Patients’ attitudes and subjective experience are crucial in the management of severe mental illness, but their practical value is overlooked.
To identify predictors of future adherence to LAI antipsychotic maintenance treatment of schizophrenia among socio-demographic, clinical, and psychometric characteristics – including Drug Attitude Inventory-10 (DAI-10) and Subjective Well-being under Neuroleptics short form (SWN-K) scores.
Retrospective baseline data from 53 clinically stable outpatients with schizophrenia switched from oral to LAI therapy were collected. Patients continuing treatment at the time of analysis (n=29) were compared to those who had discontinued it (n=24). Selected variables were further evaluated in survival analyses.
Between-group differences are presented in Table 1 (**: p<0.01; *: p<0.05).Continued treatment Discontinued treatment χ2 or t Treatment persistence (months) 63.79±21.01 23.88±25.80 6.21** Age (years) 39.17±10.11 35.58±13.39 1.11 Male 15 (51.7%) 13 (54.1%) 0.03 Single 20 (69.0%) 15 (62.5%) 0.25 Instruction (years) 13.28±3.31 11.83±3.56 1.53 Employed 20 (69.0%) 7 (29.2%) 8.32** Illness duration (years) 17.69±10.53 13.42±11.36 1.42 Previous hospitalisations 2.10±1.32 2.67±1.86 -1.29 MADRS 13.59±9.06 14.67±8.99 -0.43 YMRS 5.52±5.57 6.00±9.94 -0.22 p-PANSS 12.17±5.20 14.38±6.13 -1.41 n-PANSS 10.90±5.39 15.63±7.93 -2.48* g-PANSS 29.38±10.33 33.63±10.26 -1.49 PANSS 52.66±17.57 63.96±20.61 -2.15* DAI-10 3.86±4.96 -1.13±5.80 3.38** SWN-K 74.93±23.07 81.00±15.60 -1.09
Cox regression analysis included instruction, employment, hospitalisations, PANSS subscales and DAI-10 scores: a protective role against treatment discontinuation was outlined only for employment (HR 0.16; 95%CI 0.05-0.50) and higher DAI-10 scores (HR 0.85; 95%CI 0.78-0.94). DAI-10 scores delineated distinct adherence trajectories (Figure 1).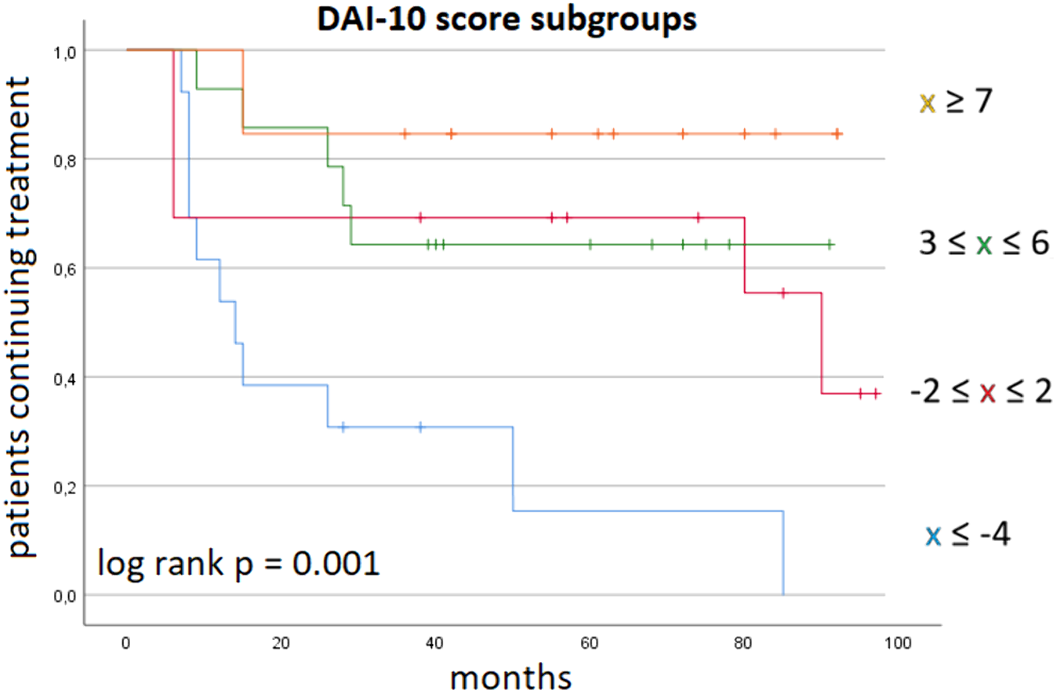
Baseline DAI-10 scores may identify patients at risk of dropout after switching to LAI.
No significant relationships.

