



Case report
A pregnant 26-year-old woman (gravida 1, para 0) was referred to our hospital after an echocardiogram screening 19 weeks of gestation revealed a suspected right-sided aortic arch and vascular ring in the fetus. An initial ultrasound examination at 22 weeks of gestation confirmed that the fetus had a right aortic arch, right ductus arteriosus, and anomalous origin of the left-sided innominate artery from the main pulmonary trunk (Fig. 1a). There were no signs of a vascular ring or intracardiac anomalies. The baby was born at 39 weeks and 4 days of gestation, weighing 3195 g, without asphyxia. The left-sided innominate artery root was patent at birth (Fig. 1b). Prostaglandin preparations were initially considered for maintaining the patency of the root. However, concerns about perfused blood flow to the head from the contralateral common carotid artery via Willis’ artery ring, as well as concerns about the development of high pulmonary blood flow due to retrograde blood flow from the head, promoted us to refrain from utilising prostaglandin preparations. Both the right and left sides of the ductus arteriosus closed at 12 h of age. Furthermore, a head MRI examination on day 6 revealed no findings suggestive of brain ischaemia, such as cerebral infarction or cerebral atrophy (Fig. 2a,b). The systolic blood pressure in the left upper extremity was approximately 20–30 mmHg lower than that in the right upper extremity. Contrast-enhanced CT on day 7 indicated disruption of blood flow between the pulmonary artery and left brachiocephalic artery and emergence of blood supply from the vertebral artery to the left subclavian artery through the Willis’ artery ring (Fig. 2c). The patient was discharged on day 8 because his general condition was good and there was no obvious paralysis or muscle weakness in the left upper limb. At the time of the manuscript submission, the patient aged 5 months, showing good development and growth without abnormal neurological findings.
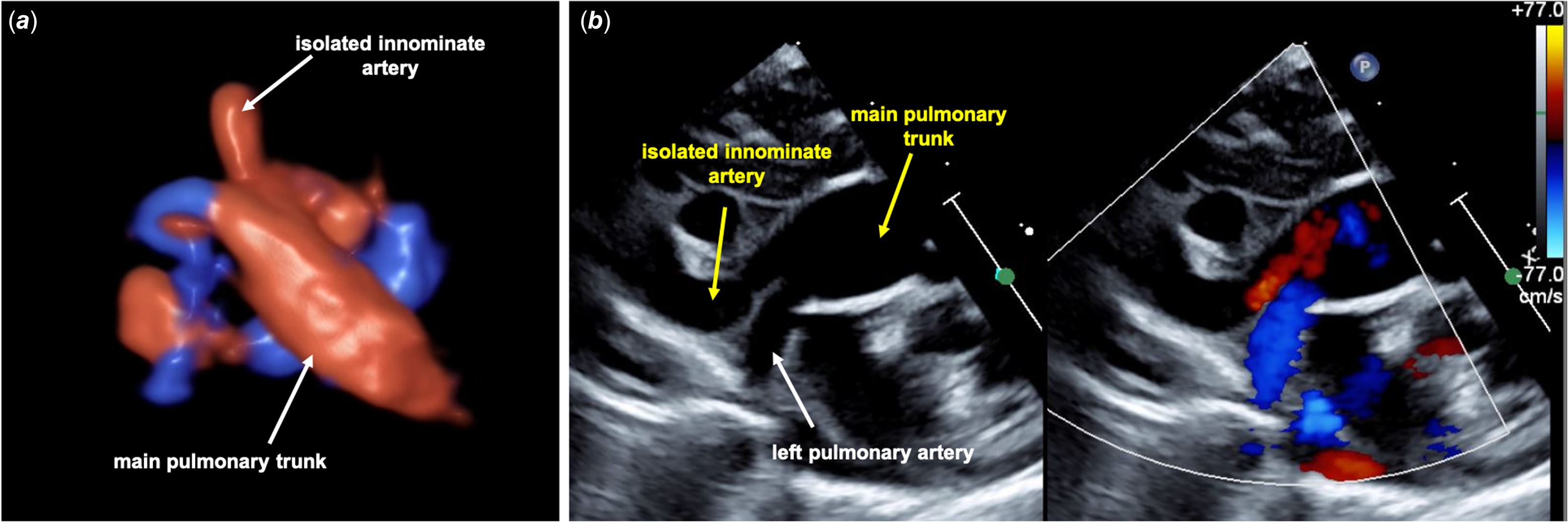
Figure 1. (a) Prenatal ultrasonographic three-dimensional picture of isolated innominate artery. Trans maternal abdominal echo at 35 weeks of gestation shows left-sided innominate artery arising from the main pulmonary trunk. (b) Postnatal ultrasonographic two-dimensional picture of isolated innominate artery. Sagittal view of the pulmonary trunk shows that the root of isolated innominate artery is patent at 3 h of age.
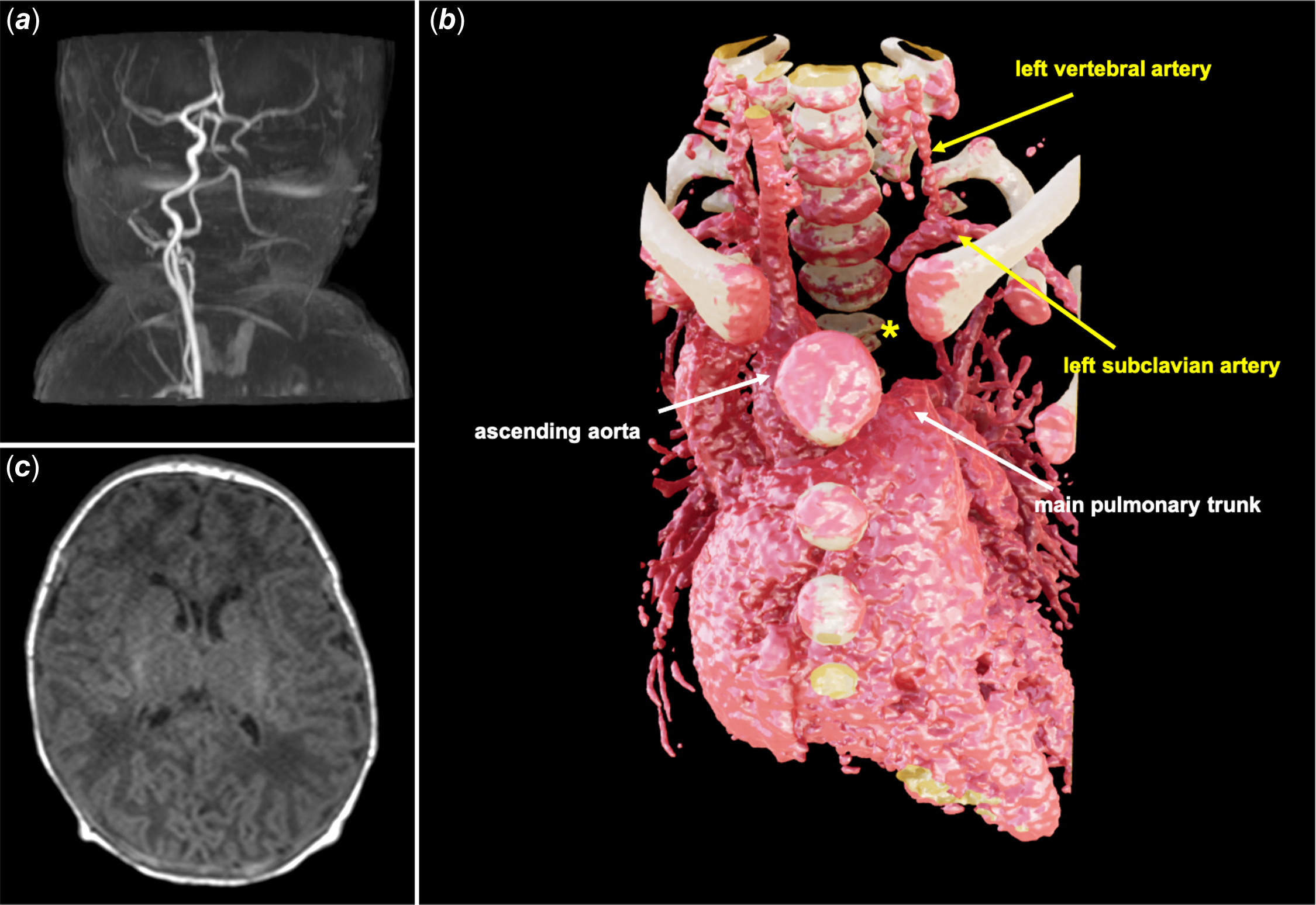
Figure 2. (a) Brain MRI images at day 6. Magnetic resonance angiography showing left-sided cerebral arteries perfused from the contralateral common carotid artery via Willis’ artery ring. (b) T1 weighed image showing no signs of cerebral infarction or cerebral atrophy. (c) Enhanced CT image heart at day 7 showing disruption of blood flow between the pulmonary artery and the left-sided innominate artery. The site of disruption is marked with an asterisk. It also shows disappearance of the left common carotid artery and blood supply from the vertebral artery to the left subclavian artery.
Discussion
Aortic arch anomalies are explained by the Edwards hypothetic double aortic arch in which selective regression of various parts of either arch demonstrates various arch anomalies. Reference Crawford1 Such anomalies may occur via interruptions at two sites in the double aortic arch: in the left posterior arch distal to the ductus and the left anterior arch proximal to the left common carotid artery. Reference Fong and Venables2 However, few reports have described prenatally diagnosed left-sided isolated innominate arteries. Reference Li, Zhang, Yan and Pei3,Reference Hao, Zhang and Zhao4 The root of the left-sided innominate artery may be narrowed or occluded to various degrees after birth due to regression of the left ductus arteriosus originating from the left sixth arch. Reference Park5 However, most cases are asymptomatic, with mild symptoms, such as a weakened peripheral pulse in the left upper limb due to mild ischaemia of the left subclavian artery. Reference Gowda, Bhat, Jayaranganath and Hegde6 Immediately after ductus arteriosus regression, the circulation of the left extremity is compensated by retrograde flow from the left vertebral artery. Subsequently, the blood supply from the internal thoracic and intercostal arteries via the collaterals gradually increases, replacing the supply from the vertebral artery. However, a small number of cases have been reported wherein cerebral atrophy or vertebrobasilar artery insufficiency developed during infancy or later due to a substantial amount of blood diversion from the vertebral artery to the subclavian artery, requiring revascularization surgery. Reference Gowda, Bhat, Jayaranganath and Hegde6–Reference Le Bret, Leobon and Roubertie8
The decision to perform surgery before symptom onset remains uncertain, given that the accurate prevalence of symptomatic patients with this rare condition is unclear. Based on previous reports describing most patients as asymptomatic, we decided to monitor our patient symptom onset. Since some cases have been reported to develop the symptoms during adulthood, lifelong follow-up might be required. Reference Li, Zhang, Yan and Pei3 The accuracy of prenatal diagnosis is steadily improving, and the prenatal diagnosis of such a condition, as in this case report, could enable us to observe the patients prospectively. This approach may assist in elucidating the accurate prevalence and clinical features in symptomatic patients and provide insights into a better clinical decision-making process. In this case, our initial observation focused on the right aortic arch and right ductus arteriosus, and subsequent exploration, guided by the knowledge that 98% of these patients could have another cardiac anomaly, enabled us to find an isolated left-sided innominate artery. Reference Maier and Van der Woude9
In conclusion, in cases of an isolated left-sided innominate artery, occlusion or stenosis of the innominate artery root associated with closure of the ductus arteriosus after birth could be tolerated. However, follow-up should be performed by paying attention to upper limb weakness and central nervous system complications.
Acknowledgements
A three-dimensional image of enhanced CT was constructed by Viewtify® supplied by SCIEMENT, Tokyo, Japan. We would like to thank Editage (www.editage.jp) for English language editing.
Financial support
None.
Competing interests
None.
Ethical standards
Written informed consent was obtained from the patient’s guardian for the publication of this case report and the accompanying images.


