



Dementia is a clinical condition that is caused by neurodegeneration and results in cognitive decline and a reduced capacity for independent living.Reference Prince, Bryce, Albanese, Wimo, Ribeiro and Ferri1 Individuals with dementia suffer from a range of symptoms including anxiety, irritability, low mood, hallucinations, delusions and sleep disorders.Reference Cerejeira, Lagarto and Mukaetova-Ladinska2 Alzheimer's disease is the most common type of dementia and accounts for around 60% of cases.Reference Lobo, Launer, Fratiglioni, Andersen, Di Carlo and Breteler3,Reference Qiu, Kivipelto and von Strauss4
Globally, it is estimated that around 55 million people were living with dementia in 2021, with numbers predicted to increase to 78 million in 2030Reference Gauthier, Rosa-Neto, Morais and Webster5 and further to 152.8 million cases in 2050.Reference Nichols, Steinmetz, Vollset, Fukutaki, Chalek and Abd-Allah6 Studies highlight geographical variations in the projected increases across countries and regions.Reference Gauthier, Rosa-Neto, Morais and Webster5,Reference Nichols, Steinmetz, Vollset, Fukutaki, Chalek and Abd-Allah6 The smallest percentage changes in numbers of projected dementia cases are expected in the high-income Asia Pacific (53%) and Western Europe (74%) regions. By contrast, the largest increases are anticipated in North Africa and the Middle East, including the Arab countries. The projected increases in cases can mainly be attributed to population growth and population ageing.
The costs of dementia are important to estimate as the condition incurs an economic burden on healthcare systems and caregivers. In 2009, Wimo and colleagues reported the worldwide cost of dementia as $422 billion, with $142 billion (34%) spent on informal care.Reference Wimo, Seeher, Cataldi, Cyhlarova, Dielemann and Frisell7 A more recent study using a similar methodology estimated the cost of dementia in the Arab world in 2009 to range from $4.2 billion to $6.7 billion, with dementia costs accounting for over 0.75% of the total gross domestic product (GDP) in Mauritania, Iraq and Egypt, whereas the economic burden for the Gulf Cooperation Council was estimated at less than 0.25% of the GDP.Reference Wimo, Jonsson and Winblad8 A recent study by Wimo et al. found that the annual global societal costs of dementia in 2019 were US $1313.4 billion for 55.2 million people with dementia.Reference Wimo, Seeher, Cataldi, Cyhlarova, Dielemann and Frisell7 These costs included direct medical costs (US $213.2 billion, 16%), direct social sector costs such as long-term care (US $448.7 billion, 34%), and informal care costs (US $651.4 billion, 50%). This research showed that although the majority of people with dementia live in low- and middle-income countries, the highest total and per-person costs are observed in high-income countries. Low- and middle-income countries accounted for 61.3% of people with dementia but only 26% of total costs, whereas high-income countries, with 38.7% of people with dementia, bore 74% of total costs. This discrepancy can be attributed to differences in healthcare systems, resource availability and accessibility, as well as varying costs of care across countries. This study did not examine individual countries but rather focused on categories of countries according to their income levels.Reference Wimo, Seeher, Cataldi, Cyhlarova, Dielemann and Frisell7
Given the lack of updated estimates regarding the cost of dementia in the Arab world, the present work aims to calculate this economic burden for the year 2021 using the same methodology as that used by Wimo et al.Reference Wimo, Seeher, Cataldi, Cyhlarova, Dielemann and Frisell7–Reference Wimo, Guerchet, Ali, Wu, Prina and Winblad11
Method
The primary aim of this study was to calculate the prevalence and cost of dementia in Arab countries. To achieve this, we first needed to accurately estimate the number of individuals living with dementia in each Arab country. Our methodology, based on a model derived from previous studies,Reference Wimo, Seeher, Cataldi, Cyhlarova, Dielemann and Frisell7–Reference Wimo, Guerchet, Ali, Wu, Prina and Winblad11 was as follows.
Data collection
We collected population distribution and age-band data for both genders for all countries from the United Nations’ website.12,13 This foundational data allowed us to perform our calculations.
Data extraction
We concentrated on the data specifically relevant to Arab countries and extracted the necessary information for our analysis.
Prevalence estimates
Table 1 presents dementia prevalence estimates categorised by age bands and gender.Reference Cao, Tan, Xu, Hu, Cao and Dong14 This information was used to calculate the number of individuals living with dementia in each Arab country.
Table 1 Global dementia prevalence estimates according to age bands and across genders
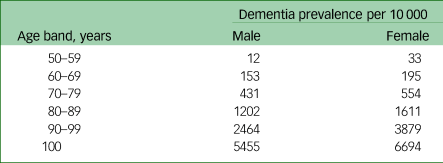
This table shows dementia prevalence estimates according to age bands and across gendersReference Cao, Tan, Xu, Hu, Cao and Dong14, which we used to calculate the numbers of individuals with dementia in individual Arab countries.
Application of prevalence estimates
We applied the prevalence figures from Table 1 to the population data for each Arab country. This enabled us to estimate the number of individuals living with dementia in each country, considering both the 10-year age bands and the gender distribution.
Aggregation of dementia cases
We summed the estimated numbers of dementia cases across all age bands and genders to determine the total number of individuals living with dementia in each Arab country. To calculate the prevalence, we divided the numbers of individuals with dementia aged 50+ and 60+ years by the total populations aged 50+ and 60+ years for each Arab country.
Cost calculation
Direct cost
The direct cost of dementia per person in each Arab country was calculated using GDP per capita, based on purchasing power parity (PPP) and the World Bank Income Classification. As depicted in Table 2, we collected GDP per capita PPP data for each Arab country and identified the World Bank Income Classification (low-income, lower-middle-income, upper-middle-income or high-income) from the most recent World Bank estimates.15
Table 2 GDP per capita PPP and income classification for Arab countries for the year 2021
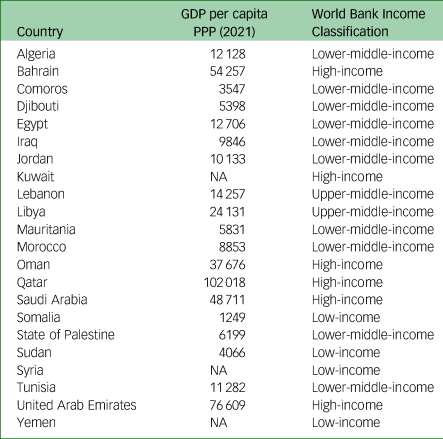
For countries with missing GDP per capita PPP data, values were obtained from the corresponding World Bank income group as follows:
(a) Kuwait (high-income, 2021): 48 894
(b) Syria (low-income, 2021): 2327
(c) Yemen (low-income, 2021): 2327.
We considered the cost per patient for the resources used in treating dementia in relation to the GDP per capita based on PPP. Wimo et al estimated that the direct cost per person with dementia is connected to the GDP per capita PPP.Reference Wimo, Seeher, Cataldi, Cyhlarova, Dielemann and Frisell7 Their study also demonstrated that the direct costs of dementia vary among countries, depending on the World Bank income classification, as shown in Table 3.
Table 3 Direct cost of dementia in relation to country income
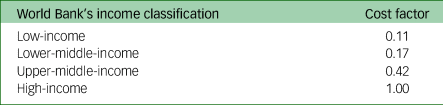
To estimate the direct cost per person with dementia in each Arab country, we multiplied the GDP per capita PPP by the corresponding factor based on income classification. By following this method, we were able to calculate the direct cost of dementia per person for each Arab country, taking into account the GDP per capita PPP and income classification. This resulted in an amount in United States Dollars (USD).
Indirect costs
To calculate indirect costs, the hourly wage of caregivers needs to be available. We extracted wage information for the year 2021 from data provided by the International Labour Organization (ILO), which includes the average monthly earnings in USD for various countries in the year 2021.16 Most Arab countries had no available data, apart from Comoros ($253.25), Egypt ($186) and Jordan ($475). For countries with missing data, the average wage was determined using calculated average monthly wages from the ILO data-set for the respective country category according to the World Bank. Table 4 depicts the calculated average monthly wages by World Bank income classification in 2021 (USD).
Table 4 Calculated average monthly wages by World Bank income classification in 2021 (USD)

Numbers of dementia cases among individuals aged 50 years and above, along with monthly wages for each country, were collected from ILO and calculated or estimated as described before. This information was used to calculate the hourly wages in USD.
The cost of dementia was calculated under two different scenarios, as follows.
(a) Best case: in this scenario, it is assumed that caregivers spend 1.6 h per day providing care to individuals with dementia living in the community. The total cost is calculated by multiplying the hourly wage, the number of individuals with dementia living in the community (90% of the dementia population) and the number of hours spent per day by caregivers, for 365 days.
(b) Worst case: in this scenario, it is assumed that caregivers spend 3.7 h per day providing care to individuals with dementia living in the community. The total cost is calculated by multiplying the hourly wage, the number of individuals with dementia living in the community (which accounts for 99% of the dementia population, owing to cultural traditions in most Arab countries, where people with dementia are often cared for by informal caregivers such as spouses or offspring within their own household) and the higher number of hours spent per day by caregivers, for 365 days. The hourly wage of a retired caregiver was considered to be equivalent to the hourly wage of a caregiver of working age; although this strategy was not ideal, it was consistent with previous research on the burden of dementia.Reference Wimo, Jonsson and Winblad8
Data processing and visualisation were performed using a range of Python libraries and software. The core data manipulation and analysis tasks were carried out using pandas 1.4.417 and NumPy 1.21.5.Reference Oliphant18 For data visualisation, the matplotlib library 3.5.2Reference Hunter19 was employed. Geospatial data visualisation was achieved using Cartopy 0.21.1.20 All of these libraries were used within the Python 3.9 programming environment.21
Results
Table 5 shows the prevalence of dementia in the Arab world in the population aged 50 and 60 years or older. Figure 1 shows the prevalence of dementia in those aged over 60 years on a map of the Arab world.
Table 5 Prevalence of dementia in the Arab world
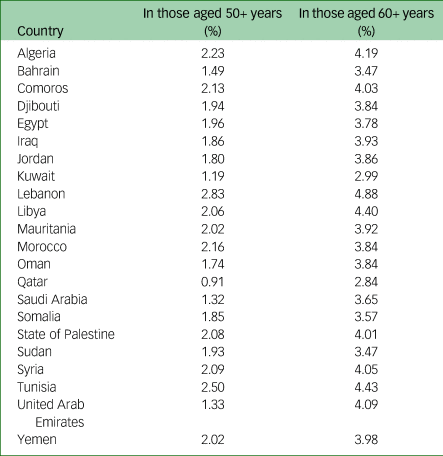
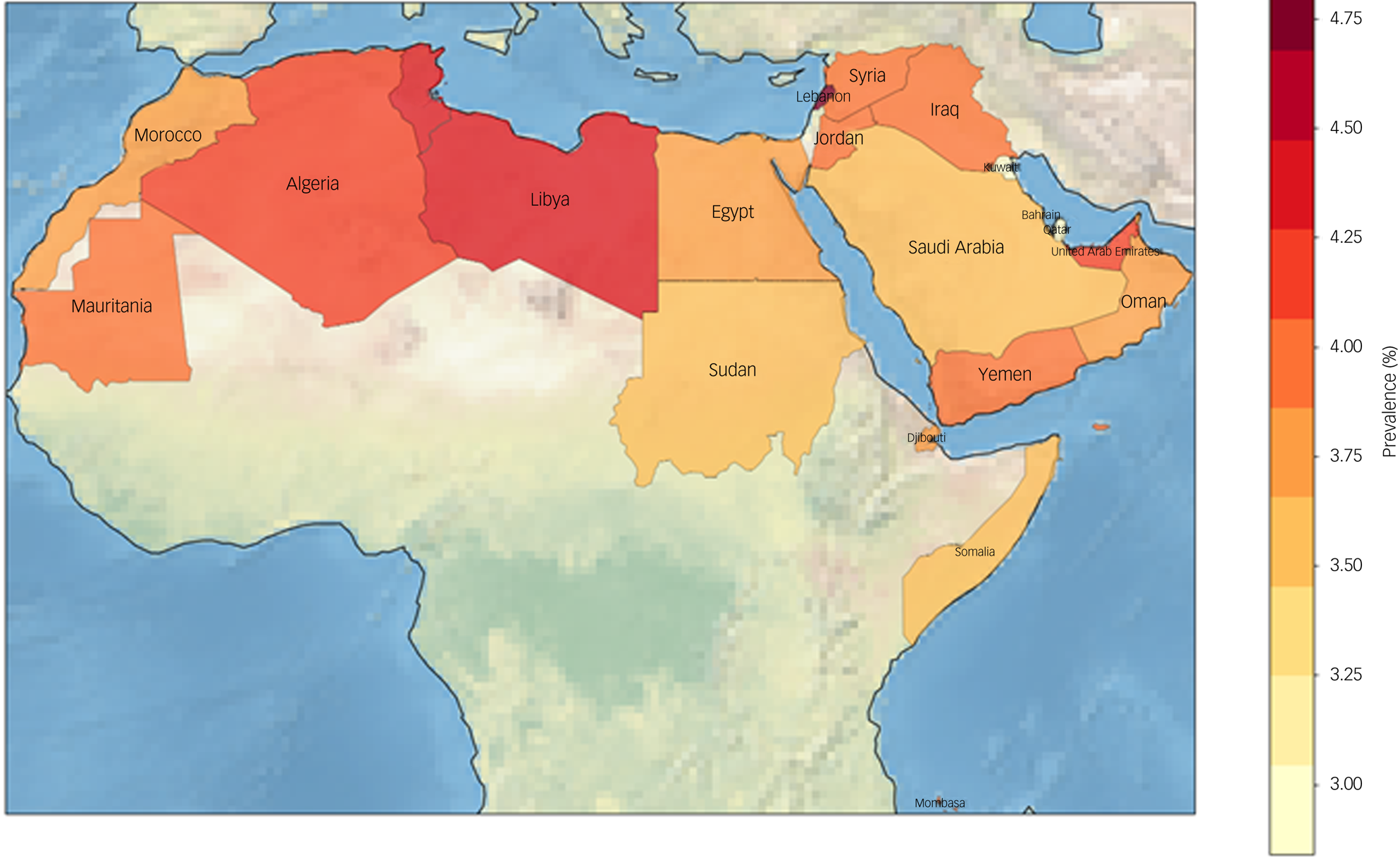
Fig. 1 Prevalence of dementia in the Arab world. The map reports the prevalence of dementia in the Arab world in the population over the age of 60 years.
Supplementary Tables 1 and 2, available at https://doi.org/10.1192/bjo.2023.517, depict the total population and dementia figures for the countries belonging to the Arab world. The highest estimates of those living with dementia aged of 50 and 60 years or older were for Egypt (333 950 and 314 359), Algeria (182 966 and 173 890) and Morocco (172 417 and 164 015). The total direct cost of dementia in the region was estimated at $8184.9 million (range: $1.4– $3475.2 million) for those above 50 years of age. Table 6 shows estimates of direct costs attributed to dementia.
Table 6 Direct costs of dementia in individual Arab countries

Table 7 presents the indirect costs of dementia in individual Arab countries, considering best- and worst-case scenarios for the percentage of individuals with dementia living in the community. Hourly wages are given in USD, and indirect costs are shown for both scenarios; the mean value is also given. The highest indirect cost in the best-case scenario was seen for Saudi Arabia ($853 139 364), whereas the lowest was for Comoros ($1 875 531). In the worst-case scenario, Saudi Arabia still had the highest indirect cost ($2 170 176 331), and Somalia had the lowest ($21 667 422). The highest hourly wages were found for Bahrain, Kuwait, Oman, Qatar and the United Arab Emirates ($22.75), whereas the lowest were for Somalia and Syria ($0.60). Overall, the total indirect cost for the Arab world ranged from $2 248 050 976 in the best-case scenario to $5 672 305 899 in the worst-case scenario, with a mean value of $3 983 257 396. Table 8 presents the total dementia care costs, both direct and indirect, in Arab countries, under best, worst and mean scenarios. Costs are shown in USD.
Table 7 Indirect costs of dementia in individual Arab countries
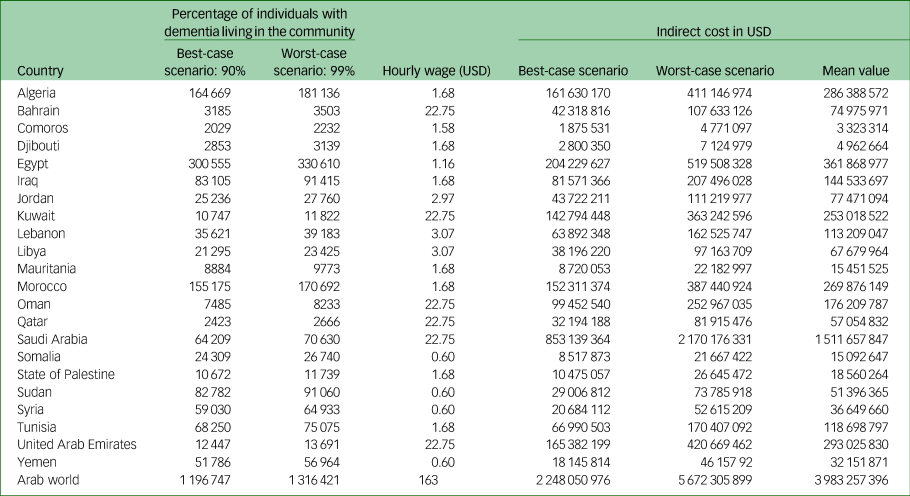
Table 8 Total dementia care costs (direct and indirect) in Arab countries: best, worst and mean scenarios
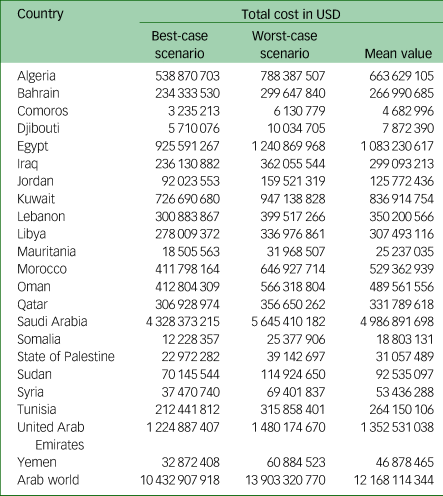
The figures reveal considerable variation in costs across the Arab countries. Saudi Arabia incurred the highest mean dementia care costs, amounting to $4 986 891 698. By contrast, Comoros had the lowest mean cost at $4 682 996. Other countries, including the United Arab Emirates, Egypt and Algeria, also had comparatively high mean costs, exceeding $1 billion, $1 billion and $663 million, respectively. At the other end of the spectrum, countries including Djibouti, Somalia and the State of Palestine had relatively low mean costs, ranging between $7 872 390 and $31 057 489. Further, the combined mean dementia care cost for the entire Arab world was $12 168 114 344. Supplementary Table 3 depicts the ratio between the indirect and total cost of dementia in Arab countries. Table 9 and Fig. 2 depict the total cost of dementia as a percentage of GDP for various countries in the Arab world, illustrating the economic burden of dementia in each country. Notably, the percentages ranged from a low of 0.05% in Sudan to a high of 0.44% in Lebanon. In addition, some countries, including Kuwait (0.40%) and Bahrain (0.34%), exhibited higher percentages of dementia costs relative to GDP compared with others in the region. The table also includes an average percentage for the entire Arab world, which was calculated to be 0.18%.
Table 9 Total cost of dementia as a percentage of GDP by country in the Arab world
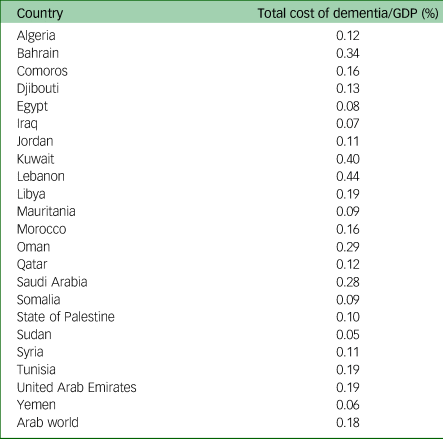
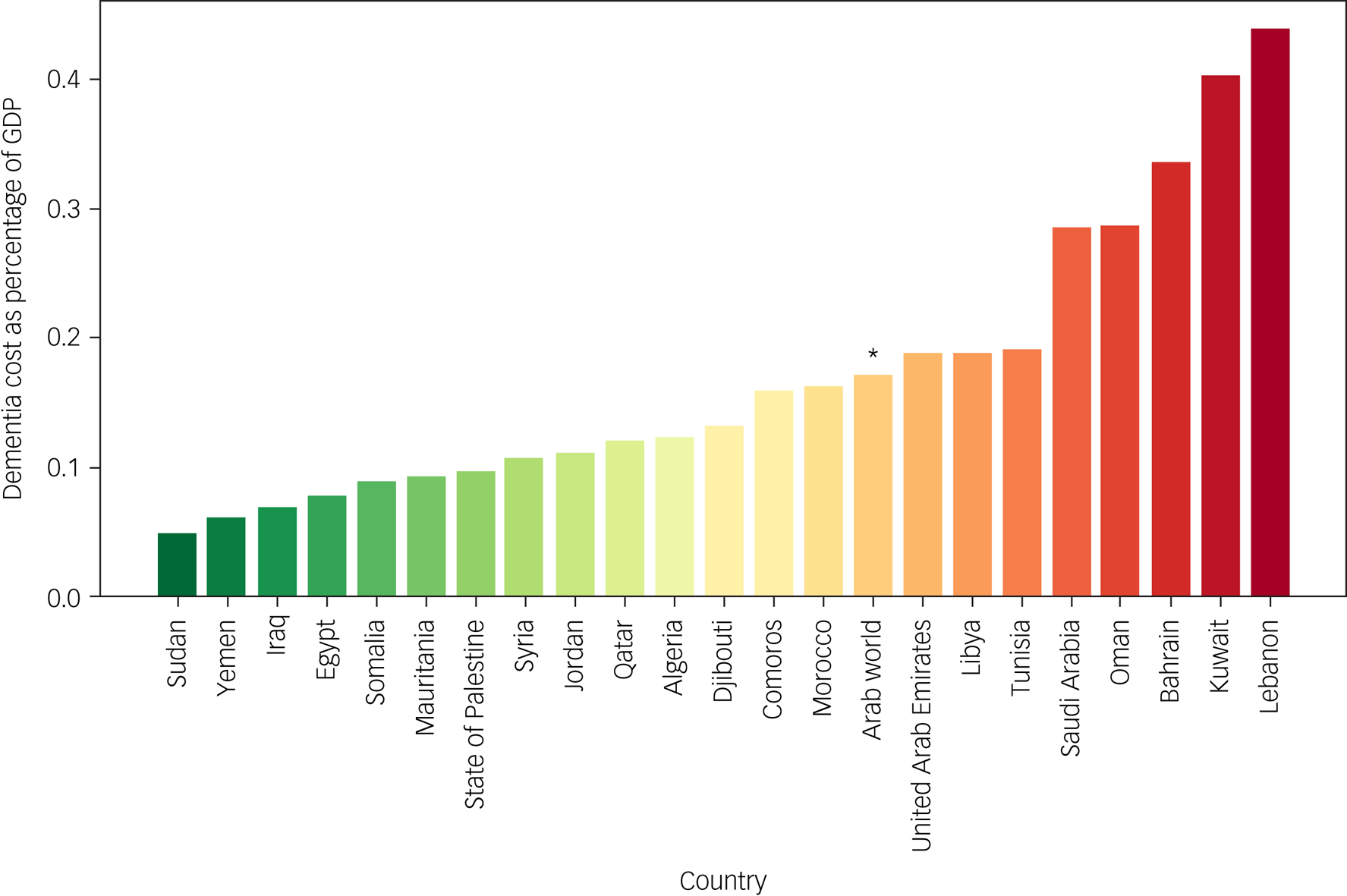
Fig. 2 Total cost of dementia as a percentage of GDP in the Arab world countries.
The asterisk denotes the total cost of dementia as a percentage of GDP in the Arab world as a whole.
Discussion
The prevalence of dementia in the Arab world has become an increasingly important public health issue, as evidenced by the growing number of affected individuals and the associated economic burden on societies. This paper seeks to emphasise the significant issue of dementia in the Arab world, with the goal of attracting the attention of decision makers to invest in research and specialised services for older adults, particularly those affected by dementia. The choice of this topic was based on the scarcity of research focusing on dementia in the Arab world. A systematic review by El-Metwally et al found only 18 studies that investigated the prevalence of dementia in the region, with only six of them being community based.Reference El-Metwally, Toivola, Al-Rashidi, Nooruddin, Jawed and AlKanhal22–Reference Farrag, Farwiz, Khedr, Mahfouz and Omran28 A 2017 review of dementia prevalence studies in Egypt found that dementia prevalence ranged from 2.01% to 5.07%.Reference Elshahidi, Elhadidi, Sharaqi, Mostafa and Elzhery29 One study from the upper desert areas of Egypt reported that the total prevalence of Alzheimer's dementia was 1% among the population aged 50 years and more, reaching 2.9% at 70–79 years.Reference EL Tallawy, Farghaly, El Hamed, Badry, Usama and Shehata30
Although the main focus of this study was the prevalence of dementia, encompassing both diagnosed and undiagnosed cases, it is worth briefly mentioning the challenge of undiagnosed dementia. As underscored in the World Alzheimer Report 2021: Journey through the Diagnosis of Dementia, obtaining a diagnosis remains a significant issue for people living with dementia; Alzheimer's Disease International (ADI) estimates that globally, 75% of people with dementia are not diagnosed, with that percentage believed to be as high as 90% in some lower- and middle-income countries.Reference Gauthier, Rosa-Neto, Morais and Webster5 Despite the limited data and the focus of the ADI report on diagnosis rates rather than dementia prevalence, the authors anticipate a considerably high percentage of undiagnosed cases in the Arab world.
According to our estimates, there were 1 329 729 individuals with dementia in the Arab world in 2021. The prevalence of dementia varied across countries, with the highest rates observed in Tunisia (4.20%) and the lowest rates in Qatar (1.57%). The prevalence of dementia in the Arab world was 2.16% in those aged 50+ years and 3.84% in those aged 60+ years. The highest estimates of those living with dementia above the age of 50 and 60 years were in Egypt (312 399), Algeria (169 784) and Morocco (159 890), whereas Comoros had the lowest number (1166). There were differences in dementia prevalence rankings between the 50+ and 60+ age groups across different countries. For instance, the United Arab Emirates experienced a significant increase in ranking, moving from fourth place with a 1.33% prevalence in the 50+ age group to 18th place with a 4.09% prevalence in the 60+ age group. Conversely, Morocco saw a considerable decrease in ranking. However, some countries, including Qatar, Kuwait, Tunisia, Syria and Lebanon, showed no difference in their rankings between the two age groups. These variations in dementia prevalence rankings between age groups can be attributed to factors such as population age distribution, dementia risk factors, access to healthcare and support services, and cultural and lifestyle factors. In this study, the differences in ranking were probably due to demographics, specifically the differences in population age distribution between the countries. A larger proportion of older adults in the 60+ age group could lead to a substantial increase in dementia prevalence, owing to the increased risk of dementia with age, whereas countries with a younger population might have a lower prevalence, resulting in a smaller change in ranking.
This study found an economic burden of dementia for those aged 50 years and above amounting to a total of 10.43 billion USD in the best-case scenario and 13.90 billion USD in the worst-case scenario for the year 2021. It is important to note that these costs are estimates rather than precise calculations. Using a comparable methodology, the cost estimates for the year 2009 in the Arab region were found to be 4.212 billion USD for the best-case scenario and 6.707 billion USD for the worst-case scenario. There are several reasons for this significant increase in the economic burden of dementia, including demographic changes; for instance, the total population above the age of 60 in 2021 was about 2.5 times that in 2009. The correlation between GDP per capita and direct cost has also been updated, and an increase in the average GDP per capita estimate for the region was found. The direct costs of dementia care in Arab countries are influenced by each country's GDP per capita and income classification, with higher costs observed in high-income countries such as Saudi Arabia (2039 USD per capita) and the United Arab Emirates (2371 USD per capita). By contrast, lower costs were seen in lower-middle-income countries such as Yemen (223 USD per capita) and Djibouti (256 USD per capita).
Indirect costs, which include loss of productivity due to caregiving, can also significantly contribute to the overall economic burden of dementia. These costs are typically higher in countries with larger proportions of informal care provision by family members or friends. For instance, informal caregiving costs were found to be exceptionally high in certain countries, including Egypt, Algeria and Morocco; by contrast, the direct costs, which are correlated with GDP per capita, were much lower in those countries. These observations probably reflect the prevailing structure of care services, which tend to rely heavily on informal rather than formal caregiving arrangements.
As this study examined dementia prevalence in 2021, when the COVID-19 pandemic was raging, it is essential to acknowledge the potential influence of the pandemic on dementia care and its costs. One cannot attempt to ignore the devastating impact of the COVID-19 pandemic on humanity during 2020 and 2021. This global crisis has strained healthcare systems and posed significant challenges for most individuals, especially those living with dementia and their caregivers. Factors such as heightened social isolation, disrupted healthcare services and increased stress levels may contribute to the exacerbation of dementia symptoms and increase the risk of developing the condition. Furthermore, COVID-19 infections have been linked to higher risk of cognitive decline, particularly among older adults.Reference Azarpazhooh, Amiri, Morovatdar, Steinwender, Ardani and Yassi31,Reference July and Pranata32
Matias-Guiu et al found that living in care homes was the most significant factor for increased risk of infection and death among dementia patients.Reference Matias-Guiu, Pytel and Matías-Guiu33 This finding suggests that the pandemic may have disproportionately affected individuals with dementia in care facilities, which could have implications for the costs of dementia care. Cascini et alReference Cascini, Agabiti, Marino, Acampora, Balducci and Calandrini34 assessed the incidence of SARS-CoV-2 infection and COVID-19-related death among dementia patients, identifying risk factors for both infection and mortality. Whereas this discussion paper does not directly investigate the relationship between COVID-19 and dementia prevalence or care in the Arab world, future research should explore the influence of the pandemic on the overall dementia landscape in the region, taking into account its potential impact on the cost of dementia care.Reference Matias-Guiu, Pytel and Matías-Guiu33,Reference Cascini, Agabiti, Marino, Acampora, Balducci and Calandrini34
The present study had some limitations, including its reliance on secondary data sources for population, prevalence and cost estimates. This may have introduce some inaccuracies in our calculations, as the quality and completeness of the data varied among countries. In addition, the cost estimates may not fully capture the complexity of dementia care provision in each country, as they were based on GDP per capita and income classification rather than detailed cost data from individual countries. This analysis focused on the Arab world, and our findings may not be generalisable to other regions with different demographic, economic and healthcare characteristics owing to economic or political instability in some of the Arab countries, potential bureaucratic or regulatory hurdles, and a lack of standardised neuropsychometric research instruments in the region.Reference Al Sinawi, Qassem and Al Harrasi35,Reference Javaid, Al-Zahmi and Abbas36 Another limitation to consider is the potential influence of the COVID-19 pandemic on dementia care and its costs during the study period, which examined dementia prevalence in 2021 when the pandemic was still ongoing. The pandemic has strained healthcare systems and introduced additional challenges for individuals living with dementia and their caregivers, as discussed earlier. Factors such as heightened social isolation, disrupted healthcare services and increased stress levels could have affected dementia symptoms and risks, and such effect may not have been fully captured in our analysis. Moreover, the implications of the pandemic for the cost of dementia care, as suggested by Matias-Guiu et al and Cascini et al,Reference Matias-Guiu, Pytel and Matías-Guiu33,Reference Cascini, Agabiti, Marino, Acampora, Balducci and Calandrini34 might not be adequately reflected in our estimates. Future research should further investigate the influence of the pandemic on the overall dementia landscape in the Arab world, considering its potential impact on care costs as a factor within the study's limitations.
Despite these limitations, we hope this study will provide useful insights into the prevalence and costs of dementia in Arab countries. These findings could help to inform policymakers, healthcare providers and researchers in their efforts to address the challenges posed by dementia in the region. As the population in Arab countries continues to age and the prevalence of dementia risk factors increases, it is crucial to invest in prevention, early detection and support services to reduce the impact of dementia on individuals, families and society. To tackle the growing issue of dementia in the Arab world, we make the following recommendations. (a) Enhance investment in dementia research to increase understanding of regional prevalence, risk factors and cultural aspects. This will aid in creating targeted interventions and policies for dementia prevention and care. (b) Strengthen national dementia strategies by improving early diagnosis, offering integrated care services and fostering dementia-friendly communities. This will reduce stigma, enhance quality of life for people with dementia and support their caregivers. (c) Create and implement training programmes for healthcare professionals, particularly in primary care settings, to improve dementia diagnosis and management. In accordance with the World Alzheimer 2022 report, emphasise person-centred care, caregiver support, evolving clinical roles and dementia education. This will result in a stable, effective, and cost-efficient care economy for people with dementia and their families.Reference Gauthier, Webster, Servaes, Morais and Rosa-Neto37 (d) Develop specialised mental health services for older adults, focusing on early identification, prevention and intervention. Collaborate with multidisciplinary teams to provide comprehensive, integrated care promoting mental well-being and quality of life for older persons in the Arab world. (e) Promote collaboration between governments, researchers, non-governmental organisations and international organisations to share best practices, resources and data on dementia care and support. (f) Increase funding for public awareness campaigns to enhance dementia knowledge and encourage early detection and intervention, reducing the societal and economic impact of dementia in the Arab world. (g) Implement dementia-friendly environment design principles from the World Alzheimer Report 2020 to improve quality of life for people with dementia and help them to maintain their abilities.Reference Zeisel, Bennett and Fleming38
In conclusion, this paper highlights the significant issue of dementia in the Arab world and underscores the urgent need for action from decision makers to invest in research and specialised services for older adults, particularly those affected by dementia. With the projected increase in the prevalence of dementia in the coming decades, addressing this public health challenge is critical to ensuring the well-being of older adults and reducing the economic burden on societies in the region.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2023.517.
Data availability
The data-sets used and analysed during the current study have been cited and are available upon request. The data that support the findings of this study are available from the corresponding author, S.F.J., upon reasonable request.
Authors’ contributions
T.Q.: conceptualisation, methodology, writing – original draft preparation, supervision. L.I.: data curation, writing – original draft preparation, supervision, conceptualisation. H.A.-S.: conceptualisation, data curation, writing – original draft preparation. W.N.: data curation, writing – reviewing and editing. D.A.-A.: methodology, data analysis. S.F.J.: data analysis, writing – reviewing and editing.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.














 Open access
Open access
eLetters
No eLetters have been published for this article.