


INTRODUCTION
The common bed bug, Cimex lectularius L. (Order: Insecta, Class: Hemiptera) has been a known human pest for thousands of years, with records dating back to ancient Egypt [1]. Bed bugs are haematophagous arthropods of the family Cimicidae within the order Hemiptera. Of the 90 or so species within the family Cimicidae, only a handful bite humans, with the two main species being the common bed bug, C. lectularius, and the tropical bed bug, C. hemipterus F. Unlike C. lectularius, C. hemipterus is the most dominant species in tropical and subtropical regions including India [1].
Although bed bugs have a long association with humans, for a period from the 1950s to almost the start of the 21st century, this pest had become relatively uncommon, particularly in the more economically advantaged nations [Reference Doggett2]. However, in recent years resurgence of bed bug infestations has been reported in Germany, USA, Canada, Italy, Australia, Europe, Africa and Asia [Reference Doggett2]. Pesticide resistance, especially to the pyrethroids, has been promulgated as the key trigger with a myriad of other factors including frequent travel, lack of public awareness, inadequate pest control programmes all contributing to this resurgence [Reference Doggett2–Reference Criado4]. Bed bug infestations are often more frequent in sites of transient populations such as hotels, dormitories, cruise ships, trains, homeless shelters and hospitals [Reference Fallen and Gooderham5].
Bed bugs are impinging upon human health in multiple ways as the insect is increasingly becoming a societal pest. In the following report we present our experience with an infestation of the tropical bed bug in our neonatal unit with the aim of increasing the awareness of physicians regarding the entomology, diagnosis and management of bed bug infestations.
METHODS
The Department of Neonatology is an 80-bed regional neonatal intensive care unit attached to the state-run Lady Hardinge Medical College, New Delhi. It caters primarily to populations from low or low-middle socioeconomic strata. Most of the population lives in small houses with overcrowding and compromised hygiene.
Attached to the neonatal unit is a step-down room where the babies are kept with their mothers for weight gain and/or completion of antibiotic treatment. Average stay of these babies is usually about 2–3 weeks.
Delhi has cool weather during winter (December–January) with an average temperature of around 4–6 °C. Mothers hospitalized in the step-down unit sometimes bring their own blankets to keep warm.
On 14 December 2013, one mother admitted to the unit complained that her baby was not able to sleep during the night. Her baby, a preterm, was transferred to her 2 days earlier and was being kept in the neonatal unit for weight gain. The mother also mentioned that she had developed itchy papular eruptions on her arms. Simultaneously, another of the mothers was also observed by the staff to have similar eruptions. A postgraduate resident posted in the unit also developed an itchy papular rash on her right leg. A mother who had previously experienced a bed bug infestation commented that she had seen bed bugs during the night. The entire unit was thoroughly inspected for bed bugs. Evidence of an infestation was found in crevices in the wall and two baby mattresses. Live bugs were also detected and latter identified as the tropical bed bug (Fig. 1) (see Supplementary online video).

Fig. 1. Tropical bed bug Cimex hemipterus, an adult female.
The following week out of a total of 15 mother–infant pairs admitted in the unit, two mothers and nine mother–infant pairs were attacked by bed bugs. A total of 39 individuals were affected in this outbreak. A detailed epidemic curve was prepared and analysed (Fig. 2). It was established that the infestation was due to a point-source outbreak with limited spread. The infestation had probably originated from one mother admitted on 10 December 2013. The blanket she had brought from her home was later observed to be heavily infested. From her, bed bugs spread to involve the adjacent mothers and mother–infant pairs. Eleven family members of three of these mothers were subsequently affected as a result of transferring bed bugs from the neonatal unit to their own home, presumably via clothing and other belongings. One of the three resident doctors (all three had bed bug bites) posted in the unit transferred the bed bugs to her home resulting in bites to all five of her family members. The clinical features of the affected persons have been summarized in Table 1. Newborns primarily experienced an inability to sleep due to bed bug bites. Papular rash and itching were the most common manifestations in adults. All affected individuals responded to symptomatic treatment consisting of emollient cream and antihistamine. Only two mothers and one family member required antibiotics for control of folliculitis.
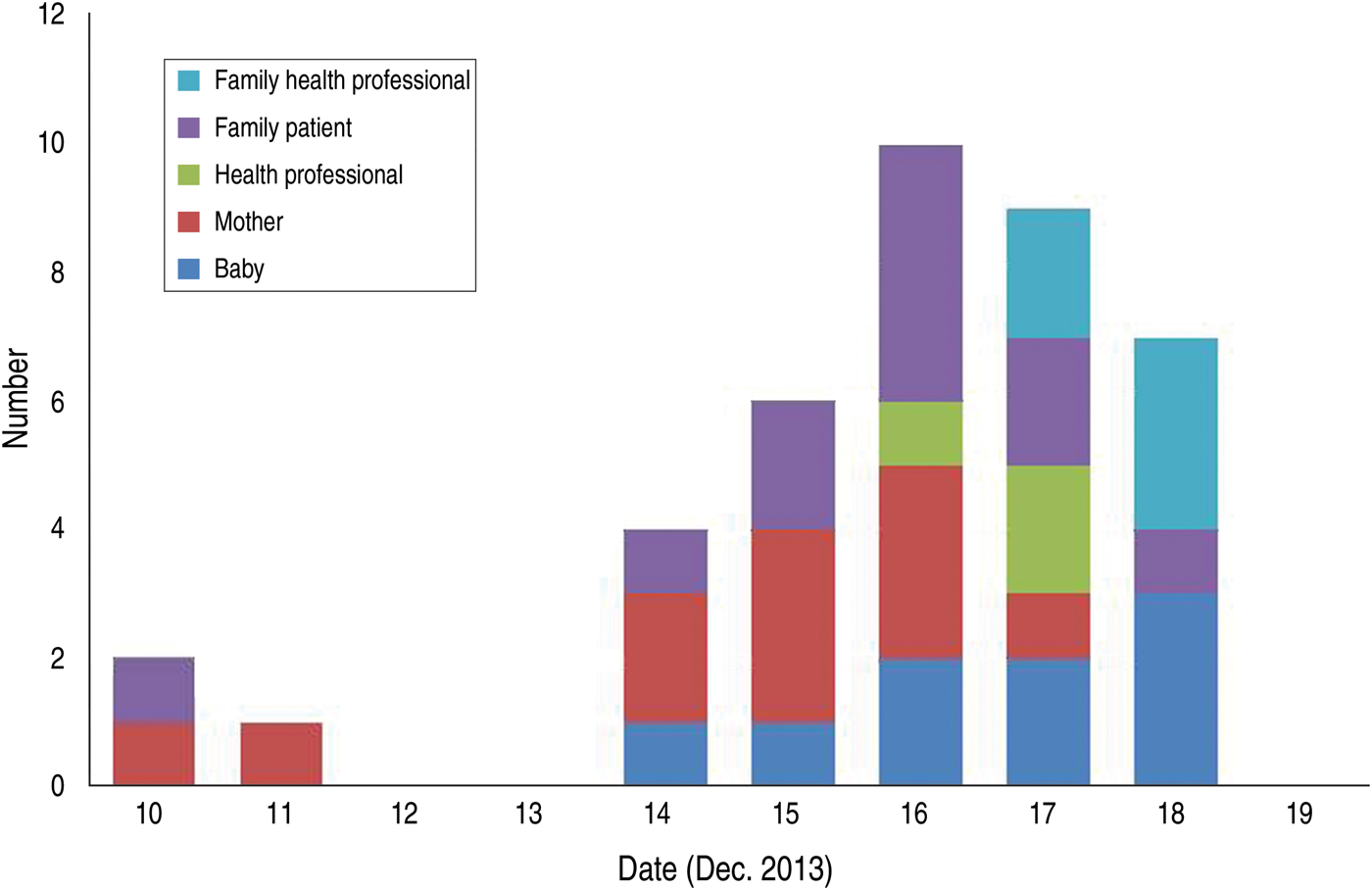
Fig. 2. Epi curve of the persons involved.
Table 1. Clinical features of affected individuals
The infested part of the unit was temporarily closed for disinfection purposes. Mothers and babies were relocated to another care area. Before moving, the patients were requested to seal into double plastic bags all their clothes, bed sheets, and personal belongings and take all these items home. They were advised to launder their clothes in hot water and iron them. Blankets and quilts were recommended to be sent to a dry cleaner. They were also given advice to inform their dry cleaner about the likelihood of these items being infested with bed bugs. All the crevices in the neonatal unit walls were sealed with plaster of Paris and the room repainted. An insecticide combination consisting of d-phenothrin, N-octyl bicycloheptene dicarboximide and imidacloprid (Bedlam Plus®, MGK, USA) was sprayed twice at an interval of 1 week. All the baby mattresses in the infested room were discarded. Baby cots were also disinfected and repainted. The health professional team posted in the unit was educated about the precautions required to avoid bed bug transmission.
This part of the unit remained closed for 2 weeks and was declared bug free in the last week of December 2013 and made operational. Since then regular inspections by bed bug pest managers in the next 1, 2 and 6 months did not reveal any recurrence.
DISCUSSION
There has been underreporting of bed bug infestations within healthcare facilities as evidenced by the scant medical literature available. This might be explained by the negative publicity reports of bed bug infestations are likely to generate [Reference Munoz-Price6]. On the other hand the lay press is full of reports of bed bugs in healthcare facilities. For example, bed bugs led to the refusal of medical treatment for a woman in Aurora, Colorado, the shutting down of an entire treatment floor in a New York medical facility, the partial closure of a hospital for 2 weeks in Kerry, Ireland and closure of a whole wing of an adolescent ward of a major Sydney hospital in Australia [Reference Doggett2]. In parts of the USA, the presence of even one bed bug in an intensive care unit will result in the unit being taken out of service for pest treatment [Reference Leininger-Hogan7].
To date, we are unaware of any published report detailing bed bug infestations in a neonatal unit, although in light of reports from a variety of other medical facilities, infestations in sites such as ours could, perhaps, almost be expected. This is the first report on an infestation involving the tropical bed bug in a clinical setting. In our neonatal unit, once the bed bugs were introduced, the social background of the mothers, their living conditions at home along with their lengthy hospital stay, presumably contributed to the degree of the bed bug infestation and its subsequent spread. One marked aspect brought out by this episode was that most of our health professionals including residents and consultants had not seen a bed bug and had many misconceptions regarding their clinical significance, spread and control. This observation follows that of similar reports on the lack of knowledge of bed bugs in the wider community. For example, in a study from Germany only 13% of the respondents could recognize a bed bug and only 15% correctly said that they would call a pest controller in case of a bed bug infestation. It was estimated that 97% of all early stage infestations would go untreated [Reference Seidel and Reinhardt8].
Bed bugs are very difficult to eradicate. It is important to understand their biology and how they spread in order to implement effective control measures.
Entomology
Bed bugs are oval, flat, and wingless. They are obligate blood parasites. Juvenile bed bugs in the first instar are around 1 mm in length and cream in colour. The insect has five juvenile stages (or instars) and becomes deeper in colour with each moult. Adults are reddish brown and typically 4–7 mm in length when not blood engorged. Adult females produce 50–200 eggs in a typical 4–6 month lifespan [Reference Doggett2, Reference How and Lee9]. To avoid light, bed bugs hide in the seams of mattresses and crevices of bed frames, walls, and furniture during the day [Reference Reinhardt and Siva-Jothy10]. They are attracted to human host by body odours, warmth and carbon dioxide [Reference Doggett2, Reference Goddard and deShazo3]. Peak feeding usually takes place just before dawn. Bed bug saliva contains several vasodilatory, anticoagulant, and proteolytic compounds, which ensures the blood does not clot while the insect feeds [Reference Francischetti11]. Some of these compounds are known to have antigenic properties in humans, which results in the allergic skin reactions [Reference Doggett2].
Clinical implications
Not all bed bug bites result in a dermatological reaction in humans. Reinhardt and colleagues reviewed the literature on human reactions to bed bug bites, and when data from all the studies were combined, 249 (75%) out of 331 patients were found to develop a reaction [Reference Reinhardt12]. Vesicles, bullae, and nodules have all been reported [Reference Cohen13]. A typical wheal-type lesion is a 2–6 cm, pruritic, erythematous maculopapule with a central haemorrhagic crust [Reference Goddard and deShazo3]. Bites are preferentially distributed in unclothed areas (e.g. face, neck, extremities) and classically are in a row or cluster, due to a number of bed bugs feeding over an area [Reference Doggett2, Reference Cohen13]. Scratching can cause impetigo, cellulitis, or folliculitis. Systemic reactions have been described, including asthma, generalized urticaria, angioedema, iron deficiency anaemia, and, very rarely, anaphylaxis [Reference Studdiford14]. Bed bugs can also affect the mental health of those bitten by the insect [Reference Doggett2].
Disease transmission
Bed bugs can be carriers of more than 40 different species of microorganisms in their stomach, faeces, tegument, and/or saliva. However, to date, there is no firm evidence to suggest that either C. lectularius or C. hemipterus is a competent vector of any pathogen [Reference Doggett2, Reference Delaunay15].
Economic impact
Bed bug infestation can result in significant economic consequences. The cost arises from payments for pest control, replacement of infested furniture, loss of productivity, adverse publicity and damage to reputation [Reference Davies, Field and Williamson16].
Diagnosis
The diagnosis of a bed bug infestation is suspected on the clinical history and appearance of bites but can only definitely be made on identification of the insect. A thorough inspection of sleeping quarters by a pest control expert may lead to the identification of live insects, or specks of blood-tinged insect faeces and exoskeleton casts [Reference Studdiford14]. Special attention should be given to cracks and crevices of furniture, electrical boxes, curtains, carpets, luggage, bed frames and headboards, picture frames, wall hangings, mattress and box spring seams, peeling wall paper, clothes, and linens [Reference Studdiford14]. Visual inspections, although not so expensive in India, are time consuming and unreliable when only a few bugs are present. Use of specially trained dogs in bed bug recognition has been available for many years particularly in the USA, but this is expensive and may unintentionally advertise a bed bug problem if seen by others, such as guests in hotels. New technologies for bed bug detection using DNA analysis, mass spectrometry, and electronic noses are innovative but often impractical, expensive and usually not very effective [Reference Vaidyanathan and Feldlaufer17].
Treatment of bites
Bed bug bite reactions are self-limiting and usually resolve in 1–2 weeks [Reference Cleary and Buchanan18]. Antipruritic preparations containing intermediate potency corticosteroids may be beneficial. Mupirocin and/or systemic antibiotics should be considered in the treatment of infected bites [Reference Goddard and deShazo3].
Bed bug control
Consultation with a professional pest control expert specifically trained in bed bug management practices is necessary. A multifaceted approach consisting of: proper identification of the bed bug species, education of the stakeholders involved, thorough inspection of infested and adjacent areas, and the implementation of chemical and non-chemical control measures, is required for pest elimination to be successful [Reference Goddard and deShazo3]. There are several chemical classes of pesticides that are currently registered in various parts of the world, including India, which are used for bed bug control: pyrethrins, pyrethroids, carbamates, organophosphates, desiccants, arylpyrroles, neonicotinoids, and insect growth regulators. Each chemical class with the exception of pyrethrins and pyrethroids, kills bed bugs via a different mode of action. It can be helpful to use pesticides that differ in their mode of action because it can reduce the likelihood that the bugs will develop further resistance or resistance to other insecticide classes [19, Reference Doggett20].
Protocol for health facilities
Each facility should have protocols in place in case a bed bug infestation is detected. A protocol similar to one published previously may be followed (see e.g. [Reference Munoz-Price6, 21]).
CONCLUSIONS
Bed bugs have re-emerged during the past two decades throughout the world. They can be very challenging to detect and difficult to eliminate. A multifaceted approach is generally needed to eradicate infestations. Bed bugs not only cause disruption of medical services, but their presence cause undue psychological stress on those affected and poses a considerable economic burden. There is a need to educate health professionals on how to identify and respond to bed bug infestation. It is impossible to prevent bed bugs; however, strategies can be implemented to minimize their impact, particularly by having protocols in place in case bed bugs are detected.
SUPPLEMENTARY MATERIAL
For supplementary material accompanying this paper visit http://dx.doi.org/10.1017/S0950268814003690.
DECLARATION OF INTEREST
None.




