either scale were categorised as showing conduct problems.
Statistical analysis
Between-group differences in the proportion of children showing dysfunction on each of the seven domains were examined using Fisher's two-tailed exact test and one degree of freedom. Within-group differences according to age of entry to the UK were examined for a linear trend on a chi square comparing entry at under 6 months, 6-24 months, and over 24 months (n=58, 59 and 48 respectively). Polychoric correlations were used to examine the association among the binary domains of dysfunction variables.
Cluster analysis was used to examine the ways in which children in the Romanian adoptees sample showed similarities in their patterns of dysfunction. The technique is valuable for grouping individuals according to shared patterns of psychopathology. The seven dichotomous variables were cluster analysed using Ward's method of agglomeration based on squared Euclidean distance (Reference Aldenderfer and BlashfieldAldenderfer & Blashfield, 1988). A four-cluster solution was chosen based on coefficient of linkage, practical considerations (such as sample size) and interpretability. The cluster analyses were then rerun using alternative indices of similarity in order to determine the consistency of the cluster profiles. All approaches gave patterns closely similar to those displayed in Fig. 1. As an additional check, cluster analyses were repeated using continuously distributed dimensions, rather than binary categories, again with similar findings (further details available from the authors upon request).
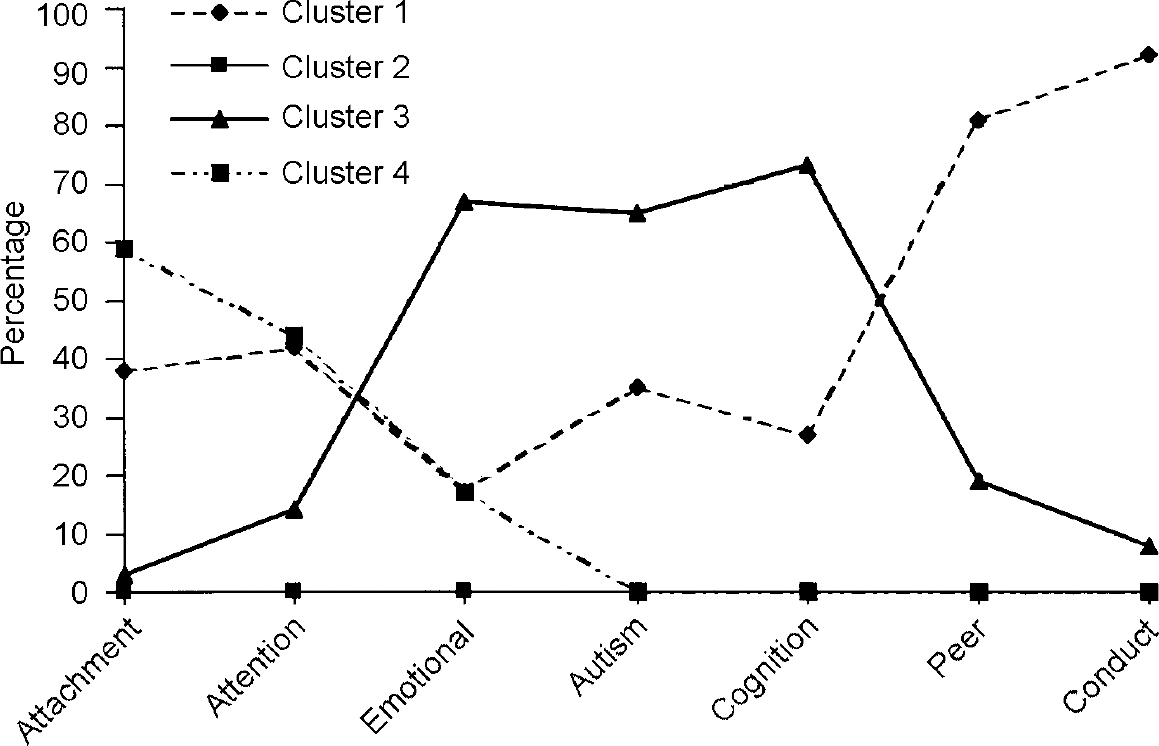
Fig. 1 Percentage extreme score across seven outcomes according to cluster membership.
RESULTS
Of the seven domains of dysfunction when the children were aged 6 years, three (emotional problems, peer difficulties and conduct problems) showed no difference in rate between the adoptees from Romania and the within-UK adoptees (Table 1). For each of these three domains, there was no association, within the Romanian adoptees sample, with the children's age at the time of entry to the UK. In sharp contrast, the other four domains (attachment problems, inattention/overactivity, quasi-autistic problems and cognitive impairment) were all much more common in the Romanian sample and, in each case, there was a significant association with age at entry, the rate of problems being much higher in those who left Romania when they were older. The implication is that the former three domains are not particularly associated with institutional privation, whereas the latter four seem to be.
Table 1 Seven domains of dysfunction at 6 years of age in Romanian and within-UK adopted children
| Domains | Rate in Romanian adoptees | Rate in within-UK adoptees | Between-group differences | Association with age at entry to UK | |||
|---|---|---|---|---|---|---|---|
| % | n | % | n | Fisher's exact P(two-tailed) | χ 2 trends | P | |
| Attachment problems | 20.7 | 164 | 3.8 | 52 | 0.003 | 11.13 | 0.001 |
| Inattention/overactivity | 25.3 | 162 | 9.6 | 52 | 0.019 | 9.04 | 0.003 |
| Emotional difficulties | 3.7 | 162 | 9.6 | 52 | NS | 0.03 | NS |
| Quasi-autistic features | 12.1 | 165 | 0.0 | 52 | 0.005 | 4.61 | 0.032 |
| Cognitive impairment | 14.0 | 157 | 2.0 | 50 | 0.018 | 14.61 | 0.001 |
| Peer difficulties | 18.9 | 164 | 9.6 | 52 | NS | 0.45 | NS |
| Conduct problems | 8.0 | 162 | 9.6 | 52 | NS | 0.97 | NS |
Table 2 summarises the findings on the number of domains showing dysfunction in the two groups, together with the association with age at entry within the Romanian sample. As would be expected in any general population sample, a substantial minority of the UK adoptees showed dysfunction in at least one domain. Less than four-fifths were free of dysfunction on any domain. Nevertheless, dysfunction was substantially more likely to be present in the Romanian adoptees, and the proportion without dysfunction on at least one domain was significantly lower in those who came to the UK when they were older. Of those leaving Romania after their second birthday, between a fifth and a quarter were free of any measurable dysfunction at 6 years of age. The trend for more dysfunction, and more pervasive dysfunction, in Romanian adoptees and for an association with age at entry was apparent at all levels of frequency of dysfunction. The main difference between the groups, however, was evident in the presence or absence of any dysfunction, rather than in the pervasiveness of dysfunction across domains.
Table 2 Romanian and within-UK adopted children: percentages of children with impairment in 0, 1, 2 or 3 or more domains
| Number of domains in which there is impairment | Within-UK adoptees (n=50) | Romanian adoptees, age at entry into UK | χ 2 trends | P | ||
|---|---|---|---|---|---|---|
| < 6 months (n=56) | 6-24 months (n=35) | 24-42 months (n=45) | ||||
| 0 (n=112) (%) | 78.0 | 69.6 | 43.6 | 23.9 | 34.81 | 0.001 |
| 1 (n=46) (%) | 12.0 | 17.9 | 23.6 | 37.0 | 19.79 | 0.002 |
| 2 (n=20) (%) | 2.0 | 7.1 | 12.7 | 17.4 | 9.75 | 0.002 |
| 3 or more (n=28) (%) | 8.0 | 5.4 | 20.0 | 21.7 | 6.73 | 0.009 |
What characterised the Romanian adoptees sample were the particular domains involved in the pervasive dysfunction pattern. Almost always, this involved some admixture of attachment problems, inattention/overactivity and quasi-autistic problems. In contrast, in the UK sample pervasive impairment usually involved either conduct or emotional disturbance plus another problem, but not one of the patterns that was distinctive of the institutional privation children.
Of the 40 children in the Romanian adoptees group who showed impairment on just one domain, 13 did so on attachment problems, 11 on inattention/overactivity, 7 on peer difficulties and 6 on cognitive impairment (with only an additional 3 on other domains). Of the 6 children in the within-UK adoptees group with impairment on just one domain, 2 showed it on emotional difficulties, 2 on inattention/overactivity, 1 on conduct problems and 1 on attachment problems.
Table 3 presents the polychoric correlations among domains of dysfunction within the Romanian adoptees sample. The intercorrelations are no more than moderate in most instances but there was a stronger correlation (0.66) between autistic features and cognitive impairment and between autistic features and peer difficulties (0.59). Cognitive impairment showed a near-zero correlation with emotional difficulties and with conduct problems. Attachment problems had their strongest correlation with inattention/overactivity (0.47). There were only 6 children in the Romanian sample with emotional difficulties but 5 of these showed a quasi-autistic pattern, giving rise to a high polychoric correlation.
Table 3 Polychoric correlation among domains of dysfunction in Romanian adoptee sample
| Attachment problems | Inattention/ overactivity | Emotional difficulties | Autistic features | Cognitive impairment | Peer difficulties | |
|---|---|---|---|---|---|---|
| Attachment problems | ||||||
| Inattention/overactivity | 0.47 | |||||
| Emotional difficulties | 0.16 | 0.29 | ||||
| Autistic features | 0.25 | 0.24 | 0.81 | |||
| Cognitive impairment | 0.20 | 0.26 | 0.05 | 0.66 | ||
| Peer difficulties | 0.30 | 0.48 | 0.39 | 0.59 | 0.47 | |
| Conduct problems | 0.38 | 0.49 | 0.46 | 0.36 | 0.03 | 0.68 |
Figure 1 shows the cluster analysis for Romanian adoptees. The largest cluster (n=74) was cluster 2, in which there was no dysfunction on any of the seven domains (Table 4). Cluster 1 was the one with the greatest pervasiveness of dysfunction, with about half of the children (or more) showing difficulties in attachment, inattention/overactivity, peer relationships and conduct. A few also showed quasi-autistic features or cognitive impairment. Cluster 3 is largely defined by the presence of both quasi-autistic features and cognitive impairment. Cluster 4 comprised children who showed only attachment problems and inattention/overactivity (apart from one child who also showed an emotional difficulty). The mean age at entry was 10.3 months for cluster 2, 18.4 months for cluster 1, 22.3 months for cluster 3 and 20.0 months for cluster 4. The only significant contrast was that between cluster 2 and the other three clusters. The effect of age at entry was similarly shown in the trend across the three age-at-entry groups. Thus, the proportion in the late-placed group (over 2 years) was 15% in cluster 2, compared with 38% in cluster 1, with 52% in cluster 3 and with 39% in cluster 4.
Table 4 Associations between clusters and domains impaired
| Cluster | Domains | Mean no. of domains impaired per child | ||||||
|---|---|---|---|---|---|---|---|---|
| Attachment problems | Inattention/ overactivity | Emotional difficulties | Autistic features | Cognitive impairment | Peer difficulties | Conduct problems | ||
| 2 (n=74) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.0 |
| 1 (n=29) | 13 | 17 | 1 | 7 | 6 | 25 | 12 | 2.79 |
| 3 (n=23) | 1 | 6 | 4 | 13 | 16 | 6 | 1 | 2.04 |
| 4 (n=31) | 20 | 18 | 1 | 0 | 0 | 0 | 0 | 1.25 |
There were no gender differences among the seven domains or among the four clusters.
DISCUSSION
Escape from dysfunction
In order to determine whether children who experience prolonged early institutional privation could nevertheless show normal psychological function at age 6 years, several years after leaving the depriving environment and after being adopted into generally well-functioning adoptive homes, we assessed dysfunction across seven different domains that were relevant at that age, occurred with a reasonable frequency and could be assessed with reasonable reliability. Normal functioning was defined according to the stringent criterion of no abnormality on any of the seven domains. As would be expected, over a fifth of the children in the non-deprived within-UK adoptee sample failed to show normal functioning on this very strict criterion.
Two findings stand out with respect to the Romanian sample. First, the proportion with normal functioning among those who left Romania before the age of 6 months was nearly as high (70%) as in the within-UK adopted sample. Second, even among the children who were over the age of 2 years when they left Romania, between a fifth and a quarter showed normal functioning on all seven domains. It is sometimes supposed that lasting damage is inevitable after prolonged early institutional privation, but our results run counter to that view. The chances of normal social functioning were substantially less the older the child was at the time of leaving the institution, but some of the children who had the most long-lasting privation appeared to be functioning entirely normally by the age of 6 years. Of course, it would be wrong to suppose that there are no scars and it is possible that there may be sequelae that become evident only at a later age. Nevertheless, the degree of resilience shown was remarkable. Because our sample extended only up to an age of entry of 42 months, we can draw no conclusions on whether or not there is an age at which recovery becomes extremely unlikely. Extrapolation from the linear trends found on all analyses suggests that the chance of normal functioning diminishes progressively the older the child at the time when profound privation comes to an end, but it is not known whether — or when — that chance eventually ceases to exist.
The findings on pervasiveness of dysfunction make the additional point that, of the children showing some form of impairment, nearly half showed impairment on only one domain, and only just over a quarter showed impairment on at least three domains. Even within the group of children who were over the age of 2 years when they arrived in the UK, only just over a fifth showed pervasive dysfunction of that extent.
Specificity of sequelae of institutional privation
Across a large number of studies, the relative non-specificity of the patterns of psychopathology associated with psychosocial stresses and adversity has been the general finding (Reference RutterRutter, 2001). Thus, negative life events carrying long-term threat have been associated with a wide range of psychiatric disorders (Reference Brown and HarrisBrown & Harris, 1989; Reference GoodyerGoodyer, 1990), and the same applies to the experience of physical and sexual abuse (Reference Kendall-Tackett, Meyer Williams and FinkelhorKendall-Tackett et al, 1993; Reference Trickett and McBridge-ChangTrickett & McBridge-Chang, 1995). Accordingly, it might have been expected that prolonged institutional privation would be associated with a general increase in all forms of psychopathology. However, that is not what we found. Strikingly, there was no increase in either emotional or conduct problems, and although the rate of peer difficulties was twice as high in the Romanian adoptees, the difference between groups fell short of statistical significance. The finding that none of these three domains of dysfunction showed any association with the children's age at entry to the UK also indicates that it is unlikely that these particular areas of problem at 6 years of age were consequences of the children's early institutional experiences. The children are too young for any firm conclusions with respect to late sequelae but, at least up to the age of 6 years, these do not seem to be a particular consequence of the depriving institutional upbringing. Accordingly, if such problems occur in young institution-reared children, they may arise for reasons that have little to do with their early adverse upbringing. However, this might change in later childhood and adolescence, when the situations with respect to both emotional disturbance and peer relationships are different.
Although there was no single pattern that characterised children who experienced institutional privation, three main features stood out, occurring both on their own and in varying combinations. First, there were attachment disturbances of various kinds (O'Connor et al, Reference O'Connor, Bredenkamp and Rutter1999, 2001). These were particularly characterised by a relatively undiscriminating social approach, a seeming lack of awareness of social boundaries and a difficulty in picking up social cues on what is socially appropriate or acceptable to other people. This is a pattern also identified in a parallel Canadian study of adoptees from Romania (Reference Chisholm, Carter and AmesChisholm et al, 1995; Reference ChisholmChisholm, 1998). Second, there was the pattern of inattention/overactivity. Of the 41 children in the Romanian sample who showed this behaviour, nearly half (16) showed it in association with attachment problems, but 11 children showed only inattention/overactivity and 8 showed it in association with quasi-autistic behaviour (in 4 of the 8 cases also with attachment problems). Attention-deficit and hyperkinetic disorders have usually been thought of as psychiatric conditions that are strongly influenced by genetic factors, with psychosocial influences playing only a subsidiary role in aetiology (Taylor, Reference Taylor, Rutter, Taylor and Hersov1994, Reference Taylor1999). It is striking, therefore, that this has emerged as one of the patterns most strongly associated with prolonged institutional privation. It could be, of course, that the key causal influence derived from nutritional privation rather than psychological privation in the institutions. On the other hand, more detailed analyses suggest that nutritional privation was not the key risk factor (further details available from the authors upon request). The finding that inattention/overactivity is also common in children reared in group homes within the UK, where nutritional privation is not an issue, suggests that it may well be the psychological features of the institutional environment that are more important (Reference Roy, Rutter and PicklesRoy et al, 2000). It remains to be determined whether the clinical picture of inattention/overactivity in these children is the same as in more ‘ordinary’ varieties of attention-deficit or hyperkinetic disorders, and a follow-up study that is now in progress should throw light on this point. Meanwhile, the evidence suggests that the problems may lie more in dealing with social group situations than with overactivity as such.
The third pattern particularly associated with a background of institutional privation was that of quasi-autistic features. Again, this appears surprising at first sight because of the evidence that autism as diagnosed in children from more ordinary backgrounds involves a strong genetic influence, with little evidence of psychosocial features playing a part in the causal process (Reference RutterRutter, 2000). The clinical picture in the sample of Romanian adoptees was, however, somewhat different from that characteristic of ‘ordinary’ autism with respect to the tendency to improve between the ages of 4 and 6 years and the extent of social approach (Reference Rutter, Andersen-Wood and BeckettRutter et al, 1999).
Institutional privation was quite strongly associated with cognitive impairment (Rutter et al, 1998, Reference Rutter, O'Connor, Beckett and Selman2000; Reference O'Connor, Rutter and BeckettO'Connor et al, 2000). In 6 of the 22 children showing cognitive impairment, this occurred without dysfunction on any of the other domains. It was, however, much more common for it to be accompanied by either quasi-autistic patterns (present in 10 out of the 20 children and in some cases with dysfunction in other domains as well) or with attachment disturbances (7 children). At the age of 6 years, there was nothing particularly distinctive about the patterns of impairment but distinctive features may be more evident at age 11 years, when the children are to be seen again. With the Romanian adoptee sample, it is also noteworthy that inattention/overactivity was more strongly associated with attachment problems (17/41 cases) than with cognitive impairment (7/41). Moreover, of these 7 children characterised by inattention/overactivity and cognitive impairment, 5 also showed attachment disturbance.
In summary, profound institutional privation was particularly associated with patterns involving attachment disturbance, inattention/overactivity, quasi-autistic features and cognitive impairment in varying combinations, but it was not associated with any marked general increase in other forms of psychopathology. There is a need for more detailed study of these psychopathological patterns; in the meantime, clinicians need to be alert to their occurrence and to the possibility that these patterns derive from early institutional privation. It is important, too, that effective methods of intervention should be developed for these privation-related problems (Reference Rutter, O'Connor, Beckett and SelmanRutter et al, 2000).
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
• Profound early institutional privation tends to be particularly associated with attachment disorder behaviours, inattention/overactivity (especially when associated with attachment disturbances) and quasi-autistic behaviour.
-
• Such privation is not followed by a significant increase in conduct problems, emotional disturbance or peer relationship difficulties other than in the context of institutional privation patterns (see first implication), at least by age 6 years.
-
• Profound institutional privation from infancy to age 3 years is still compatible with normal psychological functioning provided that the child has experienced several years in a good adoptive family.
LIMITATIONS
-
• So far, the children have been followed only up to the age of 6 years.
-
• Only some of the children have received detailed individual clinical assessments.
-
• Because the children could not be studied while in the Romanian institutions, it was not possible to determine which aspect of privation was most influential.






eLetters
No eLetters have been published for this article.