



Systemic lupus erythematosus is a chronic autoimmune disease characterised by inflammation that affects tissues in various organ systems, including the cardiovascular system. Reference Charras, Smith and Hedrich1 Cardiovascular involvement occurs in 30−40% of children with systemic lupus erythematosus with most cardiovascular involvement occurring at > 8 years. Reference Park and Salamat2 Systemic lupus erythematosus in children has more severe clinical manifestations. Reference Weiss3 Cardiac involvement often does not show specific clinical signs and symptoms. Previous studies have demonstrated myocardial dysfunction and left ventricular remodelling in systemic lupus erythematosus patients, even with a normal ejection fraction with damage to the myocardium linked to disease severity. Reference Deng, Xie, Lv, Li, Fang and Wang4
The results are consistent with the previous research on children with systemic lupus erythematosus, and left ventricular systolic dysfunction can be detected using speckle-tracking echocardiography even though it is not detected on conventional echocardiography. In addition, the speckle-tracking echocardiography strain was also found to be significantly lower in the group with more severe disease activity. Reference Dedeoglu, Şahin and Koka5 Other research has suggested that the duration and activity of systemic lupus erythematosus disease have a significant relationship to parameters of left ventricular diastolic function, as well as to left ventricular mass and pulmonary arterial pressure. Reference Mirfeizi, Poorzand, Javanbakht and Khajedaluee6
Many instruments for assessing the severity of disease activity in systemic lupus erythematosus have been developed. The Mexican Version of the Systemic Lupus Erythematosus Disease Activity Index (MEX-SLEDAI) was developed by Mexican researchers to reduce the costs required for laboratory tests required for the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). Reference Uribe, Vilá, Jr, Sanchez, Reveille and Alarcon7 A non-invasive method is needed to detect early cardiac involvement in systemic lupus erythematosus. Speckle-tracking echocardiography detects ventricular dysfunction by assessing myocardial deformation and has been reported to detect left ventricular dysfunction in adults and children with systemic lupus erythematosus. Left ventricular dysfunction is also consistent with the severity of disease activity in systemic lupus erythematosus. Reference Deng, Xie, Lv, Li, Fang and Wang4,Reference Dedeoglu, Şahin and Koka5,Reference Taha, Labib, Baghdady, El-Ghobashy and Elamragy8
Material and methods
This cross-sectional study was conducted at the Dr Hasan Sadikin General Hospital, Child Health Department in Bandung, West Java, Indonesia, from May 2023 to June 2023. Children who were diagnosed with systemic lupus erythematosus in the age range of 5 to 18 years and who are being treated at outpatient and inpatient departments and underwent physical and laboratory examinations to assess disease severity using MEX-SLEDAI were included in the study. Patients diagnosed with CHD, severe valvular heart disorder, any syndrome like Down syndrome, congenital rubella syndrome, arrhythmia, massive pericardial effusion, infection like sepsis and pneumonia, oxygen saturation < 95%, haemoglobin < 7 mg/dl, massive oedema, or poor echo window were excluded. The participants were chosen using a purposive sampling method.
The primary subject data recorded were gender, age, nutritional status measured with body mass index for age using WHO growth reference 2007, 9 blood pressure, pulse rate, oxygen saturation, duration of the disease, any cardiac manifestation, and organ manifested in systemic lupus erythematosus. These data are acquired by history taking, physical examination, medical records, and echocardiography results. The disease severity was determined using the MEX-SLEDAI, with a score of 2−5 as mild, 6–9 as moderate, and ≥10 as severe.
Each subject underwent conventional echocardiography and speckle-tracking echocardiography with a Philips EPIQ machine performed by a Pediatric Cardiologist Consultant 10 days after inclusion. Conventional echocardiographic data measured by M-mode were ejection fraction, fractional shortening, E/A ratio, and speckle-tracking echocardiography by taking apical views, namely apical four chambers, two chambers, and three chambers, and producing global longitudinal strain values. Reference Levy, Sanchez, Machefsky, Fowler, Holland and Singh10 Data analysis was performed using the Statistical Package for Social Sciences (SPSS) for Windows 25.0. A p-value of ≤0.05 was considered statistically significant.
Results
Fifty-four children met the inclusion criteria and underwent echocardiography, but five subjects were excluded due to a poor echo window, so the data of 49 subjects were included in the final analysis. Poor echo window means that good-quality images were not obtained due to some subjects being obese or having a history of pulmonary tuberculosis. Table 1 shows participants’s characteristic. The participants comprised 15 (30.6%) subjects with mild disease activity and 34 (69.4%) subjects with moderate disease activity. Mild-to-moderate valve abnormalities were found in four (8.16%) subjects and mild pericardial effusion in four (8.16%) subjects. In addition, organ system involvement consisted of kidney involvement in 37 (75.5%) subjects, followed by haematological involvement in 24 (48.9%), musculoskeletal and mucocutaneous each 19 (38.7%), and neuropsychiatric in 4 (8.1%) subjects.
Most patients were 40 (81.6%) female with a median age of 15 years. The nutritional status was adequate, both in the mild and moderate disease activity groups, and was not significantly different. Likewise, there were no significant differences in the mean pulse rate, median systolic, diastolic blood pressure, and median duration of systemic lupus erythematosus disease between the two groups.
Conventional echocardiography revealed that the average ejection fraction, fractional shortening, and median ratio E/A were still within the normal range in both the mild and moderate disease activity groups. The mean global longitudinal strain in the mild and moderate activity group were −19.65 and −16.58, respectively. The statistical analysis showed no significant difference in the mean between the ejection fraction, fractional shortening, and E/A ratio variables in the mild and moderate systemic lupus erythematosus activity groups (p > 0.05). In addition, the average global longitudinal strain was significantly different in the moderate and mild disease activity groups (p = 0.008). Table 2 shows parameter echocardiography results based on the severity of SLE activity.
Discussion
Most systemic lupus erythematosus patients in this study were female with a median age of 15 years (range 6 − 17 years), which is in line with the research by Hasan et al showing that the incidence of systemic lupus erythematosus in children is more common in females (91.3%) than males (8.7%), with an age range of 8−16 years. Reference Hassan Elsayed Hassan11 These data are in accordance with the study of Evalina et al who reported that 91.7% of paediatric systemic lupus erythematosus patients treated at the Adam Malik General Hospital in Medan were female. This may be related to the female hormones oestrogen and prolactin which can induce autoimmunity that occurs in systemic lupus erythematosus. Reference Evalina12
In the present study, most subjects had a normal nutritional status with no significant differences between the two groups. The systemic lupus erythematosus duration ranged from 1 to 96 months with a median of 12 months and no significant difference in duration between the two groups. This shows the long duration experienced by patients with systemic lupus erythematosus (up to 8 years). Tselios et al reported that of 267 systemic lupus erythematosus patients, 10.1% experienced remission within 5 years and maintained their remission condition for ≥ 10 years (prolonged remission), 67.4% of patients experienced relapsing–remitting periods, and 9.4% experienced persistent active disease. Reference Tselios, Gladman, Touma, Su, Anderson and Urowitz13
In the present study, 15 (30.6%) subjects had mild disease activity and 34 (69.4%) had moderate disease activity with no subjects with severe disease activity. The MEX-SLEDAI score range in this research is 2−9 because most subjects were systemic lupus erythematosus patients treated in the outpatient department, and some of the exclusion criteria used can affect left ventricular function such as severe valvular heart disorders, massive pericardial effusion, massive oedema, and severe anaemia that may occur in systemic lupus erythematosus patients with severe disease activity.
All subjects in this research have more than one organ involvement. Kidney involvement was the most common organ manifestation in this study (75.5%), followed by haematological involvement (48.9%), musculoskeletal (38.7%), mucocutaneous (38.7%), and neuropsychiatric (8.1%). Systemic lupus erythematosus onset in children is generally sudden and has a more aggressive course than in adults, affecting major organs such as the kidneys, brain, and blood. In addition, systemic lupus erythematosus in children has more severe disease activity than adults. Ping Tang et al stated that systemic lupus erythematosus in Southeast Asia has similar characteristics to the results of cohorts of children with systemic lupus erythematosus worldwide but has unique characteristics, including higher disease activity and a predominance of kidney disorders. Mortality varies in several countries but is influenced by heterogeneity in access to health services and socio-economic status in each region. Reference Tang, Lim and Arkachaisri14
In this study, mild–moderate valve abnormalities were found in the form of mitral valve insufficiency in four (8.16%) subjects and mild pericardial effusion in four (8.16%) subjects, where valve abnormalities and pericardial effusion occurred in all patients with moderate disease activity. This result is in line with research by Chang et al who reported that 18% of 699 subjects with systemic lupus erythematosus who had disease onset in childhood experienced cardiac manifestations, with most abnormalities being valvular insufficiency and pericarditis at the time of diagnosis. Reference Chang, Knight, Xiao, Mercer-Rosa and Weiss15
Until now, the use of conventional echocardiography for the assessment of left ventricular function is routine in daily practice. From the present study results, it can be concluded that the average left ventricular function of the study subjects was normal when measured by conventional echocardiography (ejection fraction, fractional shortening, and E/A ratio). This research also shows that the average global longitudinal strain value in the mild activity group was −19.65%, and in the moderate activity group was −16.58%. Until now, there has been no global agreement on the optimal cut-off value of global longitudinal strain in children with systemic lupus erythematosus. A systematic review and meta-analysis by Levy et al identified 2,325 children from 43 research data, defining the mean global longitudinal strain reference value in healthy children as −20.2%. Reference Levy, Sanchez, Machefsky, Fowler, Holland and Singh10 The average global longitudinal strain value in this study was abnormal (<20.2%) in both mild and moderate groups, with statistical analysis showing a significant difference.
These data are in accordance with research by Agha et al, where ejection fraction, fractional shortening, mitral annular plane systolic excursion, and global longitudinal strain were assessed in 26 children with systemic lupus erythematosus and 21 healthy patients as controls. The LV dimensions and systolic function (including ejection fraction) assessed by M-mode (conventional echocardiography) in both groups were normal, with no significant difference. In contrast, global longitudinal strain in systemic lupus erythematosus patients was significantly reduced compared to controls. This result could suggest that M-mode is a rapid screening modality, but that subclinical ventricular dysfunction may go undiagnosed. The severity of systemic lupus erythematosus activity is considered a predictor of subclinical dysfunction in the left ventricle. Agha et al found that a SLEDAI score > 6 was associated with a global longitudinal strain < −14 in 34% of patients. Reference Agha, Othman and El-Saiedi16
This result is also in line with the study by Mohammed et al who aimed to use echocardiography to identify cardiac dysfunction in asymptomatic systemic lupus erythematosus patients. In this study, of 50 adult patients with systemic lupus erythematosus, only 8 patients had ventricular systolic dysfunction and 4 patients had ventricular diastolic dysfunction based on conventional echocardiographic assessment. Reference Mohammed, Alghamdi, ALjahlan and AL-Homood17
Dedeoglu et al performed speckle-tracking echocardiography on 35 children with systemic lupus erythematosus and 30 healthy children and assessed disease severity using SLEDAI. Overall, global longitudinal strain values were reduced in children with systemic lupus erythematosus compared to controls. Patients were then divided into two groups and underwent a follow-up speckle-tracking echocardiography examination after therapy, showing that patients with SLEDAI scores who did not improve (score still > 4) had decreased global longitudinal strain results compared to patients who experienced improvement. Reference Dedeoglu, Şahin and Koka5 Deng et al divided adult systemic lupus erythematosus patients into groups based on the SLEDAI score. On speckle-tracking echocardiography examination, global longitudinal strain results were significantly reduced in patients with systemic lupus erythematosus, even with normal ejection fraction. In addition, the global longitudinal strain obtained in the group with the more excellent SLEDAI score had significantly more severely impaired ventricular function. Reference Deng, Xie, Lv, Li, Fang and Wang4
The limitation of this study is the research design which was a cross-sectional analytic observational study, so it was only performed at onetime point without follow-up of disease activity and cardiac function that may change over time. Some subjects have mild-to-moderate valvular disorder and mild pericardial effusion, conditions that may also affect left ventricular function. There was also lack of data on previous heart conditions and the systemic lupus erythematosus treatment that will influence LV systolic function. This study conducted at one single centre, which could lead to low external validity. Although Dr Hasan Sadikin General Hospital is a referral centre for systemic lupus erythematosus in children in West Java, the results of this study may differ from other regions in Indonesia. Further research is needed to assess left ventricular function using speckle-tracking echocardiography with a prospective cohort study design in multiple centres and to consider the effect of disease duration and systemic lupus erythematosus treatment.
All children with systemic lupus erythematosus should have routine echocardiography for every year and the global longitudinal strain included in addition to left ventricular ejection fraction measurement. In conclusion, left ventricular function, as measured by systemic lupus erythematosus, is lower in children with moderate systemic lupus erythematosus activity than in those with mild disease activity.
Table 1. Participants’ characteristics based on the severity of SLE activity.
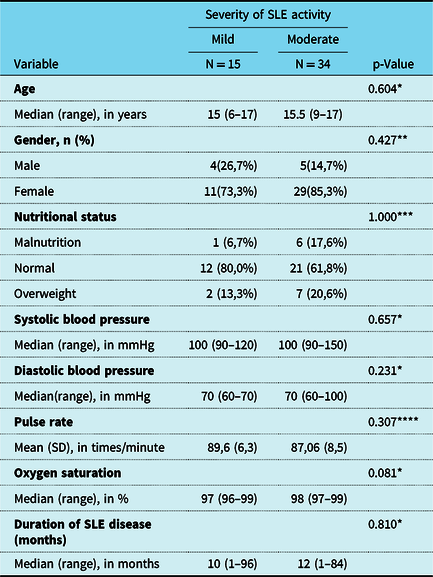
SD = standard deviation; SLE = systemic lupus erythematosus.
* Based on Mann–Whitney test.
** Based on Fisher’s exact test.
*** Based on Kolmogorov–Smirnov test.
**** Based on unpaired t-test.
Table 2. Parameter echocardiography results based on the severity of SLE activity.
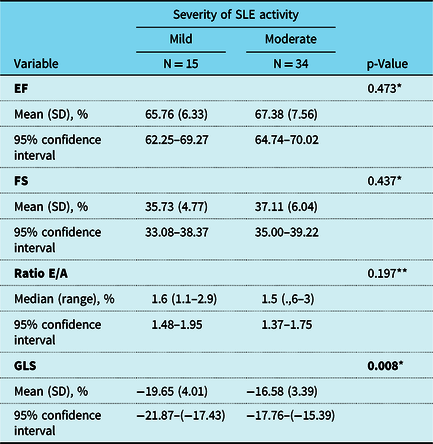
EF = ejection fraction; FS = fractional shortening; GLS = global longitudinal strain; SD = standard deviation.
* Based on unpaired t-test.
** Based on Mann–Whitney test.
Acknowledgements
The author would like to thank Dr Hasan Sadikin General Hospital Bandung as the location of the research study and also to Dr Putria Rayani as staff at Division of Cardiology, Department of Child Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional committees of Dr Hasan Sadikin General Hospital Bandung.



 Open access
Open access