Patients with OCD often show unsatisfactory response to first-line treatment, giving rise to a need for novel therapeutic approaches. Recent studies using tDCS for OCD treatment have shown promise.
To assess efficacy and safety of add-on c-tDCS over pre-SMA compared to sham stimulation in patients with OCD.
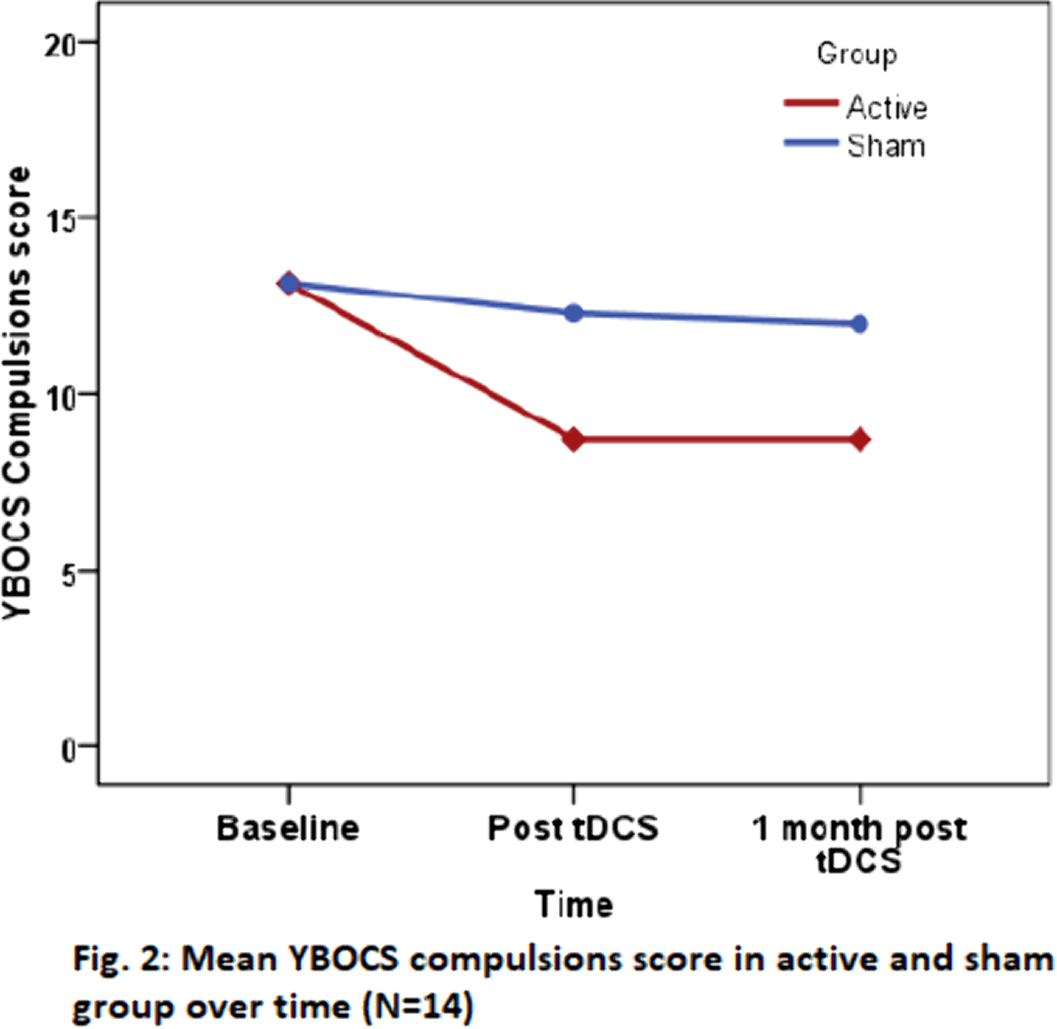
In this double-blinded study, fourteen patients with OCD were randomized to receive 10 sessions of either active (Cathode over pre-SMA, anode over right deltoid, 2mA, 20 minutes per session, 2 sessions per day, 2 hours apart) or sham tDCS. YBOCS, HAM-D, HAM-A, CGI, Wisconsin Card Sorting Test (WCST), and Stroop Test were administered at baseline, post-tDCS, and 1 month post-tDCS.
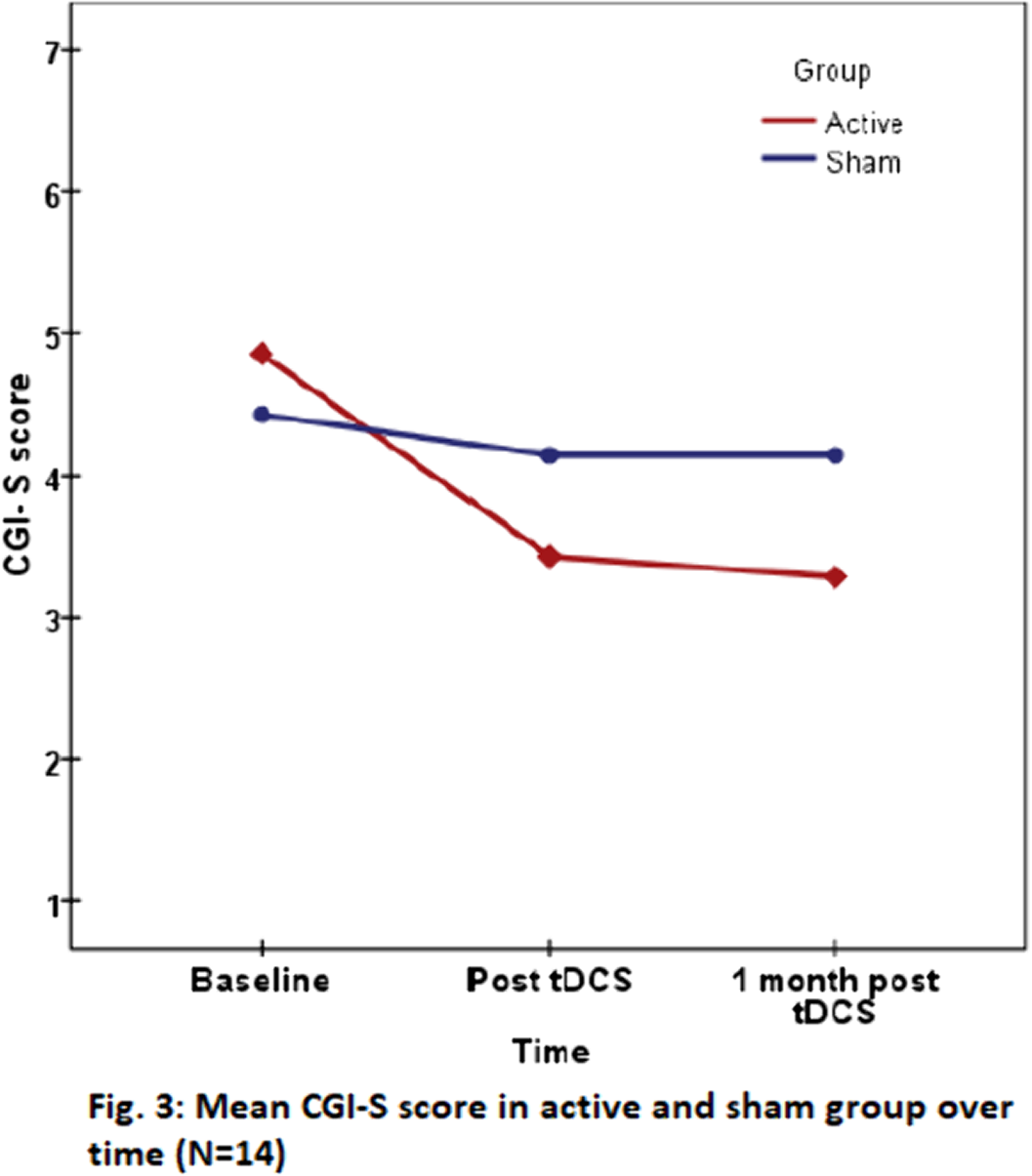
Group×time interaction effect for YBOCS scores with Repeated Measures ANOVA was not statistically significant, however, reduction in scores in active group was higher, with large effect size (YBOCS scores: Obsessions-ηp2=.344, Compulsions-ηp2= .384, Total-ηp2=.392) (Fig.1 & 2). At 1 month, 42.9% patients in active group and none in sham group showed response. CGI-S score (p=0.016, ηp2=.531) (Fig. 3) and four parameters of WCST (Perseverative responses:p=0.038, ηp2=.448;Percent perseverative responses:p=0.026, ηp2=.485;Percent perseverative errors:p=0.038, ηp2=.447;Trials to complete first category:p=0.011, ηp2=.563) significantly reduced in active group. No significant difference in change in depressive and anxiety symptoms between groups, or change in Stroop Test performance was noted. Adverse effects included transient headache and tingling sensation.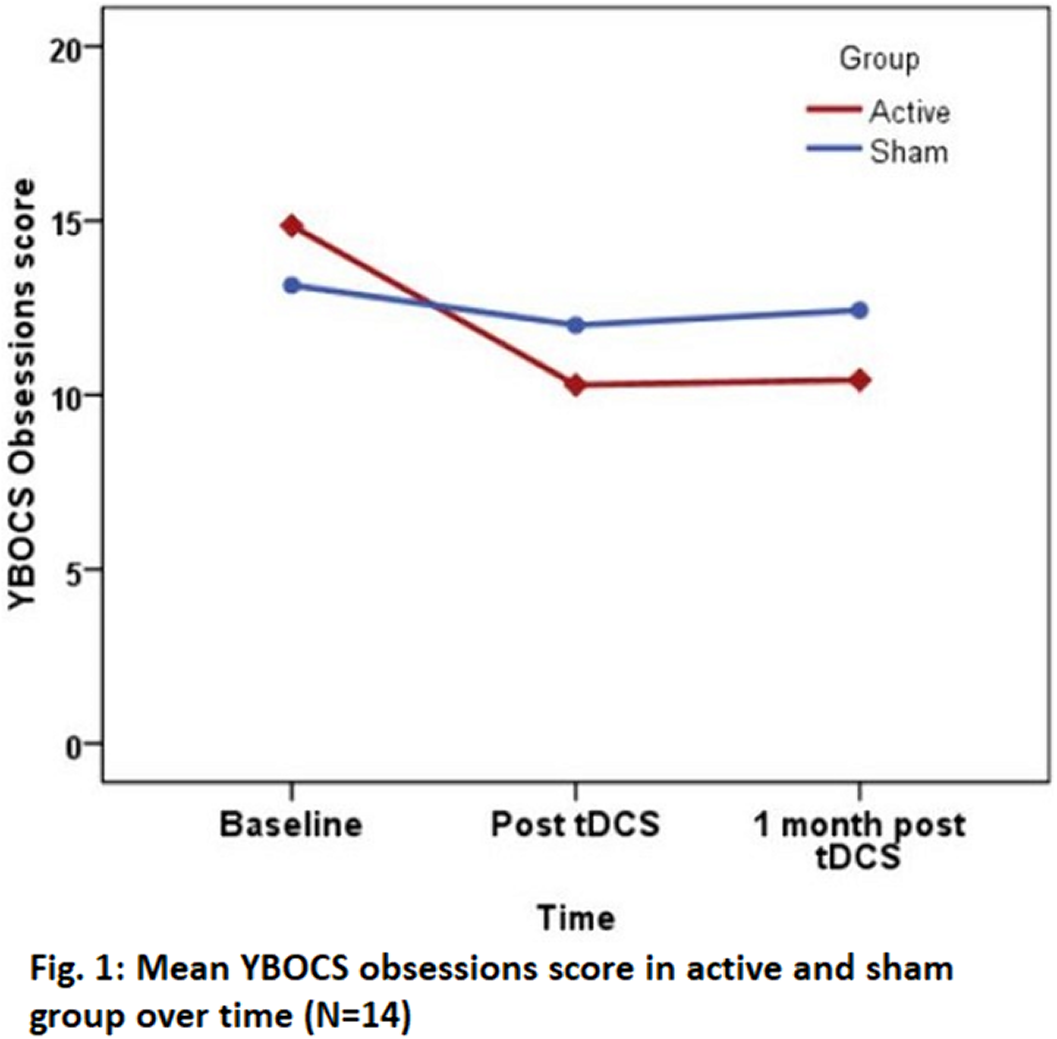
Cathodal tDCS over pre-SMA may be effective in reduction of obsessions, compulsions, illness severity, and enhancing cognitive flexibility in patients with OCD, with no major adverse effects. Larger studies are required to confirm these findings.
No significant relationships.

