



On August, 2020, Beirut experienced the largest urban explosion since Hiroshima and Nagasaki when 2750 tons of ammonium nitrate exploded in the Beirut port. 1 This blast resulted in more than 220 deaths, 76 000 injuries, 300 000 people displaced, 19 000 businesses destroyed, 55 non-functional health care facilities, and 15 billion dollars in property damage. 2 Multiple hospitals were severely damaged and made dysfunctional, and the remaining functional hospitals, although also affected, had to accommodate an unprecedented number of injuries at once.
Amidst a squandered and nearly bankrupt country, Hôtel-Dieu de France (HDF), one of the largest university hospitals and tertiary care centers in Beirut, received more than 700 injuries within a few hours of the blast. Health care workers, who had been already shattered financially by the economic crisis that started in 2019 and psychologically by the coronavirus disease (COVID-19) pandemic, suddenly found themselves facing another disaster. This experience is important to share because HDF received the largest number of patients the night of the blast.
This article describes this center’s preparedness for mass casualty incidents (MCIs), its emergency response, and the lessons learned from this tragic event.
HDF Disaster Preparedness
HDF is a 430-bed teaching hospital in Beirut, Lebanon, with approximately 29 000 inpatient hospitalizations and 30 000 emergency department (ED) visits annually. 3 The hospital is capable of providing comprehensive care to trauma patients and is comparable to a Level I adult trauma center as per the trauma center ranking of the American Trauma Society and the American College of Surgeons. 4
At HDF hospital, a committee formed in 2008 was created specifically to work on disaster preparedness. The hospital also has an all-hazards emergency plan, and the medical staff had its first practice drill for an MCI at Hariri airport in 2008. 5 Efficient and stable primary backup communication systems are in place through the in-hospital paging system. The center has access to an updated contact list of all its medical staff. A public information spokesperson has been selected to facilitate communication with the public, the press, and the government health authorities in case of a disaster.
The hospital uses DxCare as its electronic health record (EHR) system, and the ED has a custom-developed version.
HDF’s ED has a Simple Triage and Rapid Treatment (START) mass casualty triage protocol in place that follows internationally approved guidelines. It also has a contingency site for reception and triage of the numerous injuries. Its emergency plan includes the appointment of a hospital security staff and procedures for accurate electronic identification of patients and employees aided by the Lebanese Army at the exit doors. The plan also includes procedures for early control of institution access points, triage sites, and other regions of patient flow, traffic, and parking. The hospital has a system to increase capacity by outsourcing care of non-critical patients to the most appropriate alternative sites. The institution can lead operations at maximum occupancy for 72 hours or more during an MCI.
The hospital has appropriate backup arrangements for essentials including water, electricity, and oxygen, and has stored resources in case of an MCI. In fact, a stock of resources that could last 6 months was in place before the blast.
August 4: the Disaster Response
At 6:08 pm, the ground shook beneath our feet, and after a few seconds, we heard the sound of an explosion.
The blast was so loud that many hospital personnel and patients believed that it originated from inside the hospital. The shockwave was so strong that even HDF, which is located at nearly 1.3 miles from the epicenter, sustained considerable damage. 6 Shattered glass windows flew from all sides and the false ceiling fell, which injured patients and hospital staff. This prompted everyone to hide under the desks and counters in fear of a second explosion, not apprehending what had just happened (Figure 1).

Figure 1. The explosion epicenter with close health care facilities, and Hôtel-Dieu de France located 1.3 miles (2 kilometers) away.
The false ceilings fell in the hallways, patient rooms, the ED, the operating rooms (OR), the intensive care units, and the resident lounge. Many doors were jammed, including the ED entrance door which made circulation inside and outside of the triage room particularly difficult. The main doors were blasted off, with their glass shattered all over the main hall. To add to this, the power went out in many hospital units. We could not get a few minutes to comprehend what had just happened, before bloodstained injured patients started climbing over damaged infrastructure and debris and running into the ED (Figure 2).
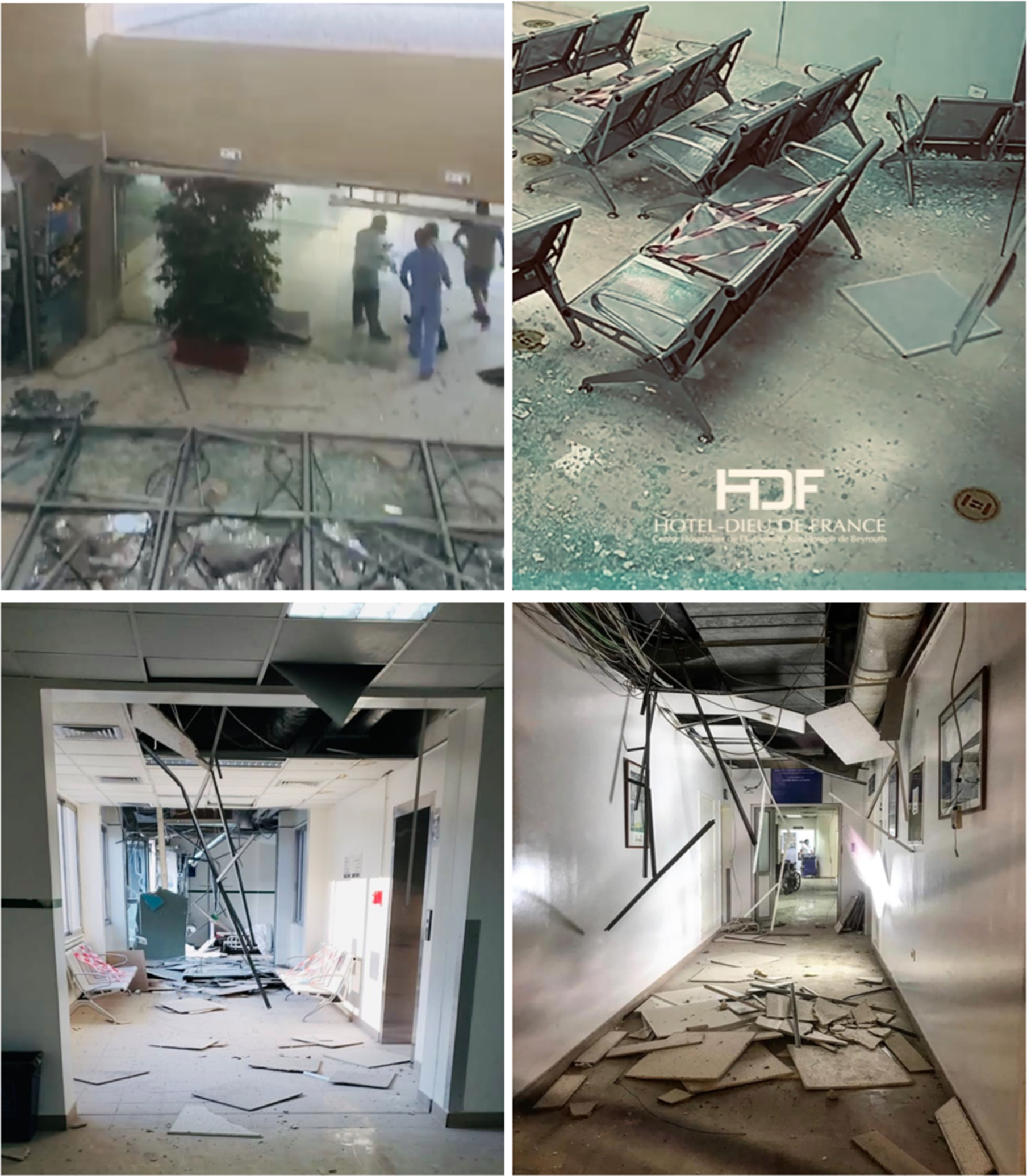
Figure 2. Shattered glass doors at the main entry, damage to the false ceiling, and power cut off.
Activation of the Emergency Protocol
Around 20 minutes after the blast, the hospital disaster plan was activated by the hospital director. By this time, the ED was already filling up with both the patients arriving to the hospital and injured hospital staff. The alert message “mass influx of patients” was sent to each stakeholder on the disaster leadership committee via the hospital paging system.
Each member of the committee quickly assessed the situation in terms of protocols, resources, and the number of personnel needed from their departments, and sent out notifications and alerts to their teams by telephone calls and text messages.
The hospital administration also sent a disaster plan alert to both the hospital and its medical school communication platforms. This meant that every physician, nurse, resident, intern, and medical student had to report for duty and head to the ED. The administrative body, janitors, and maintenance staff also promptly made their way to the ED, ICU, OR, and key floors to help control the situation.
In the ED
When the blast happened, 1 ED physician, 6 nurses, 6 practical nurses, 4 residents, 6 interns, 1 administrative employee, and 4 security agents were present in the ED. However, all health care workers and personnel who were present at the hospital instinctively made their way to the ED to multiply the workforce on the ground in a matter of minutes.
The ED typically accommodates 20 patients in individual rooms, as well as 5 patients in the triage room beds. All previously admitted patients were quickly discharged from the ED or moved to inpatient medical wards.
The first wave of entries were people from the hospital’s neighborhood who mostly came on foot. They had relatively mild injuries and lacerations. An attending and an ED nurse quickly set up a triage area at the ED entry. Anticipating the massive influx of critically ill patients, ED nurses promptly brought all the suturing equipment from the ED storage room and handed out needles, wires, bandages, dressings, gauze, scissors, antiseptics, and anesthetics.
Most of the surgeons and surgical residents were needed in the OR, leaving ED casualties to be primarily managed by nonsurgical physicians and residents who had to suture wounds and lead basic wound explorations with the supervision of the emergency physician due to the limited availability of the surgical personnel.
Medical students were also present on site to help in the transportation of equipment and material from storage rooms to the ED. They also accompanied patients being transferred between the ED, the radiology unit, and the OR, to help in the communication of relevant clinical and radiological findings. For the majority, this was the first encounter with severely injured patients.
At first, wounds were sutured using local anesthetic and sterile techniques. However, the number of patients grew rapidly out of control, and time was a luxury we did not have. The suturing supplies at hand were getting depleted fast, and it was impossible to move around the crowded ED to search or ask for more. The more patients had arrived, the more serious their conditions were, and the less stringent we were with sterilization and aseptic protocols. Some patients were even sutured without anesthesia because there was not any left. Staples were handed out for prompt management of lacerations. In cases of severe bleeding, the bleeding was controlled by packing or dressing the wounds with later delayed suturing. This strategy was crucial to quickly guarantee hemostasis and avoid wound contamination, and also due to lack of local anesthesia. Two nurses went around the ED and put in place intravenous (IV) lines and saline infusions to hypotensive patients who were holding their own IV bags because of a shortage of IV poles. Tetanus shots and other storage were getting depleted. The hospital pharmacy initiated prompt communication with drug suppliers and neighboring pharmacies to replenish their supplies. The hospital staff was too busy providing direct care to the critically injured patients so they used verbal orders for medication, laboratory, and radiology orders. All orders were then added electronically to the hospital EHR system after electronic identification of all admissions was complete. Patient charts were also completed retrospectively because providers evidently prioritized patient care over documentation.
In the first hour following the blast, around 200 wounded patients had already poured into the ED and the numbers kept increasing at an uncontrollable pace. The second wave of patients arrived 2 hours after the blast. Brought in by cars and ambulances, these patients’ conditions were overall more severe. For the first time, this hospital witnessed its doors and ceilings being used as stretchers to transport patients. Those with less severe cases of the second wave reached HDF after walking long distances due to roadblocks and saturated or dysfunctional hospitals in their area.
The hospital security guards struggled to control the ED entrance and hospital access points. Panic, frustration, and anger reigned, and patients’ families became violent and aggressive when asked to stay outside. Many family members were relieved to find their loved ones alive after having searched for them in every other hospital in town. A few hours after the blast, armed forces were mobilized to help and army soldiers arrived and helped control access to the hospital. This loosened the tension and supplied the staff with the energy to continue working until the next morning.
At this point, the ED resembled nothing we had ever seen. All beds were taken. Casualties were lying on the floor, close to each other, with COVID-19 being the least of their concerns. Some of them were unconscious, others were bleeding to the point of exsanguination, drenched in blood, and crying out loud.
Blood was everywhere. It covered the floor, the walls, the ED counters, and our white coats. Patients were being intubated and resuscitated on the floor, sometimes using the same equipment on different patients.

Figure 3. The emergency department, overcrowded with health care workers and patients. ED counters used to accommodate more patients.
Triaging and increasing capacity
As the number of casualties kept increasing, ED counters were being used as substitutes for additional patient beds (Figure 3). An ED physician stood in front of the emergency entrance and was in charge of triaging incoming patients, with the help of residents and nurses. Although HDF follows the START triaging protocol, no space, time, or resources were available to sort patients according to any validated protocol. Instead, the emergency response team opted for a quicker and simpler strategy—dividing patients into 3 categories:
-
(1) Ambulatory injuries were taken care of outside the ED to avoid overcrowding.
-
Head nurses tracked available hospital beds and attempted to free some by temporarily discharging elective patients. Additional beds were added to single-bed rooms to increase capacity. Those with milder injuries who still needed medical attention were sent to the general wards, and residents and interns accompanied them to provide care. The wards were also prepared to receive patients who underwent surgery.
-
Ambulant patients with eye injuries were immediately sent to the ophthalmology clinics for management, and complex lacerations were taken to the minor surgery unit for exploration.
-
The parking lot facing the ED served as a field hospital for patients who did not have life-threatening injuries. They were being cared for on the pavement, and doctors’ vision relied on cell phone lights as it was getting dark.
-
-
(2) Non-ambulatory patients were treated immediately in the ED with a primary survey assessing airway, breathing, circulation, and the presence of immediate life-threatening conditions:
-
Non-ambulatory and non-serious injuries were sent either to the general wards or to the gastrointestinal endoscopy department, which communicates directly with the ED.
-
Non-ambulatory but serious injuries were resuscitated on-site in the ED and sent to the radiology department or the OR immediately. The residents’ primary survey results were written on a paper that was attached to patients’ clothes or given to medical students who accompanied them to their destination. Once patients were safely transferred between the ED, radiology, and the OR, students accompanying them would go back to get more patients. This “one-on-one care” proved to be efficient and was only possible due to the considerable number of health care workers and students who responded to duty.
-
-
(3) The dead-on-arrivals (DOAs): The more these grew in numbers, the harder it was to transfer them to the morgue due to many physical obstacles and the lack of available personnel. They started aligning on stretchers and were transferred to a closed room in the ED. They were transported to the morgue later during the night.
Identification of casualties
Guaranteeing an accurate identification of all casualties was one of the most challenging tasks. Many patients were unconscious and had severe traumatic brain or life-threatening injuries. Some were brought in by strangers who found them lying on the streets, and others by an ambulance. Only a few cases had family members around to help with the identification. Moreover, many casualties were directly intubated or went straight to the OR without prior identification. At peak times, administrators and ED nurses wrapped documentation papers around patients’ clothes and sometimes were even obligated to write on patients’ foreheads their identification information (eg, first name, family name), with the radiologic test requested and its indication (eg, brain CT-scan for head trauma).
A list of all injured patients and DOAs who presented to the ED was carefully recorded by administrators and hospital employees and was constantly updated.
Official electronic registration began retrospectively later during the night, once the ED was a bit less congested. Registration personnel went around all patient care areas and began the identification process. Many patients who only needed basic care and suturing were discharged without thorough registration. At the end of the night, only 2 patients could not be identified because they were unconscious and unaccompanied on arrival. They were registered as “X” and “Y” until we received their appropriate identification on the following day.
It was very challenging to track patient locations as nurses were busy providing direct patient care. This made it impossible for staff to know where patients were being treated and which rooms and areas were available for the next wave of patients.
Distribution of casualties
At least 733 patients signed in to the ED within 12 hours of the blast; 719 injured patients made it through the night, 12 were declared as DOAs, and 2 others were dead within an hour of their admission: 1 from cardiac arrest and the other patient from a severe thoracic blast injury.
Among the injured, a total of 73 underwent surgery; 47 surgeries took place between 6:30 pm and 7:00 am the next morning (noting that 7 patients had to undergo a second revision surgery), while the 33 remaining surgeries were performed later during the next day. The 525 injured patients were treated in the ED, and the other 121 with mild lacerations were treated in the parking lot facing the ED, the endoscopy department, and the general wards (Figure 4).

Figure 4. Diagram showing the distribution of the casualties on August 4.
In addition to the 14 deaths received on that day, 5 patients died on the next day, increasing the total death toll to 19.
In the Operation Rooms
The blast occurred at 6:08 pm, a time when most scheduled surgeries are usually done. On that day, the only surgery that was still ongoing was the repair of a child’s congenital heart malformation. The shockwave did not spare this OR’s false ceiling. Luckily, the scialytic lamps above the surgical site prevented the broken ceiling from going into this child’s cardiothoracic cavity.
Although the ORs did not sustain severe damage other than the disruption of the false ceiling, they were rapidly filled with debris and dust suspended in the air. They needed to be decontaminated and dust-free in a matter of minutes to start receiving the flow of patients. Most of the maintenance staff had already left the hospital and the rest were needed on inpatient floors and at the ED. Fortunately, all staff members who were still in the OR (ie, doctors, nurses, maintenance officers) cooperated to clean the entire department.
An anesthesiologist and surgery nurse gathered all necessary anesthetics from the storage room and filled a big medicine trolley with sufficient quantities of drugs needed for surgeries. The nurse then rounded on all 15 ORs through the night, delivering drugs, and regularly replenishing the trolley.
Every OR accommodated on average a cumulative 3 to 4 surgeries during that night, for a total of 47 surgeries. Some anesthesiologists, surgeons, and residents were asked to go home and rest and come back the next morning, as there were no indicators that the next day would be less tiring. These planned rest periods allowed for the ongoing functioning of the health care team.
As soon as an injured patient went into the OR, the surgeons would evaluate their condition and the extent of vascular, nerve, and bone involvement, as well as measure their blood pressure and pulse rate. They then assessed whether further imaging was needed or whether the patient could directly proceed with the surgery.
Type O blood transfusions were used at the beginning until blood type and crossmatch results were obtained. Social media and news outlets called for blood donors to boost hospital supplies and donors rushed from all over the country. In total, 65 packed red blood cell transfusions, 52 fresh frozen plasma, and 10 platelet units were used that night.
On the night of the blast, life-saving and vital surgeries were prioritized: brain, eye, facial, spinal cord, visceral, and musculoskeletal injuries along with external fixation of fractures. On nights like these, resources are limited and time is crucial. Damage control surgery was the ideal way to stabilize patients and prevent further bleeding and complications.
Fortunately, there was no delay in the surgical management of patients, and surgical tools or anesthetics did not run out. Ever since Lebanon was hit with an unprecedented economic crisis, the hospital expanded most of its supplies to cover 6 months’ worth of medicine, tools, and equipment. On that night alone, 1 month’s worth of supplies was consumed.
With the ICU being at full capacity, the OR recovery room was transformed into an ICU and supplied with more respirators and needed equipment while the surgeries were still ongoing.
On the General Wards
Patients’ rooms facing the explosion’s epicenter were severely damaged. Some patients were ejected from their beds, and the shattered glass was propelled on them. These patients were quickly moved to different rooms and nurses took care of their wounds and lacerations.
After the general wards received the flow of patients from the ED and OR, nurses rounded on all floors to measure vital signs and put in place IV lines when needed. Practical nurses helped clean the patients and replace their bloodstained gowns.
Around 2:00 am, after the new arrivals decreased, physicians who were not needed in the ED rounded with their residents on all floors to obtain a more elaborate medical history, a full examination, and to treat overlooked lacerations and non-sutured wounds. They also prescribed painkillers, antiemetics, antibiotics, and tetanus shots when needed.
Lessons Learned
While hopefully, most medical centers will never face the kind of disaster faced by the staff at HDF, the lessons we learned can be generalizable to similar surge situations and helpful to different EDs while planning for and responding to disasters.
(1) Be Prepared
The key to controlling a crisis remains in a state of permanent preparedness. Being prepared for the worst possibilities, even scenarios that are hard to imagine, can be a game-changer. This starts with a hazard assessment to identify the greatest risks and threats in the country and region. A comprehensive disaster plan can then be created and tailored to those risks and must be able to respond to all possible scenarios. Having this plan is not enough, as it needs to be updated yearly, if not more often. The plan of action should be widely disseminated to all employees concerned and tested through drills and field simulation exercises, in order to have hospital staff fully aware of their roles in responding to a disaster. Realistic drills require investment in time and resources and must be repeated at least every 2 years.
(2) Be Able to Adapt to Different Workforce Capacity
One of the main determinants of the success of our disaster response was the big number of hospital staff that responded to the emergency call. This allowed us to maximize our capacity by having enough staff to cover different hospital locations. Deploying medical students for porterage of the critically injured allowed us to provide one-on-one care when transferring patients between these locations.
Every non-clinical hospital employee has a crucial role, including cleaning staff, suppliers, pharmacists, administrators among others. These important employees must be included in all drills conducted at hospitals.
While a big workforce is extremely advantageous, disaster plans must be flexible to adapt to a smaller staff. For that reason, important roles and functions during disaster scenarios must be clearly explained and accessible on hard copies and on all hospital computers (for example, sorting patients into ambulant, non-ambulant, and dead). That way, any member of staff present on site can try to compensate for personnel shortages that may occur.
Maps to storage rooms, triage protocols, and departments that can be used to increase capacity must be printed as posters and hung in strategic spots across the hospital.
Planned rest periods are important to guarantee the continuity of care during the days following an MCI.
(3) Develop Capacity-Expansion Strategies
Contingency plans and strategies must include an inventory with all available departments, services, and resources that can be used in case of an MCI. Additional allocated areas must be well-equipped and ready to be promptly transformed into areas capable of accommodating injured patients. In our case, re-deploying the gastrointestinal endoscopy unit as an acute care center allowed us to significantly increase our capacity.
(4) Triage Outside the ED
Triage must be done in a large area outside the ED to avoid overcrowding it with non-urgent injuries. Mild ambulant injuries should be directly transferred to the designated areas. These areas must be near the ED so transfers can be easy and fast. It is necessary to have standardized identification sheets where one can register diagnosis, care, radiological assessment, examinations, and operation with the color code of the START protocol. These sheets should be printed and stored in sufficient quantities in the emergency admission office, ready for use. They can ideally be hung on the patient’s neck.
ED entry points and other hospital access areas must be immediately secured by security officers. Hospitals cannot rely on the help of external police or military forces in the first hours. Security officers should be trained to control hazardous areas, secure the vicinity of the hospital, and secure main doors until external help can get there.
(5) Prepare Alternatives for Failed Electronic Records
In case regular patient registration and identification processes are disrupted, develop the simplest forms of identification, including writing on pieces of paper, on bracelets, or on patient beds.
An ideal method would be to use identification bracelets with pre-established Personal Identification Numbers (PINs) with the START color code. These bracelets should also be already printed and stored.
If providers are unable to adhere to electronic charting, orders, and documentation, which is probable in the case of an MCI, unsophisticated paper-based MCI tools must be developed, and verbal orders must be used so the ED workflow is not halted.
Hospital registration staff should be designated to oversee electronic registration whenever it becomes possible, by going around the ER and entering the PINs with patients’ names on the hospital EHR system. Unidentified patients can be registered using their PINs and an assigned temporary letter (A-Z).
(6) Maintain Solid Communication Within the Team
Comprehensive communication plans between administrators and the main actors during MCI should be established via efficient and robust technology as an alternative communication system in case the routine communication channels are hampered.
Keeping a record of voice calls is important for post-incident investigations and for improvement.
A common group of communication should gather physicians and nurses from the ED, the radiology department, and the OR on which the patient’s history, clinical exam, vital signs, and imaging results are shared before sending them to the OR.
Conclusion
August 4 will remain engraved in the memories of every Lebanese, especially frontline health care staff who witnessed the heart-wrenching consequences of such a tragedy. This night taught us many lessons and led most Lebanese hospitals to improve their emergency plans and preparedness for future disasters.
At HDF, drills and simulations should be conducted more frequently, which will require investment in time and resources. Along with the large number of medical respondents, one of the main determinants of that night’s success was the leadership’s flexibility and capacity to adapt.
It is said that Beirut was buried to the ground and rebuilt 7 times. It has certainly witnessed a lot of destruction over the past 50 years, leading to financial losses, damage to infrastructure, and mostly human loss. The Beirut blast destroyed much of what has remained. Yet what has not been destroyed is the resilience of its people, a trait particularly needed as the fragilized country attempts to recover.
Author contributions
All authors listed have significantly contributed to the investigation, development, drafting of the article, revising it critically for important intellectual content, and the final approval of the version to be submitted. Authors AK, SFH, MZ, TS contributed equally to this work.
Conflict(s) of interest
The authors declare they have no conflicts of interest.




