



Introduction
The term ‘microaggression’ was coined in 1970 to describe subtle dismissals and insults towards Black Americans (Pierce, Reference Pierce1970). The word remained largely in obscurity until the late 2000s, when a paper exploring ‘subtle and contemporary’ forms of racism in the context of therapy gained widespread public attention (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007). Based on the analysis of personal narratives and the social and counselling psychology literature, Sue et al. defined microaggressions as ‘brief and commonplace daily verbal, behavioural or environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative racial slights and insults towards people of color’ (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007, p. 271). They describe three distinct forms of microaggressions: microassault, microinsult and microinvalidation. A microassault is the most overt form, for example, intentionally calling a person of colour a derogatory term. Microinsults are more subtle and convey rudeness or insensitivity, for example, clutching one's purse more tightly when in the presence of a person of colour. Finally, microinvalidations negate or nullify the feelings or experiences of a person, by saying, for example, ‘Don't be so oversensitive’ (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007, p. 275).
The concept of subtle, contemporary forms of racism has captured the attention of wide audiences, not least because these researchers argue that microaggressions have a powerful, negative cumulative effect on the mental health of people of colour (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007; Sue, Reference Sue2010). The theoretical basis of this assertion is grounded in ‘minority stress theory’ (Meyer, Reference Meyer1995) which states that a hostile social environment demands heightened vigilance to protect oneself from discrimination and violence. It is also argued that the subtle nature of microaggressions creates a ‘catch-22’ (or ‘no win’) situation, in which an individual is left questioning the validity of his or her experience (‘Did what I think happened, really happen?’). This concept has been described as attributional ambiguity in the wider stigma literature and is argued to pose a particular threat to self-esteem and lead to suspicion and mistrust (Crocker et al., Reference Crocker, Major, Steele, Gilbert, Fiske and Lindzey1998).
Numerous studies have reported a significant correlation between reported experiences of microaggressions and self-reported negative mental health outcomes (e.g. Nadal et al., Reference Nadal, Griffin, Wong, Hamit and Rasmus2014; Gattis and Larson, Reference Gattis and Larson2017; Reid, Reference Reid2017). Whilst most studies have been cross-sectional, a study using a longitudinal design has shown that microaggressions in the form of ‘underestimation of personal ability’ significantly predicted self-rated depression symptoms 1 year later – providing some indication of potential causation (Torres et al., Reference Torres, Driscoll and Burrow2010).
Research on microaggression is not without its critics. Some argue that a microaggression is an open concept with ‘fuzzy’ boundaries, full of contradictions and ambiguities – for example, both ignoring and attending to minority students in classrooms have been listed as microaggressions (Lilienfeld, Reference Lilienfeld2017). It is apparent that microaggressions are ambiguous and ‘lie in the eye of the beholder’, and so, variations in responses by targets of microaggressions may be a function of an individual's personality dispositions, a key confounder when asserting a causal association between microaggressions and adverse mental health outcomes (Lilienfeld, Reference Lilienfeld2017). Indeed, once accounting for scores of ‘perceived stress’ (feeling life is unpredictable, uncontrollable and overloaded), Torres et al. found that the predictive effect of microaggressions on depression symptoms was non-significant (Torres et al., Reference Torres, Driscoll and Burrow2010).
Nevertheless, the use of the term ‘microaggression’ is expanding. It is now used to describe snubs, slights and insults towards members of other marginalised social groups including women, sexual minorities and people with disabilities (Sue, Reference Sue2010). There is a growing literature on the experience of people affected by mental health problems, arguably a marginalised social group in its own right. This emerging field can be seen to fit into the wider literature on stigma towards mental illness – a broad concept that encompasses ignorance, prejudice and discrimination (Thornicroft, Reference Thornicroft2006).
The purpose of this scoping review was to answer the following research question: ‘What is the scope of the literature regarding mental health-related microaggressions towards people affected by mental health problems?’. We aimed to characterise the literature in this area (e.g. who is conducting this research, and from what discipline?), elucidate the purpose of research on this topic for this population (e.g. to describe the experiences of people with mental health problems or to measure the effect) and describe and synthesise the current evidence base. In doing so, we planned to clarify the definition of the term microaggression as it is used in relation to people with mental health problems. In addition, we aimed to identify the problematic areas of this research topic (e.g. varying definitions, the distinction between a microaggression and other forms of subtle discrimination) and propose the next steps for researchers in this field.
Methods
A scoping review approach was used to answer the research question. Like a systematic review, a scoping review is informed by an a priori protocol, involves systematic and exhaustive searching, must be transparent and reproducible, includes steps to reduce error and increase reliability, and presents data in a structured way (Munn et al., Reference Munn, Peters, Stern, Tufanaru, McArthur and Aromataris2018). However, in contrast to the systematic review method which is guided by a highly focussed research question, the scoping review method is guided by a requirement to identify all relevant literature, and as such it allows for procedural flexibility during the conduct of the review to achieve this aim (Arksey and O'Malley, Reference Arksey and O'Malley2005). A scoping review methodology was therefore considered highly appropriate for our research aim to characterise and synthesise the current literature. We followed the procedure outlined by Arksey and O'Malley (Reference Arksey and O'Malley2005) and further developed by Levac et al. (Reference Levac, Colquhoun and O'Brien2010).
This review complies with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (Moher et al., Reference Moher, Liberati, Tetzlaff and Altman2009). It follows an a priori developed review protocol, registered at the Open Science Framework platform (Barber et al., Reference Barber, Gronholm, Ahuja, Rüsch and Thornicroft2019).
Identifying the review question and aims
The research question was formulated through consideration of the concept and target population, using aspects of the SPIDER question format tool (i.e. examining Sample, Phenomenon of Interest, Design, Evaluation, and Research type) (Cooke et al., Reference Cooke, Smith and Booth2012). For this review, we specified only the ‘sample’ and ‘phenomenon of interest’ aspects, to fulfil the aim of characterising the literature in this area.
In line with the iterative, flexible nature of the scoping review process (Levac et al., Reference Levac, Colquhoun and O'Brien2010), the ‘sample’ was revised during the study selection process. Initially defined as ‘people with mental health problems’, this was refined to ‘people whose defining characteristic, in the study, is being affected by a mental health problem or disability’.
The ‘phenomenon of interest’ was mental health-related microaggressions specifically. This was specified as microaggressions attributed to a mental health problem or mental health-related disability. We did not include papers which addressed racial or other microaggressions directed towards people with mental health problems. Unless otherwise stated, the term microaggression in this manuscript refers to this narrow definition.
Identifying relevant studies
The search strategy was designed to identify formally published, peer-reviewed articles and selected grey literature, including research degree theses and book chapters but not ‘grey data’ (e.g. websites, tweets and blog posts). Four electronic health-oriented databases were searched in July 2019: Medline, EMBASE, PsycINFO and WorldCat Dissertation database. We also searched Google Scholar, identified as a powerful addition to traditional search methods (Haddaway et al., Reference Haddaway, Collins, Coughlin and Kirk2015). The first 300 results of a search on ‘Incognito mode’ (used to improve replicability) were screened.
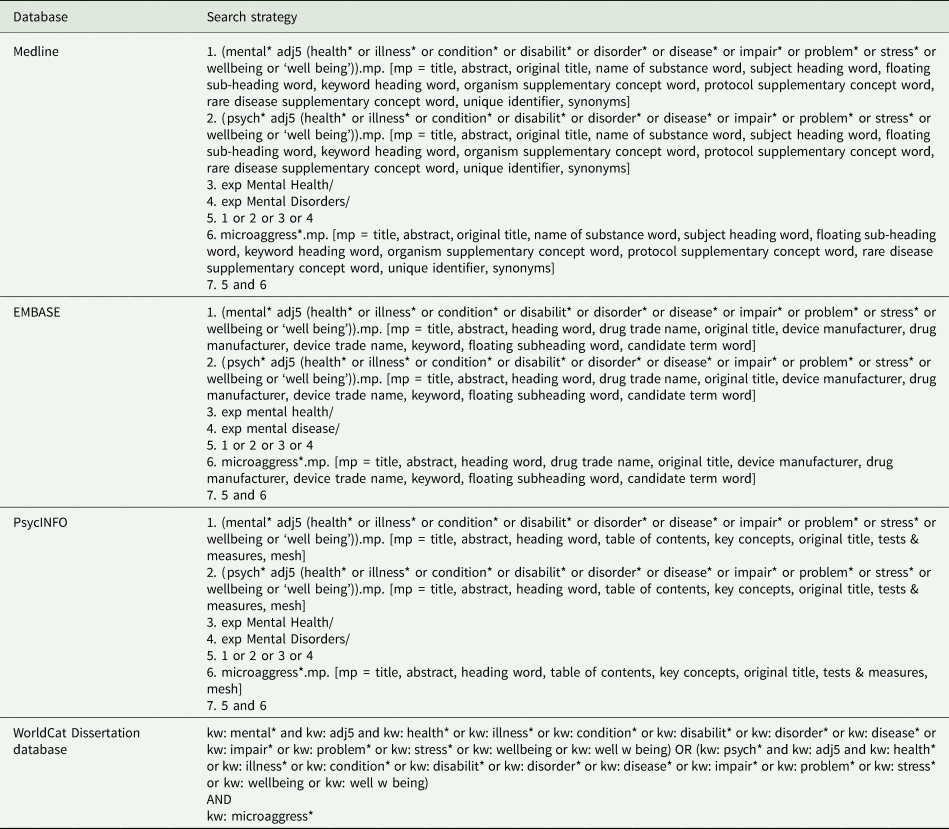
The search strategies consisted of keywords and subject headings related to ‘mental health’ and ‘microaggressions’. For Google Scholar the following search strategy was used: ‘(Mental* or Psych*) AND microaggress*’. Appendix 1 gives full search strategies for each database.
We supplemented the database and search engine searches by conducting backwards and forwards citation checking and contacting authors and experts in the field.
Study selection
Study selection followed a two-step approach: (1) title, abstract, key word screening, (2) full-text screening. In both stages, SB and SA independently screened a proportion of results (25 and 40%, respectively), with PCG acting as an arbitrator. Interrator reliability was calculated and exceeded 80%. SB screened the remainder of the results. In line with scoping review principles, inclusion criteria were developed iteratively through discussion between authors.
Data extraction and management
Data from the included full texts were extracted onto a ‘Characteristics of Included Studies’ table, including country, department/institution (lead author), publication type, study design, population of interest (sample size) and purpose (e.g. to describe the experience of microaggressions, or to validate a scale).
Qualitative synthesis and analysis
The results of included studies were synthesised using a basic narrative synthesis approach, applying principles of thematic analysis (Braun and Clarke, Reference Braun and Clarke2006) and thematic synthesis (Thomas and Harden, Reference Thomas and Harden2008) where appropriate, given the available data and how it could best be examined to answer the review questions.
Quality of included studies assessment
We used the Mixed Methods Appraisal Tool (MMAT) (Hong et al., Reference Hong, Pluye, Fàbregues, Bartlett, Boardman, Cargo, Dagenais, Gagnon, Griffiths, Nicolau, O'Cathain, Rousseau and Vedel2018) to assess the quality of included empirical studies. This tool is designed for quality assessment in systematic reviews that include quantitative, qualitative and mixed-method studies. Articles were assigned one point for each criterion that was fulfilled, and half a point for each partially met the criterion. These points were summed to produce an index based on the proportion of total criteria met. No studies were excluded from the synthesis due to low-quality score.
Results
In total, 1196 records were identified: 889 records from database searching, and 307 through other sources (300 from Google Scholar, five through communication with authors, two through consultation with experts). After duplicates were removed, 1000 records remained for title, abstract and key word screening. In total, 959 records were excluded at this stage, leaving 41 records for full-text assessment for eligibility, of which 17 met inclusion criteria for this review. This study selection procedure is illustrated in the PRISMA flow diagram (see Fig. 1).
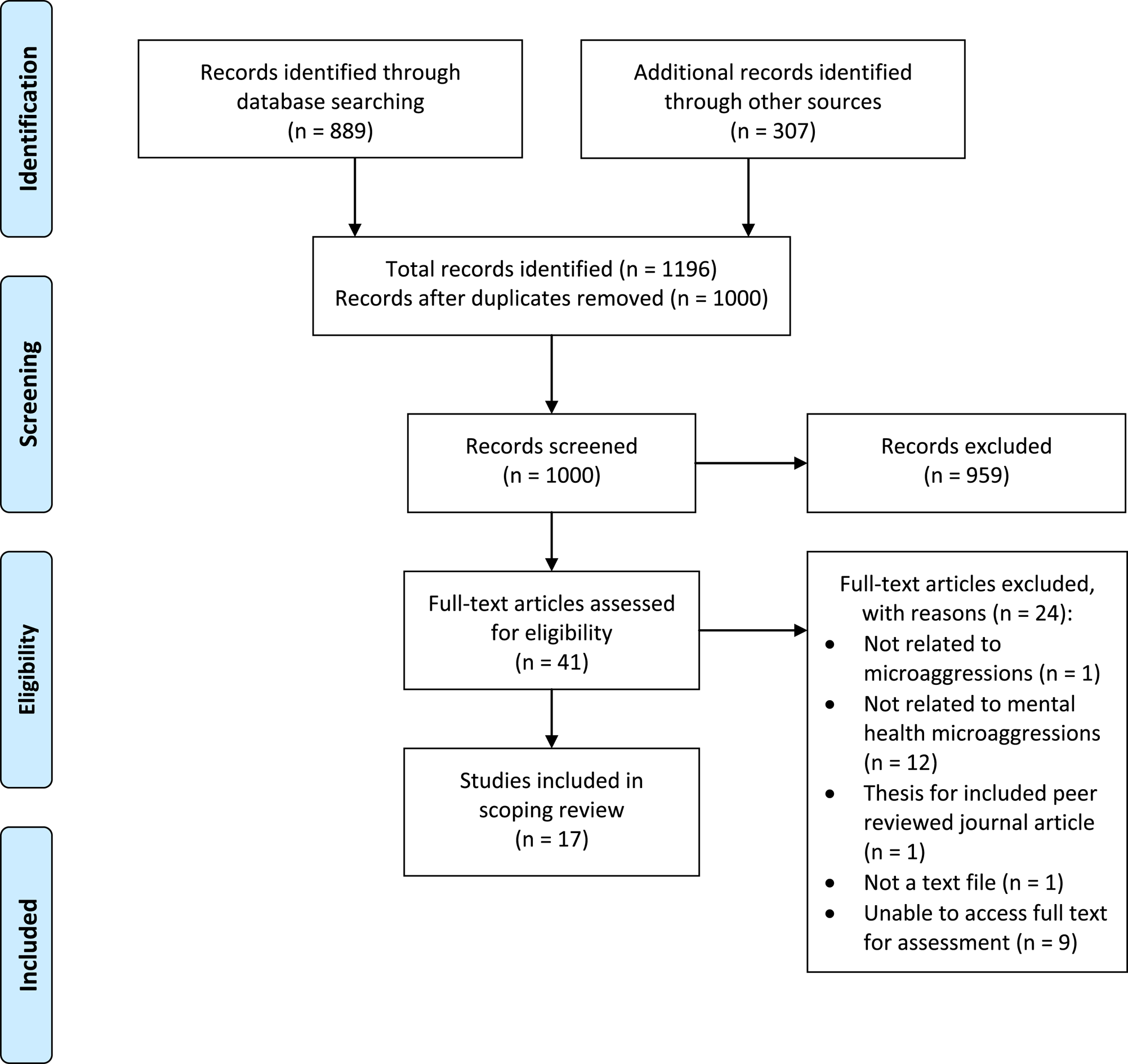
Fig. 1. PRISMA flow diagram. Adapted from Moher et al. (Reference Moher, Liberati, Tetzlaff and Altman2009).
Characterising the literature
The characteristics of included studies are summarised in Table 1.
Table 1. Characteristics of included studies
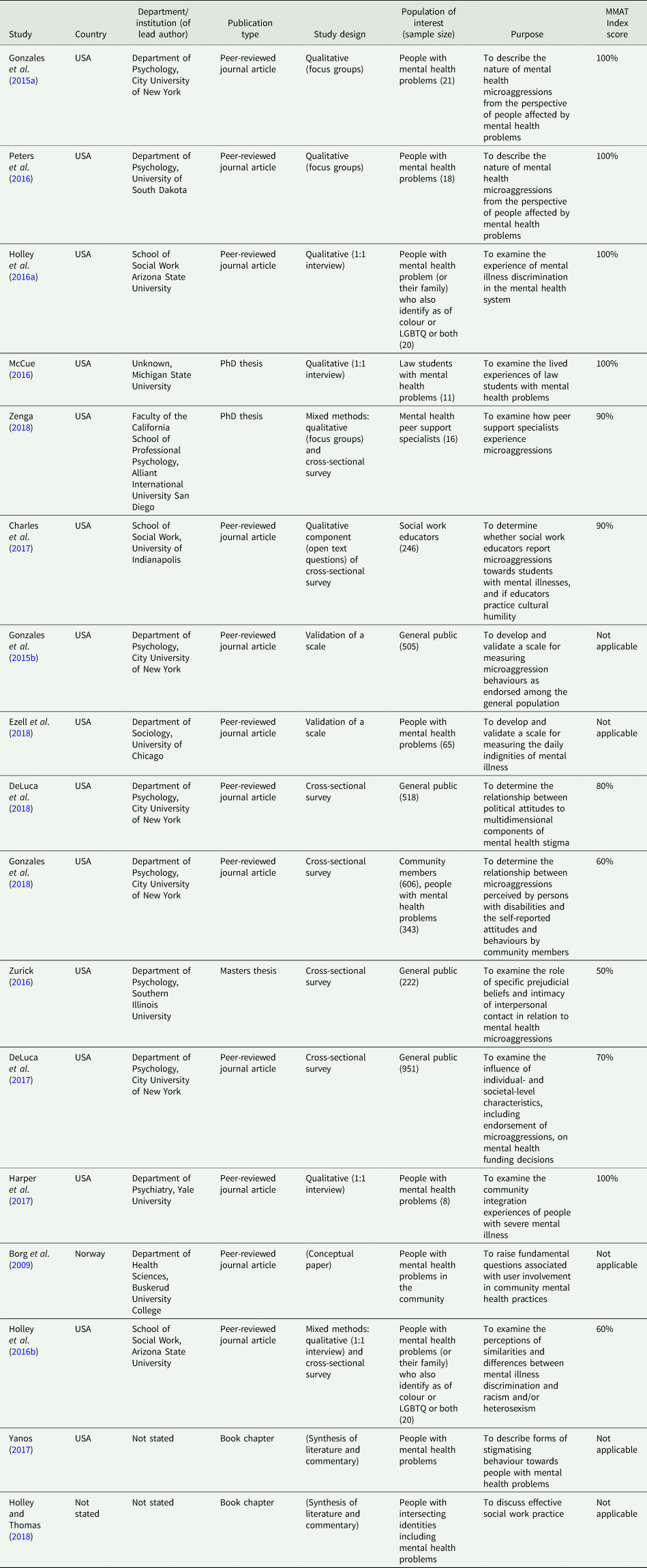
All papers and chapters were published in the last decade (16 in the last 4 years), 15 are from the USA (five from authors associated with the City University of New York) and most papers originated from departments of Psychology (n = 8), followed by Social Work (n = 3).
Six included empirical studies were qualitative in nature, using focus group (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a; Peters et al., Reference Peters, Schwenk, Ahlstrom and Mcialwain2016), one-to-one semi-structured interviews (Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a; McCue, Reference McCue2016; Harper et al., Reference Harper, Kriegel, Morris, Hamer and Gambino2017) and analysis of free-text survey questions (Charles et al., Reference Charles, Holley and Kondrat2017). Four were cross-sectional surveys (Zurick, Reference Zurick2016; DeLuca et al., Reference DeLuca, Clement and Yanos2017; DeLuca et al., Reference DeLuca, Vaccaro, Seda and Yanos2018; Gonzales et al., Reference Gonzales, Yanos, Stefancic, Alexander and Harney-Delehanty2018), with sample sizes from 222 to 951 participants. Four of these studies employed convenience sampling of the US public using online survey platforms. Two studies adopted a mixed-methods design (Holley et al., Reference Holley, Tavassoli and Stromwall2016b; Zenga, Reference Zenga2018). Two included publications aimed to validate a scale (Gonzales et al., Reference Gonzales, Davidoff, Deluca and Yanos2015b; Ezell et al., Reference Ezell, Chien-Wen, Wall and Link2018). The remaining three papers and chapters (Borg et al., Reference Borg, Karlsson and Kim2009; Yanos, Reference Yanos2017; Holley and Thomas, Reference Holley, Thomas and Dentato2018) were not research studies, but still met inclusion criteria and offered an insight into the scope of the literature.
Characterising the purpose of research on this topic for this population
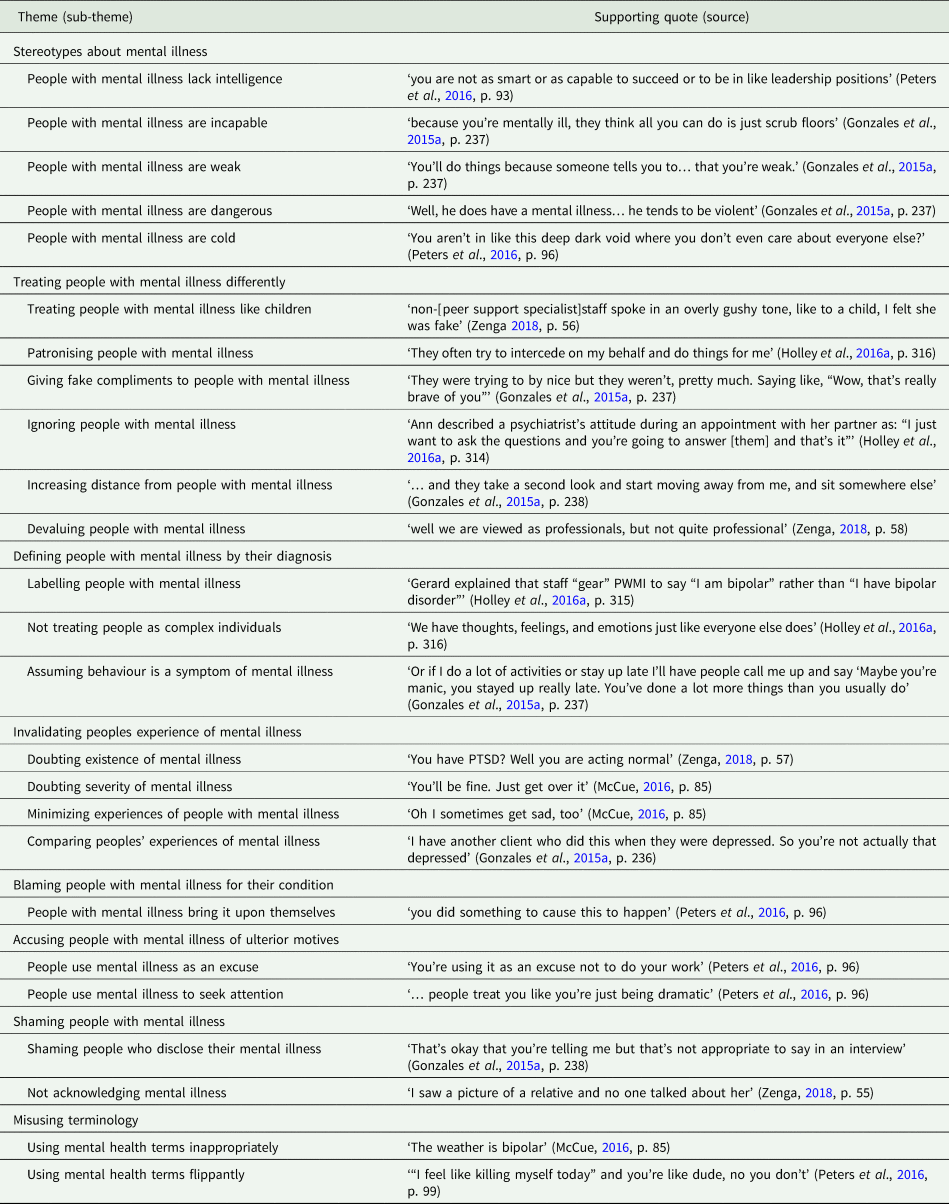
Five studies aimed to elucidate the nature of mental health microaggressions from the perspective of people affected by mental health problems (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a; Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a; McCue, Reference McCue2016; Peters et al., Reference Peters, Schwenk, Ahlstrom and Mcialwain2016; Zenga, Reference Zenga2018). In three, the participants had intersecting identities as racial and/or sexual orientation minority group members (Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a), law students (McCue, Reference McCue2016) and peer support specialists (Zenga, Reference Zenga2018). We synthesised the experiences of microaggressions described in these studies (see Table 2).
Table 2. A thematic synthesis of experiences described as mental health microaggressions
These five papers also provide data on the perpetrators of mental health microaggressions, which included family, friends and health professionals. For example, a participant in Gonzales et al. (Reference Gonzales, Davidoff, Nadal and Yanos2015a) stated: ‘People in my family, if I actually starting being happy they're like, “Are you sure you're okay?”’ (p. 237). Similarly, Peters et al. (Reference Peters, Schwenk, Ahlstrom and Mcialwain2016) provided an example of friends misusing terminology ‘I even have friends that say it… they're just like, “But oh man they were so bipolar”’ (p. 100). Additionally, a participant in McCue (Reference McCue2016) described an experience where a fellow student said ‘that he has depression’ and that ‘he could go out and get that extra time but he has dignity’ (p. 85), consistent with perpetration of a microaggression by a peer (by shaming mental illness). One further paper aimed to describe mental health microaggressions from the perspective of potential perpetrators (Charles et al., Reference Charles, Holley and Kondrat2017). They demonstrated that social work educators report personal reactions that reflect microaggressions.
Two papers aimed to create scales, one measuring the experience of microaggressions (Ezell et al., Reference Ezell, Chien-Wen, Wall and Link2018) and one measuring endorsement of microaggressions by possible perpetrators (Gonzales et al., Reference Gonzales, Davidoff, Deluca and Yanos2015b). The latter was used in three studies aiming to identify individual characteristics associated with endorsement of mental health microaggressions by the general public. Broadly, endorsement of microaggressions was positively associated with right-wing political views (DeLuca et al., Reference DeLuca, Vaccaro, Seda and Yanos2018), suburban values and socio-economic disadvantage (Gonzales et al., Reference Gonzales, Yanos, Stefancic, Alexander and Harney-Delehanty2018), authoritarianism (the attitude that people with serious mental illness cannot care for themselves and require coercion) and social restrictiveness (the belief that people with mental illness should be feared and excluded) (Zurick, Reference Zurick2016). Endorsement was negatively associated with benevolence (the belief that people with mental illness are innocent and naïve) (Zurick, Reference Zurick2016).
Two studies considered the impact of microaggressions. One qualitative study described a ‘negative outcome’ theme that included frustration, loss of self-esteem and alienation (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a). One quantitative study assessed the impact of endorsing microaggressions on preferences for mental health funding allocation by the general public and found a weak but significant negative correlation (DeLuca et al., Reference DeLuca, Clement and Yanos2017).
Defining the term microaggression as it is used in relation to people with mental health problems
We found that the majority (11/17) of papers directly or indirectly referenced a definition of microaggressions from the work of Sue et al. (e.g. Sue, Reference Sue2010; Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007), and eight listed the three types of microaggression described by Sue et al.: microassaults, microinsults and microinvalidations. Ezell et al. (Reference Ezell, Chien-Wen, Wall and Link2018) referenced Pierce et al. (Reference Pierce, Carew, Pierce-Gonzalez and Wills1977) and described a ‘nexus of recurrent, daily indignities, both overt and non-overt, that are directed at historically marginalised populations… which insult, degrade or otherwise demoralize their recipients’ (p. 28). Borg et al. (Reference Borg, Karlsson and Kim2009) describe ‘the things you experience every day that then add up and take their toll’ (p. 290). Three papers provided no reference but emphasised the ‘everyday’ (Harper et al., Reference Harper, Kriegel, Morris, Hamer and Gambino2017) or ‘subtle’ (DeLuca et al., Reference DeLuca, Clement and Yanos2017; DeLuca et al., Reference DeLuca, Vaccaro, Seda and Yanos2018) nature of microaggressions. There is an apparent consensus across all included studies that microaggressions are brief, everyday slights, snubs or insults, which may be subtle or ambiguous, but communicate a negative message to a target person based on their membership of a marginalised group, in this case, people with experience of mental illness.
Quality of included studies
The 12 empirical studies included in the review were assessed using the MMAT tool. Index scores are presented in Table 1. All of the qualitative studies (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a; Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a; McCue, Reference McCue2016; Peters et al., Reference Peters, Schwenk, Ahlstrom and Mcialwain2016; Charles et al., Reference Charles, Holley and Kondrat2017; Harper et al., Reference Harper, Kriegel, Morris, Hamer and Gambino2017) used an appropriate approach (interpretive or critical) and methods of data collection and analysis were well described and adequate. Overall, conclusions were well substantiated by data and the author's arguments were coherent. Of note, Charles et al. (Reference Charles, Holley and Kondrat2017) included a clear discussion of neutral and ambiguous findings. In general, there was an absence of reflexivity (with McCue (Reference McCue2016) a notable exception) or respondent validation. Three of the cross-sectional surveys used online convenience methods to sample US residents (Zurick, Reference Zurick2016; DeLuca et al., Reference DeLuca, Clement and Yanos2017, Reference DeLuca, Vaccaro, Seda and Yanos2018). In one study, the recruitment system stratified based on demographic attributes resulting in gender balance and equal numbers of four age groups and regions (DeLuca et al., Reference DeLuca, Vaccaro, Seda and Yanos2018). The other two were biased, for example, towards females. Zurick (Reference Zurick2016) found that 36.9% of their sample reported they had a mental illness, a limitation to the study of general attitudes. All three of these surveys used validated measures and appropriate statistical techniques. One cross-sectional study used an unvalidated perceived microaggression scale (Gonzales et al., Reference Gonzales, Yanos, Stefancic, Alexander and Harney-Delehanty2018). Two studies employed mixed methods (Zenga, Reference Zenga2018; Holley et al., Reference Holley, Tavassoli and Stromwall2016b), both using quantitative measures to triangulate the qualitative analyses. In both cases, there were weaknesses in the interpretation and integration of the quantitative findings, due to small sample size, reducing the quality of the study.
Discussion
The results of this scoping review have demonstrated an emerging field that is highly heterogenous methodologically. Largely in the last five years, researchers have described mental health-related microaggressions, operationalised them into scales, examined the characteristics associated with perpetration and begun to study the impact. By synthesising the results of four good quality qualitative studies and one mixed-method study, we provide an overview of the experiences people with mental illness have described as microaggressions in the literature to date.
The influence of Sue et al. from the racial microaggression field is evident; the majority of studies directly cite their definition and some authors framed their results in terms of microassualts, microinsults and microinvalidations (Peters et al., Reference Peters, Schwenk, Ahlstrom and Mcialwain2016; McCue, Reference McCue2016; Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a; Zenga, Reference Zenga2018). There are similarities between racial and mental health microaggressions, such as the assumption of inferiority or dangerousness (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007) and the notion of questioning the validity of the perceived microaggressions. For example, one focus group participant felt a false sense of support when she won an award (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a). This is an example of attributional ambiguity, arguably a threat to self-esteem by making it difficult to assess one's abilities (Crocker et al., Reference Crocker, Major, Steele, Gilbert, Fiske and Lindzey1998).
However, the mental health literature has key differences to the wider microaggression work. The ‘perpetrators’ of microaggressions towards people with mental illness are largely family and friends and health professionals, rather than strangers or acquaintances. This follows from mental illness being an arguably more concealable potential identity compared to race, but this has particular implications for intervening to reduce mental health microaggressions. In addition, certain experiences are unique to mental illness, such as symptomizing – where ‘emotions and behaviours considered “normal” for people without mental illness are assumed to be a symptom of their mental illness’ (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a, p. 236).
Criticism of the wider microaggression literature has focused on boundaries of the concept, the ambiguous and contradictory nature of microaggressions and role of unexplored confounders such as personality traits (Lilienfeld, Reference Lilienfeld2017). These challenges and problems are evident in the mental health literature too. Firstly, in synthesising the experiences described as microaggressions by people affected by mental health problems, we found examples that do not fit with the apparent consensus definition of microaggressions as brief, everyday forms of discrimination. For example, ‘I was arrested, I spent 8 months of my life in a cage for something I did not do’ (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a, p. 237). If this incarceration had anything to do with stigma or discrimination, it might be more helpfully considered an example of structural discrimination within the legal system than a microaggression. Similarly, ‘shortly before going back to work, they informed her that someone with more experience was hired’ (Zenga, Reference Zenga2018, p. 59) is not consistent with a subtle slight, snub or insult.
Defining what is, and what is not, a microaggression will be critical to distinguishing microaggressions from other described forms of discrimination. Currently, authors appear to be at odds as to whether the microaggression concept is new and ‘scarcely… studied or discussed’ (Gonzales et al., Reference Gonzales, Davidoff, Nadal and Yanos2015a, p. 234), or an extension or rebranding of previously described forms of covert discrimination or forms of oppression (e.g. Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a). In his book chapter, Yanos (Reference Yanos2017) explores the relationship between microaggressions and other forms of stigmatising behaviour. To distinguish a microaggression from a ‘social rejection’ experience, Yanos describes ‘the difference between situations in which others avoid initiating a relationship with someone and situations in which others actively end a relationship’ (p. 46). He places microaggressions on a spectrum of stigmatising behaviour, at ‘the lowest level of severity’ (p. 41).
Several papers discuss the changing, contradictory and ambiguous nature of microaggressions. For example, Charles et al. (Reference Charles, Holley and Kondrat2017) reflect that ‘the nature of language and what is not recognised as a microaggression is always in flux’ (p. 420) and that ‘reaching out’ to students who disclose their mental illness could be seen as either supportive or a microaggression. ‘Symptomizing’ also presents a ‘catch-22’ situation to friends, family members and health professionals. Sleep disturbances are well recognised to be manic prodromes (Sierra et al., Reference Sierra, Livianos, Arques, Castelló and Rojo2007), and a psychoeducational family intervention (including early warning signs) has been shown to improve the level of disability of patients with bipolar disorder (Fiorillo et al., Reference Fiorillo, Del Vecchio, Luciano, Sampogna, De Rosa, Malangone, Volpe, Bardicchia, Ciampini, Crocamo, Iapichino, Lampis, Moroni, Orlandi, Piselli, Pompili, Veltro, Carrà and Maj2015). Yet, one participant in Gonzales et al. (Reference Gonzales, Davidoff, Nadal and Yanos2015a) gives the following example of a microaggression: ‘…if I do a lot of activities or stay up late I'll have people call me up and say “Maybe you're manic, you stayed up really late…”’ (p. 237).
The authors of a number of the included studies suggest strategies to reduce perpetration of microaggressions and their impact. They focus on health professionals (Borg et al., Reference Borg, Karlsson and Kim2009; Peters et al., Reference Peters, Schwenk, Ahlstrom and Mcialwain2016; Charles et al., Reference Charles, Holley and Kondrat2017), institutions (Holley et al., Reference Holley, Mendoza, Del-Colle and Bernard2016a; McCue, Reference McCue2016) and the general public (DeLuca et al., Reference DeLuca, Clement and Yanos2017; DeLuca et al., Reference DeLuca, Vaccaro, Seda and Yanos2018), and consider training and awareness campaigns. However, given the evidence that family and friends often perpetrate microaggressions, it may be useful to target interventions to closer acquaintances, for example, in family therapy. Another paper included in this study highlighted resilience as a key theme in the experience of microaggressions by peer support specialists (Zenga, Reference Zenga2018). Having gained confidence through recovery, one participant explained ‘she has developed empathy and compassion because she believes that they are “trying to be supportive”’ (p. 62). Given the changing, ambiguous nature of microaggressions, supporting people with mental health problems to cope with these slights, snubs and insults may be critical to reducing the impact of microaggressions. This could be done, for example, by focusing on strategies that improve self-esteem.
Limitations
There are several limitations to this scoping review. Firstly, our search strategy extended to grey literature but not grey data, which may have contained important perspectives. Secondly, we identified several studies in the screening stages that we were unable to access, despite attempts to contact the authors, which may represent a loss of valuable data.
We adopted a narrow focus for this scoping review for reasons of feasibility, including only papers that referenced mental health-related microaggressions explicitly. Widening the search to include terms such as subtle and covert discrimination might have enabled us to comment on distinguishing features (if they exist) of microaggressions in particular.
Conclusions
This scoping review has revealed a highly heterogenous body of work relating to microaggressions towards people with mental illness. The research has been heavily influenced by the work of Sue et al. in the wider microaggression literature. However, it is also embedded in the broader field of discrimination towards people with mental illness, with apparent similarities to previously described forms of subtle discrimination such as social rejection.
We have identified many challenges in this field of research, not least issues with the definition and boundaries of the concept: what is, and what is not, a microaggression needs to be clear and distinct to other forms of discriminatory behaviour. Also, some authors have asserted that the experience of microaggressions has a negative impact on people with mental illness, with little empirical evidence. Further work, including a careful examination of potential confounding personality traits, is required (as has been done in the wider mental health stigma literature, see Schibalski et al. (Reference Schibalski, Müller, Ajdacic-Gross, Vetter, Rodgers, Oexle, Corrigan, Rössler and Rüsch2017)). Indeed, placing the experience of microaggressions at the ‘lowest level of severity’ (Yanos, Reference Yanos2017, p. 41) of stigmatising experiences may be premature. Daily exposure to subtle forms of discrimination may, paradoxically, have a greater cumulative negative effect than other forms of blatant, unambiguous discrimination (Crocker et al., Reference Crocker, Major, Steele, Gilbert, Fiske and Lindzey1998).
Acknowledgements
At the time of starting this review, SB was supported by the National Institute for Health Research (NIHR) Integrated Academic Training Programme as an Academic Foundation Programme Trainee. GT is supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) South London and by the NIHR Applied Research Centre (ARC) at King's College London NHS Foundation Trust, and the NIHR Applied Research and the NIHR Asset Global Health Unit award. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. GT receives support from the National Institute of Mental Health of the National Institutes of Health under award number R01MH100470 (Cobalt study). GT is supported by the UK Medical Research Council in relation to the Emilia (MR/S001255/1) and Indigo Partnership (MR/R023697/1) awards. PCG is supported by the UK Medical Research Council in relation to the Indigo Partnership (MR/R023697/1) award. SA receives support from the Economic and Social Research Council (ESRC) through the ASPIRES research project.
Financial support
None.
Conflict of interest
None.
Ethical standards
We have adhered to the principles of open and transparent reporting.
Appendix 1
Appendix 1 Full search strategy





 Open access
Open access