



Post-traumatic growth
Post-traumatic growth (PTG) refers to the phenomenon of beneficial psychological change as a result of experiencing a traumatic event.Reference Tedeschi and Calhoun1 The most used measure of PTG, the Post-Traumatic Growth Inventory (PTGI), defines PTG within the domains of being able to relate to others better, spiritual change, a new understanding of your own personal strength, perceiving new possibilities in your life or having a better appreciation of your life.Reference Tedeschi and Calhoun2 Along with the beneficial psychological changes involved with PTG, the construct has also been associated with other positive outcomes such as better mental health and positive health behaviours, such as lower alcohol and cigarette use.Reference Siegel and Schrimshaw3,Reference Barskova and Oesterreich4
PTG and the armed forces
With an increased focus on building a more resilient, psychologically prepared military forceReference Tedeschi and McNally5,Reference Angel6 and the UK armed forces responsibilities during the COVID-19 pandemic,7 it may be helpful to understand PTG in the UK military context and identify factors that might be associated with this beneficial psychological change. A systematic review on the topic suggested that military personnel experienced moderate PTG following deployment to Iraq/Afghanistan;Reference Mark, Stevelink, Choi and Fear8 however, this was based almost entirely on samples from the USA. Among serving and ex-serving personnel in the USA, better mental health and physical healthReference Tsai, Sippel, Mota, Southwick and Pietrzak9 were associated with greater PTG, whereas greater anger problemsReference Hijazi, Keith and O'Brien10 were associated with lower levels of PTG. Greater combat exposure,Reference Mitchell, Gallaway, Millikan and Bell11 being a reservist,Reference Maguen, Vogt, King, King and Litz12 perceived threat during deployment,Reference Maguen, Vogt, King, King and Litz12 being of junior rankReference Mitchell, Gallaway, Millikan and Bell11 and a greater length of time since deploymentReference Hawker and Nino13 were associated with greater PTG. PTG and post-traumatic stress disorder (PTSD) have a more complicated relationship, with increasing PTSD symptoms being shown to have a curvilinear relationship with PTG (e.g. a bell-shaped curve, with PTG symptoms increasing along with PTSD symptoms up to a point, upon which as PTSD symptoms continue to increase, PTG symptoms decrease).Reference Shakespeare-Finch and Lurie-Beck14 There are numerous differences in the way that the UK and USA deploy troops and manage their personnel, including variations in deployment length, greater number of reservists/national guard deployed and differences in regimental systems. There are also noted differences in mental health and behavioural outcomes between UK and US armed forces following deployment.Reference Sundin, Herrell, Hoge, Fear, Adler and Greenberg15 It may therefore be problematic to extrapolate USA findings to the UK context regarding PTG.
Aims
The only UK data on PTG in military personnel focuses on PTG as a result of seeking treatment for PTSD.Reference Murphy, Palmer, Lock and Busuttil16 Given the paucity of UK military research into PTG, we aim to (a) examine deployment-related PTG among serving and ex-serving personnel in the UK military who deployed to Iraq or Afghanistan; and (b) explore relationships between selected sociodemographic, health and deployment-related variables and PTG.
Method
Study design and participants
Data were drawn from the third phase of a representative longitudinal survey investigating the health and well-being of a cohort of Iraq or Afghanistan deployed and non-deployed UK military personnel since the UK deployed to Iraq in 2003.Reference Stevelink, Jones, Hull, Pernet, MacCrimmon and Goodwin17 At baseline, 10 272 participants took part (response rate 61.0%). At phase 3, 8093 participants took part (response rate 44.3%). Eligibility for the current study required participants to have deployed to either Iraq, Afghanistan or both. Only data collected at phase 3 is reported in this paper.
Participants were asked to complete a questionnaire relating to sociodemographic, service information, deployment experiences, transitioning from deployment to home experiences, mental and physical health, relationships and lifestyle-related variables, either via paper survey or online. Data collection took place between 2014 and 2016. Access to a participant information sheet as well as specification that research was being conducted independently of the Ministry of Defence, and that participation was entirely confidential and voluntary was included in the questionnaire.
Materials
PTG
The PGTI is a validated 21-item measure of PTG.Reference Tedeschi and Calhoun2 A military deployment version of the PTGI (DPTGI) was administered (Supplementary File 1 available at https://doi.org/10.1192/bjo.2022.570). The stem question to the questionnaire was changed to ‘As a result of my deployment(s) to Iraq/Afghanistan since 2002 … ’. Because of concerns about readability for a UK armed forces audience, especially among those with low educational attainment, the language of some questions was altered minimally and responses were reduced from a six-point to a four-point Likert scale: ‘no change for the better’, ‘a small change for the better’, ‘a medium change for the better’ and ‘a big change for the better’. The sum of all PTG items was used to generate a total PTG score (score range 0–63).
Sociodemographic and military factors
Data on age, service, rank, relationship status and engagement status (regular or reservist) were gathered from the questionnaire and supplemented by Defence Statistics, the Ministry of Defence's data and statistics branch.
Health factors
PTSD
To measure PTSD, the 17-item Post-Traumatic Checklist – Civilian VersionReference Blanchard, Jones-Alexander, Buckley and Forneris18 was used. A score of ≥50 was used to define probable PTSD (score range 17–85).
Common mental disorders
To measure common mental disorders (CMD), the 12-item General Health Questionnaire was used.Reference Hardy, Shapiro, Haynes and Rick19 A score of ≥4 was used to define a probable CMD (score range 0–12).
Anger
To measure anger, the Dimensions of Anger Responses (DAR-5) questionnaire was used.Reference Forbes, Hawthorne, Elliott, McHugh, Biddle and Creamer20 A score of ≥12 was used to define a probable anger problem (score range 4–25).
General health
A single question from the 36-item Short Form Survey was used as a measure of self-reported general health: ‘In general, how do you rate your health now?’. Responses were given on a five-point Likert scale from poor to excellent. General health was recoded into three categories: ‘excellent/very good’, ‘good’ and ‘fair/poor’.Reference Jenkinson, Coulter and Wright21
Smoking
Two questions were asked in the survey regarding ‘Do you currently smoke?’ and ‘If yes, how many cigarettes, cigars or rollups do you smoke a day?’. Total number of cigarettes smoked per day was used as a reflection of smoking behaviours.
Alcohol consumption
Alcohol use was measured with the ten-item World Health Organization's Alcohol Use Disorders Identification Test (AUDIT).Reference Babor, Higgins-Biddle, Saunders and Monteiro22 To measure alcohol consumption, the sum of scores from the first three questions of the AUDIT (AUDIT-C) were used. Higher scores reflect greater alcohol consumption (score range 0–12).
Childhood adversity
Childhood adversity was measured through use of a 16-item questionnaire used previously in UK military health research.Reference Iversen, Fear, Simonoff, Hull, Horn and Greenberg23 A score of ≥4 indicated greater childhood adversity (score range 0–16).
Recent life events
To measure stressful life events, a post-deployment stressor measure was adaptedReference Smid, Kleber, Rademaker, van Zuiden and Vermetten24 into an 11-item checklist with responses ‘yes’ or ‘no’, indicating whether the participant experienced a significant life event (e.g. divorce, death of a loved one) during the past 3 years.
Deployment-related factors
Combat exposure
Combat exposure was assessed with a 14-item measure adapted from the Combat Experiences Scale,Reference Hoge, Castro, Messer, McGurk, Cotting and Koffman25 which asked about exposure to potentially traumatic combat events such as exposure to an improvised explosive device or coming under small arms fire. Responses were given as either 0 (no reported experience) or 1 (experienced once or more on deployment) (score range 0–14). If the participant deployed to both Iraq and Afghanistan, the combat experience was counted if they experienced it on either deployment.
Belief of being in serious danger and length of time in hostile areas
Belief that ‘you were in serious danger of being injured or killed’ and ‘length of time in hostile areas during deployment’ were derived from the Deployment Risk and Resilience Inventory.Reference King, King, Vogt, Knight and Samper26 Belief of being in serious danger had answers ranging from ‘never’, ‘once or twice’, ‘sometimes’ to ‘many times’. Length of time participants were in hostile areas during their deployment had answers ranging from ‘not at all’, ‘up to 1 week’, ‘1 week to 1 month’ to ‘more than a month’.
Both questions were asked for Iraq as well as Afghanistan deployments. The maximum score on either deployment was used to generate a ‘belief of being in serious danger’ and ‘length of time in hostile area’ variable. Belief of being in serious danger was recoded into three categories: 1 (never), 2 (once or twice/sometimes) and 3 (many times). Length of time in hostile area was recoded into three categories: 1 (not at all), 2 (up to 1 week/1 week to 1 month) and 3 (more than a month).
Role on last deployment
Role was grouped based on types of role-in-theatre reported, ‘combat’ (e.g. infantry), ‘combat support’ (e.g. Royal Engineers) and ‘combat service support’ (e.g. medics).
Data analysis
Sample and response weights based on gender, age, rank, service, engagement type, serving status, sample and the interaction between sample and engagement type were used to generate response weights, and sample weights were calculated as the inverse likelihood of a participant being sampled from a specific subgroup (e.g. deployment era).Reference Stevelink, Jones, Hull, Pernet, MacCrimmon and Goodwin17 The sample weights and response weights were multiplied together to make a single weight, and applied using the ‘svy’ function in Stata (version 16.1 for Windows). Weighted percentages and relative risk ratios (RRRs) are presented along with unweighted cell counts.
PTG tertiles based on total DPTGI score were used: no/a very low degree of PTG (0–7), a low degree of PTG (8–20) and a moderate/large degree of PTG (21–63). The statistical software package Stata was used for all statistical analyses. All sociodemographic (age, gender, service, rank), health (overall general health, anger, childhood adversity, common mental disorders, PTSD, alcohol use, smoking) and deployment-related (deployment, reservist status, ex-serving status, years since trauma, combat role, combat experiences, belief of being in serious in serious danger, length of time in hostile areas) variables investigated as part of this analysis have previously been shown to be associated with PTG (9–14).
For the purposes of this paper, PTSD scores were splined based on a clinically meaningful threshold of ≥50, indicating probable PTSD, because of the known curvilinear relationship between PTSD and PTG.Reference Shakespeare-Finch and Lurie-Beck14 Two variables, one representing PTSD symptoms in the non-caseness group (<50) and one representing PTSD symptoms in the caseness group (≥50), were created. Visual inspection of plots of all variables investigated as part of this paper with PTG were conducted. Variables that appeared to have a curvilinear relationship with PTG were squared and entered into a univariable multinomial logistic regression model, and those with a significant association with PTG (P < 0.05) were defined as having a curvilinear relationship. Adverse childhood events and anger scores on the DAR-5 were found to have a curvilinear relationship with PTG, and subsequently, both were splined in a similar fashion to PTSD. Adverse childhood events were splined around four or more events,Reference Iversen, Fear, Simonoff, Hull, Horn and Greenberg23 and anger was splined around caseness (DAR-5 score ≥12). Because of the known correlations between anger and PTSD,Reference Olatunji, Ciesielski and Tolin27 anger was only investigated at a univariable level.
Multinomial logistic regression was used to assess the sociodemographic, military, health and deployment-related factors associated with PTG. Univariable analysis was conducted on all variables of interest. As gender is a known predictor of PTG,Reference Vishnevsky, Cann, Calhoun, Tedeschi and Demakis28 analysis was completed on the whole sample, then male personneland female personnelseparately. Variable selection procedures for the multivariable multinomial logistic regression model were based on recommendations in the literature.Reference Heinze, Wallisch and Dunkler29 The procedures were as follows: (a) all variables with a strong evidence base in the literature were selected for inclusion (this included age,Reference Janoff-Bulman30 PTSD symptomsReference Shakespeare-Finch and Lurie-Beck14 and CMDReference Barskova and Oesterreich4), (b) all variables with univariable RRRs >1.25 or <0.80 were selected for inclusion of model 1 and (c) all remaining variables were subject to best subset variable selection with the ‘gvselect’ Stata function. Variables in the model selected with the lowest Bayesian information criterion were selected for inclusion in model 1 (Supplementary File 2). Model stability analysis was conducted on model 1 by using bootstrap analysis (‘mfpboot’ function in Stata); 1000 replications were used. Bootstrap inclusion frequencies were generated, and variables that had scores >0.50 and P < 05 were included in the final model (model 2) (Supplementary File 3). Because of the small number of female personnel who scored over the clinical cut-off point on the PTSD Checklist, only PTSD symptoms in the non-probable PTSD group were included in the final model. Multicollinearity was assessed through variance inflation factors.
Ethical approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Ethical approval for the Health and Well-Being StudyReference Stevelink, Jones, Hull, Pernet, MacCrimmon and Goodwin17 was granted by the UK Ministry of Defence Research Ethics Committee (reference: 448/MODREC/13) and the King's College London Psychiatry Nursing and Midwifery Research Ethics Subcommittee (reference: PNM/12/13–169). Participants provided informed consent to take part in the study by completing and returning the questionnaire.
Results
Of the 8093 participants who took part in phase three of the cohort study, 5239 had deployed to Iraq and/or Afghanistan (64.7% of the total sample). This included participants from all branches of the armed forces (Royal Navy (including Royal Marines), army and Royal Air Force), as well as regulars and reservists. After excluding those with two or more missing answers on the DPTGI, 5180 out of 5239 (98.9%) participants were included for analysis. Cronbach's alpha for the 21-item DPTGI was excellent (α = 0.95), which indicates excellent internal validity.
Sample characteristics
The mean age of the sample was 40 years (standard deviation 9.35), 89.0% (n = 4610) were male and 11.0% (n = 570) were female. Further, 30.6% (n = 1460) of participants held combat roles, 13.0% (n = 643) held combat support roles and 56.4% (n = 3072) held combat service support roles. Regarding deployment, 35.7% (n = 1773) of participants were deployed to Iraq only, 29.6% (n = 1604) were deployed to Afghanistan only and 34.7% (n = 1803) were deployed to both Iraq and Afghanistan. Table 1 describes the sociodemographic and deployment characteristics of those included in the study overall and by PTG tertile (no/a very low degree of PTG, a low degree of PTG and a moderate/large degree PTG).
Table 1 Description of study participants (sociodemographic factors) overall and by post-traumatic growth tertiles (N = 5180)

Numbers may not add up to 5180 because of missing data. Weighted percentages are presenting alongside unweighted cell counts. PTG, post-traumatic growth; DPTGI, military deployment version of the Post-Traumatic Growth Inventory; IQR, interquartile range.
Table 2 describes the health characteristics of the sample; 22.3% (95% CI 20.9–23.7, n = 1138) of participants met the criteria for probable CMD and 6.6% (95% CI 5.8–7.6, n = 281) met the criteria for probable PTSD.
Table 2 Description of study participants (health and deployment factors) overall and by post-traumatic growth tertiles (N = 5180)

Numbers may not add up to 5180 because of missing data. Weighted percentages are presenting alongside unweighted cell counts. PTG, post-traumatic growth; DPTGI, military deployment version of the Post-Traumatic Growth Inventory; CMD, common mental disorders; GHQ, General Health Questionnaire; PTSD, post-traumatic stress disorder; PCL-C, Post-traumatic stress disorder CheckList – Civilian version; DAR-5, Dimensions of Anger Responses; IQR, interquartile range; AUDIT, Alcohol Use Disorders Identification Test.
PTG
The median score for PTG in the whole sample was 13 (interquartile range (IQR) 5–24), with 35.1% (95% CI 33.5–36.7, n = 1771) scoring in the lowest tertile (no/a very low degree of PTG), 33.8% (95% CI 32.2–35.4, n = 1764) scoring in the middle tertile (a low degree of PTG) and 31.1% (95% CI 30.0–32.7, n = 1645) scoring in the top tertile (a moderate/large degree of PTG). For male personnel, the median score was 13 (IQR 5–24), with 35.1% (95% CI 33.4–36.9, n = 1586) scoring in the lowest tertile (no/a very low degree of PTG), 34.1% (95% CI 34.1–35.8, n = 1577) scoring in the middle tertile (a low degree of PTG) and 30.8% (95% CI 29.2–32.5, n = 1447) scoring in the top tertile (a moderate/large degree of PTG). For female personnel, the median score was 13 (IQR 5–26), with 34.2% (95% CI 29.5–39.2, n = 185) scoring in the lowest tertile (no/a very low degree of PTG), 31.0% (95% CI 26.6–35.9, n = 187) scoring in the middle tertile (a low degree of PTG) and 34.8% (95% CI 30.1–39.8, n = 198) scoring in the top tertile (a moderate/large degree of PTG).
Subscale scores for PTG, stratified by gender, can be found in Supplementary File 4.
Sociodemographic, military, health and deployment factors associated with PTG
The results from the univariable multinomial logistic regressions for the whole, male-only and female-only samples can be found in Supplementary File 5.
The results from the multivariable multinomial logistic regression model for the whole sample can be found in Supplementary File 6. Table 3 describes the multinomial logistic regression models created to investigate the relationships between sociodemographic, military, health and deployment variables with PTG in male personnel, and Table 4 describes the same models for female personnel.
Table 3 Multivariable multinomial logistic regression model of sociodemographic, health and deployment factors and post-traumatic growth in male personnel (n = 4610)
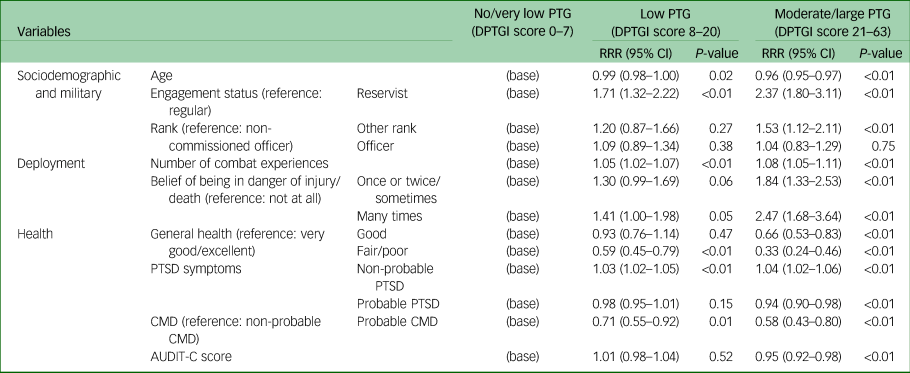
Sampling/response weights have been applied to analyses in this table. PTG, post-traumatic growth; DPTGI, military deployment version of the Post-Traumatic Growth Inventory; RRR, relative risk ratio; PTSD, post-traumatic stress disorder; CMD, common mental disorder; AUDIT, Alcohol Use Disorders Identification Test – alcohol consumption.
Table 4 Multivariable multinomial logistic regression model of sociodemographic, health and deployment factors and post-traumatic growth in female personnel (n = 570)
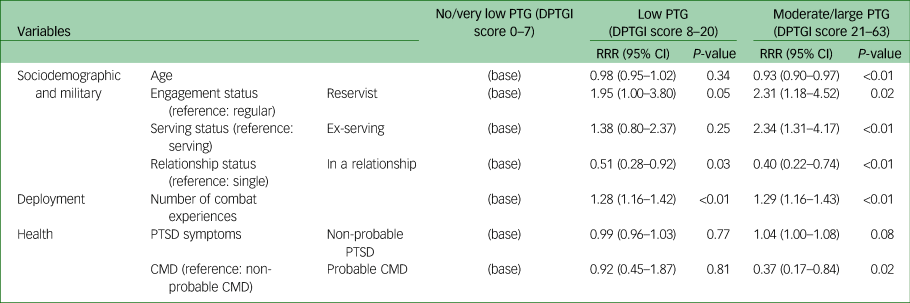
Sampling/response weights have been applied to analyses in this table. PTG, post-traumatic growth; DPTGI, military deployment version of the Post-Traumatic Growth Inventory; RRR, relative risk ratio; PTSD, post-traumatic stress disorder; CMD, common mental disorder.
In the final model for male personnel, reservists, those who reported a greater belief of being in danger of injury/death on deployment, those who reported a greater number of different combat experiences, those of lower rank and those that reported more PTSD symptoms in the non-probable PTSD group were significantly more likely to report a moderate/large degree of PTG compared with those who reported no/a very low degree of PTG. Those with fair/poor general health, probable CMD, those who were older, those who reported greater alcohol consumption and those who reported more PTSD symptoms in the probable PTSD group were significantly less likely to report moderate/large growth and more likely to report no/a very low degree PTG.
In the final model for female personnel, reservists, those who had left service and those who had reported a greater number of different combat experiences were significantly more likely to report a moderate/large degree of PTG compared with those who reported no/a very low degree of PTG. Those with probable CMD, who were in a relationship and were older were significantly less likely to report moderate/large growth and more likely to report no/a very low degree of PTG.
Discussion
This study aimed to examine the prevalence of PTG among UK military serving and ex-serving personnel as a result of deployment to Iraq/Afghanistan, and identify the sociodemographic, military, health and deployment-related factors associated with PTG. Our results showed that 30.8% of male personnel and 34.8% of female personnel reported a moderate/large degree of PTG after an operational deployment. Our results are in keeping with known associations previously found in research of PTG, such as that female personnel and those of younger age experienced greater rates of PTG, those with current probable CMD experienced less PTG, and the noted curvilinear relationship between PTSD symptoms and PTG.Reference Barskova and Oesterreich4,Reference Mark, Stevelink, Choi and Fear8,Reference Vishnevsky, Cann, Calhoun, Tedeschi and Demakis28 This study extends the literature on military/deployment-related factors associated with PTG, including that reservists, those with a greater number of different combat experiences and those who report a greater belief of being in danger on deployment are more likely to report a moderate/large degree of PTG; and health factors associated with PTG, including that those who report better general health and less alcohol use are more likely to report a moderate/large degree of PTG. We also found that health-related factors were associated with male, but not female, serving and ex-serving personnel's experience of PTG; other factors such as having left the service and being single were associated with female, but not male, serving and ex-serving personnel's experience of PTG.
Deployment factors and PTG
We identified that a number of combat/deployment factors are associated with PTG. Greater combat exposure has been reported to be associated with PTG previously,Reference Mitchell, Gallaway, Millikan and Bell11 and it is suggested that stress inoculation and adaptive coping mechanisms might explain this association. However, we also find that reservists, when compared with regular serving personnel, were more likely to report a moderate/large degree of PTG compared with no/very low PTG. Stress inoculation therefore has limited applicability to reservists, who are less likely to deploy frequently compared with regular serving personnel.Reference Stevelink, Jones, Hull, Pernet, MacCrimmon and Goodwin17 It might be more beneficial to understand combat exposure as traumatic events that have the potential to change the basic schemas in the survivor's psyche by restructuring basic assumptions about the world around them or themselves that result in either positive, negative or both positive and negative psychological change.Reference Shakespeare-Finch and Lurie-Beck14,Reference Janoff-Bulman30 Belief of being in serious danger when on deployment has, to our knowledge, only been investigated among those serving during the 1991 Gulf War.Reference Maguen, Vogt, King, King and Litz12 Rumination on the traumatic event has previously been shown to be related to PTG,Reference Barskova and Oesterreich4,Reference Mark, Stevelink, Choi and Fear8 which might increase a person's appraisal of the potential danger associated with the event.
Gender-related differences in PTG
The gender-related differences noted in this study may, in part at least, be related to differences in the lived experience of military deployment between the gender. In the UK, female personnel have only been employed in close combat roles since 2018, roles that traditionally comprised junior rank male personnel. Ex-serving status was a unique aspect associated with PTG for female personnel in our sample. It has been reported in US military veterans that there is a large amount of heterogeneity with regards to experiences of PTG over time,Reference Wu, Kaminga, Dai, Deng, Wang and Pan31,Reference Morgan and Desmarais32 meaning that different subgroups of trauma-exposed military serving and ex-serving personnel might have different trajectories of growth.
Other factors
Several potential variables of interest were not included in our final multivariable models because of our rigorous variable selection procedures (e.g. service, combat role, length of time in a hostile area and length of time since last deployment). It is likely that these variables may have acted as indicators of the type of experiences a servicemember would have during deployment, and it makes sense that they would be superseded by deployment-related factors such as number of combat experiences and belief of being in serious danger of injury or death. Greater time since traumatic event is largely seen as being associated with greater PTG,Reference Barskova and Oesterreich4,Reference Mark, Stevelink, Choi and Fear8 but in our study, PTG was investigated as a result of any Iraq/Afghanistan deployment.
Implications for clinical practice
In our study, reservists, when compared with regular serving personnel, and those who experienced a greater number of different combat experiences were more likely to report moderate/large PTG compared with no/very low PTG. Combat exposure and reservist status have been linked to both positive and negative mental health consequences in previous literature.Reference Mark, Stevelink, Choi and Fear8,Reference Stevelink, Jones, Hull, Pernet, MacCrimmon and Goodwin17 Although the UK armed forces already aims to promote good mental health through Medical Force Protection (i.e. actions taken to promote healthy behaviours or minimise risks regarding ill-heath where possible), it may be beneficial for military leaders to target individuals with high combat exposure and reservists for interventions promoting psychological growth following deployment. Although screening procedures for mental illness have been shown to be ineffective in the armed forces,Reference Rona, Burdett, Khondoker, Chesnokov, Green and Pernet33 screening for combat exposure may identify individuals who (a) might be at increased risk of poor mental health outcomes and (b) might be targeted for interventions that elicit positive psychological growth. Such an approach may be less stigmatising than trying to identify personnel at risk of mental health difficulties.Reference Stevelink, Jones, Jones, Dyball, Khera and Pernet34 However, further research is required to understand whether repeated combat exposure, specific types of combat exposure or increased severity of combat experiences have differing effects on psychological well-being. Intervention post-deployment is a possible avenue for exploration in future research.Reference Tedeschi and McNally5 Increasing severity of PTSD symptoms among those with probable PTSD, as well as probable CMD, were associated with a lower likelihood of reporting moderate/large PTG; however, evidence does suggest that those with mental health difficulties can experience psychological growth after mental health treatment.Reference Murphy, Palmer, Lock and Busuttil16 It is important to note that PTG is beneficial psychological change following a trauma and traditionally includes one or many of the following factors: better appreciation of life, seeing new possibilities in your future, understanding your own personal strength, being better able to relate to others and spiritual change.Reference Tedeschi and Calhoun1,Reference Tedeschi and Calhoun2 As such, interventions that encourage aspects of positive psychology, such as optimism and gratitude, may offer pathways to positive growth similar those who experience PTG.Reference Carr, Cullen, Keeney, Canning, Mooney and Chinseallaigh35
Strengths and limitations
The cross-sectional study design and small sample size of female personnel are notable limitations of our study. Additionally, our representation of combat experiences limited combat scenarios to either experienced or not experienced, and did not investigate the effect of multiple, repeated experiences of those scenarios. This relationship is worthy of separate investigation and beyond the scope of this study. The question used in this study relating to general health does not provide details regarding the physical well-being of our sample, and unique factors such as battlefield injuryReference Tsai, El-Gabalawy, Sledge, Southwick and Pietrzak36 or long-term serious illnessReference Barskova and Oesterreich4 might also affect PTG or even form an independent domain of PTG not currently measured in the DPTGI or PTGI. Further research investigating physical injury and factors of physical health related to PTG is recommended. This study relies on self-report data regarding PTG, and data on external sources assessment of the participants experience of PTG was not available. Tertiles were used as part of this study because no clinical cut-off points were available for the DPTGI or PTGI that were applicable to armed forces personnel.Reference Wu, Kaminga, Dai, Deng, Wang and Pan31 As such, inferences from this sample may not be generalisable to other non-UK military samples. Finally, there was a notable floor effect in our measure. This may be reflective of post-traumatic depreciation; negative changes as a result of deployment to Iraq/Afghanistan,Reference Nordstrand, Hjemdal, Holen, Reichelt and Bøe37 which the DPTGI/PTGI do not measure. Future studies might benefit from using a bi-directional measure of post-traumatic change, which allows participants to report beneficial change (PTG), negative change (post-traumatic deprecation) or no change as a result of their trauma/deployment. Strengths of our study include a robust statistical approach to variable selection; inclusion of pertinent and informative sociodemographic, health and deployment-related variables; and a breakdown of both male and female PTG, which is lacking in the general literature.
In conclusion, this paper identified that a moderate/large degree of PTG is associated with military/deployment-related factors as well as sociodemographic and health-related factors. We also found gender-related differences in the factors associated with experiencing a moderate/large degree of PTG, most notably that health-related factors were associated with PTG in male, but not female, serving/ex-serving military personnel; and relationship and serving status were associated with PTG in female, but not male, serving/ex-serving military personnel. These results will hopefully inform future interventions designed to increase the likelihood of armed forces personnel experiencing beneficial psychological growth over negative mental health outcomes as a result of deployment.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2022.570
Data availability
Requests for data will be considered on a case-by-case basis and are subject to UK Ministry of Defence clearance.
Acknowledgements
We would like to thank N. Jones and R. Rona for their contributions to the inception of this analysis.
Author contributions
D.D. was involved in all aspects of the study, including literature search, study design, data analysis, data interpretation and writing. S.T.-B. was primarily involved in the literature search, and was involved in review and editing the paper. S.A.M.S. and N.T.F. provided supervision with relation to all aspects of the study, including review and editing. N.G. was involved in review and editing the paper.
Funding
The study from which this data were derived received funding from the UK Ministry of Defence (JFC7A/00033). N.T.F. is part-funded by a grant from the UK Ministry of Defence. S.A.M.S. is part-funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London, and the NIHR.
Declaration of interest
D.D. has no interests to declare. N.T.F. is a trustee of a charity for service personnel, veterans and their families. N.G. is the Royal College of Psychiatrists Lead for Trauma and the Military. S.T.-B. is a serving officer in the Royal Army Medical Corps. The views expressed are those of the author(s) and not necessarily those of the National Health Service, NIHR, MoD or Department of Health and Social Care.







 Open access
Open access
eLetters
No eLetters have been published for this article.