We thank Houyel et al. for their robust and intriguing response to our own commentary on their description of an interesting heart with so-called “heterotaxy.”Reference Houyel, de Bellaing and Bonnet1–Reference de Bellaing, Bonnet and Houyel3 They take us to task, however, in their eyes, for having cited incorrectly some of their own concepts. We wonder whether their criticisms are entirely justified? Disputation is the life blood of science. It follows that the dialectic will never be achieved without appropriate thesis and antithesis. We thank the Editor, therefore, for allowing us the opportunity to respond to those criticisms that, in our opinion, depend on the inferences made by the Parisian group, rather than representing our intentions when submitting our commentary. We also had a degree of difficulty in following the logic of their own approach. Thus, they question our dependence on the writings of St Hilaire, arguing that it is inappropriate to rely on “anteriority.” Yet they then cite the importance of the “anteriority” of the definition offered by the International Nomenclature Committee, even though this is now more than 10 years old. Should we not now be basing our definitions on the most recent and reliable evidence?
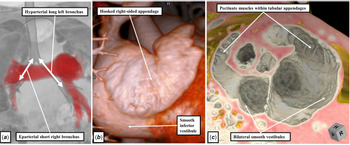
In this regard, we emphasised that, nowadays, it is increasingly possible, when using modern techniques, to distinguish the extent of the pectinate muscles relative to the atrial vestibules. On the basis of the criterions developed by Van Praagh, this feature is the most reliable means of distinguishing the morphology of the atrial appendages. The Parisian authors are disingenuous when suggesting that the pectinate muscles cannot be seen within the right-sided appendage in the figure we provided to substantiate this notion. We were surprised in their interpretation of the apex of the appendage, admittedly not well visualised in our figure, as representing its entire extent. We retain the belief that our figure shows that the pectinate muscles truly encircle the vestibule on the right side. Perhaps it is failure to recognise the extent of the appendage that accounts in part for their misinterpretation? In this light, we can now share a recently encountered case, which shows the features of the right-sided morphologically left appendage when the pectinate muscles truly fail to encircle the vestibule of the right atrioventricular junction (Fig 1). It is also of interest that, in this individual, the bronchuses were usually arranged. Hence, using the criteria of the Parisian group, the individual is heterotaxic. From the stance of the heart, nonetheless, there is unequivocal evidence of left isomerism (Fig 1).
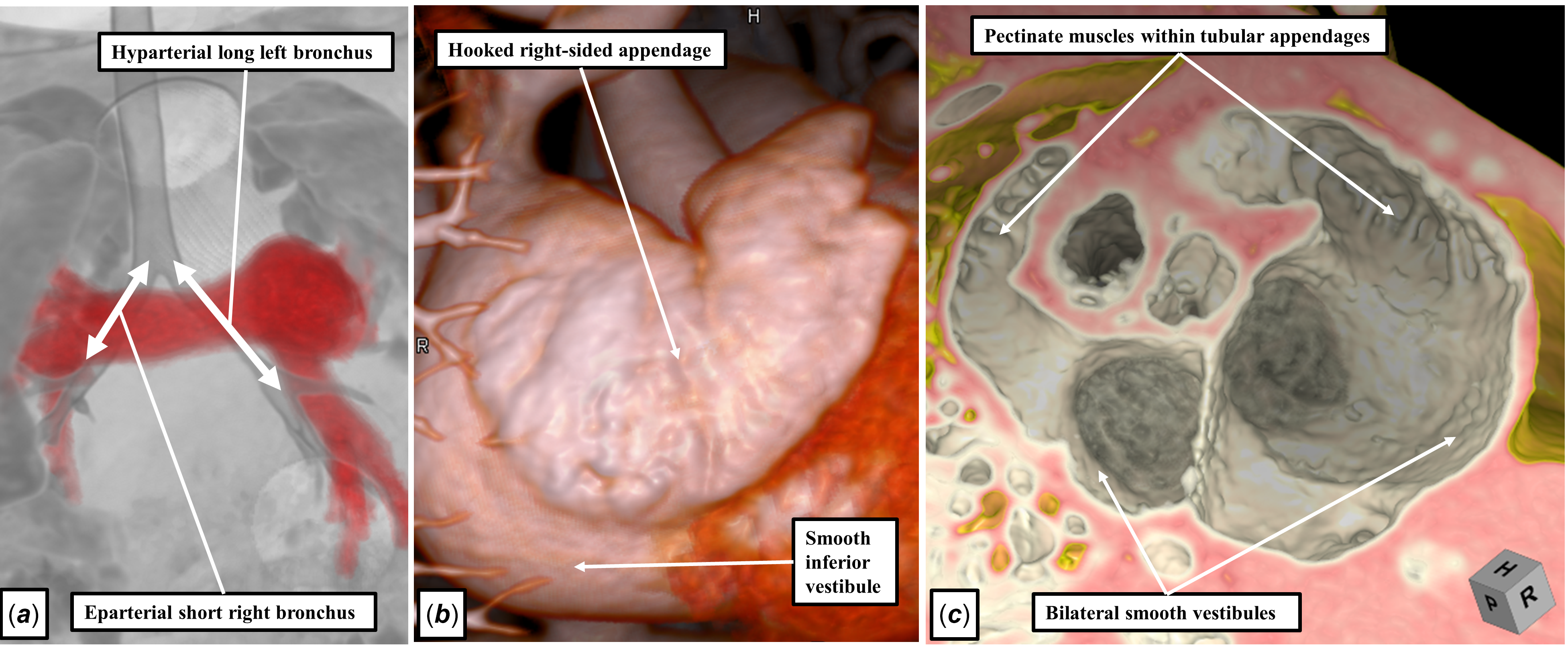
Figure 1. The panels show the morphological features of an individual who, following the criterions suggested by Houyel and her colleagues, would be categorised as being heterotaxic. As shown in (Panel a ), there is usual arrangement of the bronchuses, with the right-sided bronchus being short and eparterial, in contrast to the left-sided bronchus, which is long and hyparterial. (Panel b ) shows the right lateral view of the right-sided appendage, which is tubular and hooked. Analysis of the short axis of the atrioventricular junctions, as shown in (panel c ), shows that the pectinate muscles on both sides are confined within the tubular appendages, indicating the presence of left isomerism. Specificity for further description in this individual is provided by the recognition of the isomeric left atrial appendages. There is no accuracy provided by suggesting that the heart is "heterotaxic.”
It is true that we had presumed, in their own patient, that the appendages had been usually arranged. In their letter, the Parisian authors raise the possibility, on the basis of their shape, that both appendages may have been of right morphology. If this was, indeed, the case, then their experience would truly have been unique. We are unaware of any documented case in which, in the setting of an otherwise normal heart, both appendages have been of either right or left morphology. In their case, had both appendages been triangular, and of right morphology, then a coronary sinus would surely have been lacking in the left atrioventricular junction? They have the option, therefore, of providing more information on the specific cardiac morphology in their patient. In this regard, furthermore, they inferred that we were seeking to deny the possibility that individuals with normal hearts could be found in the setting of the arrangements they group as representing “heterotaxy.” This is not the case. In our commentary, we emphasised that, long since, we had encountered numerous examples of individuals with normal hearts, including usual atrial arrangement, with bronchial and abdominal visceral findings consistent with so-called “heterotaxy.”Reference Anderson, Devine, Anderson, Debich and Zuberbuhler4
In the final analysis, the argument boils down to whether or not we now need the term “heterotaxy” when analysing intracardiac anatomy. The Parisian authors conclude their letter by suggesting that the term provides an “accurate description.” But an accurate description of what? They have emphasised that mirror imagery, when involving the entirety of the body, is now to be excluded by paediatric cardiologists from the category of “heterotaxy.” In this regard, they suggest, incorrectly, that it is our own wish to include mirror imagery within the category. On the contrary, our contention was that, when analysing cardiac morphology, we no longer needed heterotaxy at all! Why would we wish to include mirror imagery within a term we have deemed redundant? All devolves, therefore, on how to categorise the two subsets that the Parisian group, using the definition proposed by the International Nomenclature Committee, would unite to comprise “heterotaxy” within the heart. The question comes down to the purpose of classification. We understand this process to require the grouping together of those entities that have things in common, but separation of those that have obvious differences. Our group has previously demonstrated that bronchial morphology, pulmonary morphology, drainage of the inferior caval vein, the location of the coronary sinus, the morphology of the atrioventricular junctions, the presence of pulmonary atresia, the specific ventriculo-arterial connections, and the position of the aorta and the pulmonary trunk all are statistically significantly different between those individuals exhibiting left as opposed to right isomerism. Many, if not most, of these features are readily discernible to the clinician.Reference Tremblay, Loomba and Frommelt5
Early genetic findings indicate that it is the findings in terms of the atrial appendages, rather than the splenic findings, which are most reproducible using knockout models.Reference Meno, Shimono and Saijoh6,Reference Yoshioka, Meno and Koshiba7 Involvement of specific genes also has been demonstrated, clinically, to be implicated more often in either right or left isomerism.Reference Loomba, Frommelt and Anderson8 Thus, the genetic underpinnings seem to indicate that isomerism, and not heterotaxy, better discriminates the entities by their potential genetic perturbations. It is these genetic cues that seem to be responsible for the production of isomeric as opposed to lateralised features. Thus, it will be essential to keep the two sub-sets apart. As emphasised by the Parisian authors, it will also be necessary to distinguish both sub-sets from complete mirror imagery. We accept, therefore, the contention of Houyel and her colleagues that “the essence of heterotaxy is potential disharmony between the situs of bronchi, abdominal organs, and the atrial appendages.” We submit, nonetheless, that the “accuracy” demanded rightly by the Parisian authors when considering the heart can only be provided by specific description of each of these features. As our new figure shows, these can now readily be discerned in the clinical setting. And, as we also show, description of these cardiac features no longer requires the use of “heterotaxy.” Quod erat demonstrandum.
Acknowledgements
None.
Financial support
None
Conflicts of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.