Amenorrhea is one of the most frequent and serious consequences of Anorexia Nervosa (AN). Resumption of menses (ROM) is considered an important goal and is associated with a better outcome.
To investigate the role of age, Body Mass Index (BMI), diagnostic subtype (restrictive vs binge-purging), history of childhood abuse, duration of illness, psychopathology and sex hormones on ROM in AN.
52 patients with AN and amenorrhea were enrolled at the start of treatment. Clinical parameters of interest were collected, and questionnaires were administered for the assessment of general (SCL-90-R) and specific (EDE-Q) psychopathology. Blood samples were taken to assess FSH, LH and estradiol levels. All patients were monitored regularly through psychiatric checkups until ROM, for up to four years.
A total of 30 (57.7%) subjects recovered their menstrual cycle in the follow-up period (mean time: 18.7 ± 14.8 months). Recovery was more frequent in the binge-purging subtype than in the restrictive subtype (82.4% vs 48.6%, p=0.019), and was significantly associated with diagnostic crossover (odds ratio=10.0, p=0.032). Multivariate Cox regression showed an increased likelihood of menstrual recovery for binge-purging subtype (p=0.005) and for those reporting a history of childhood abuse (p=0.025). Early ROM was also associated with baseline SCL-90-R scores (p=0.002) and FSH (p=0.011), while a longer duration of illness (p=0.003) and EDE-Q scores (p=0.009) predicted a later recovery.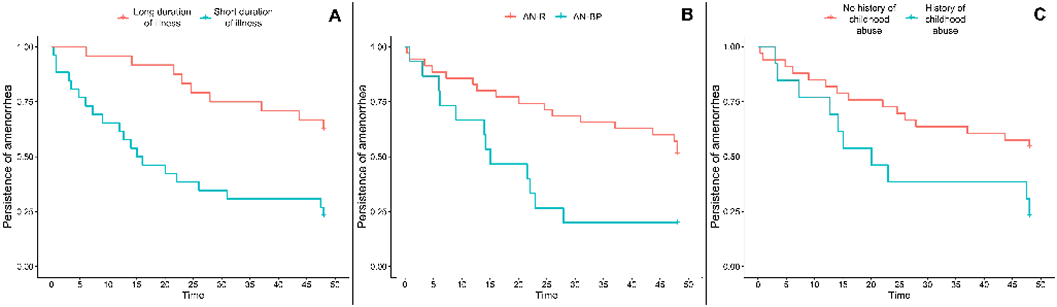
This study highlights the role of duration of illness, childhood abuse history and psychopathological characteristics in subjects with AN at the start of treatment in predicting ROM.
No significant relationships.

