This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
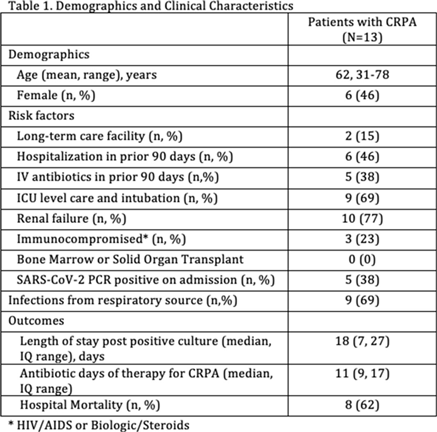
Background: Hand hygiene is essential to preventing the spread of disease in hospitals. Renewed emphasis has been placed on hand hygiene during the COVID-19 pandemic. We investigated whether UNC Medical Center’s well-established Clean-In Clean-Out (CICO) program for hand hygiene observations was sustainable throughout a public health and healthcare crisis and whether the COVID-19 pandemic had an effect on hand hygiene compliance. Methods: UNC Medical Center utilizes a crowd-sourced hand-hygiene audit application, CICO, to track hand-hygiene observations, compliance, and feedback. This application encourages participation from all staff and promotes providing real-time feedback in the form of a compliment or reminder when performing hand hygiene observations. During this evaluation, hand hygiene data were queried from the CICO application on the number of observations performed, hand hygiene compliance percentage, and feedback compliance percentage from July 2019 to December 2020. Hand hygiene data were compared to patient volumes in different care settings and the number of hospitalized patients being treated for COVID-19. Results: Initial increases in hand hygiene observations, compliance, and feedback were detected in the months leading up to UNC Medical Center receiving its first SARS-CoV-2–positive patient. Observations were highest when patient volumes were low due to closed clinics and restrictions on elective surgeries (Figure 1). When patient volumes returned to pre–COVID-19 levels coupled with treating more COVID-19 patients, the number of observations and compliance rate metrics declined. Feedback compliance percentage remained relatively stable through the entire period (Figure 2). Conclusions: Despite the additional strain on healthcare staff during COVID-19, the CICO model was a sustainable method to track hand hygiene observations and compliance. Notably, however, engagement was highest when patient census was lower, demonstrating that operating at a high capacity is not beneficial for patient safety. Due to the success and sustainment of the CICO program, UNC Medical Center used this model to create a Mask-On Mask-Up campaign to engage staff to submit observations, track compliance, and encourage feedback to promote the appropriate use of masks during COVID-19.
Funding: No
Disclosures: None
Figure 1.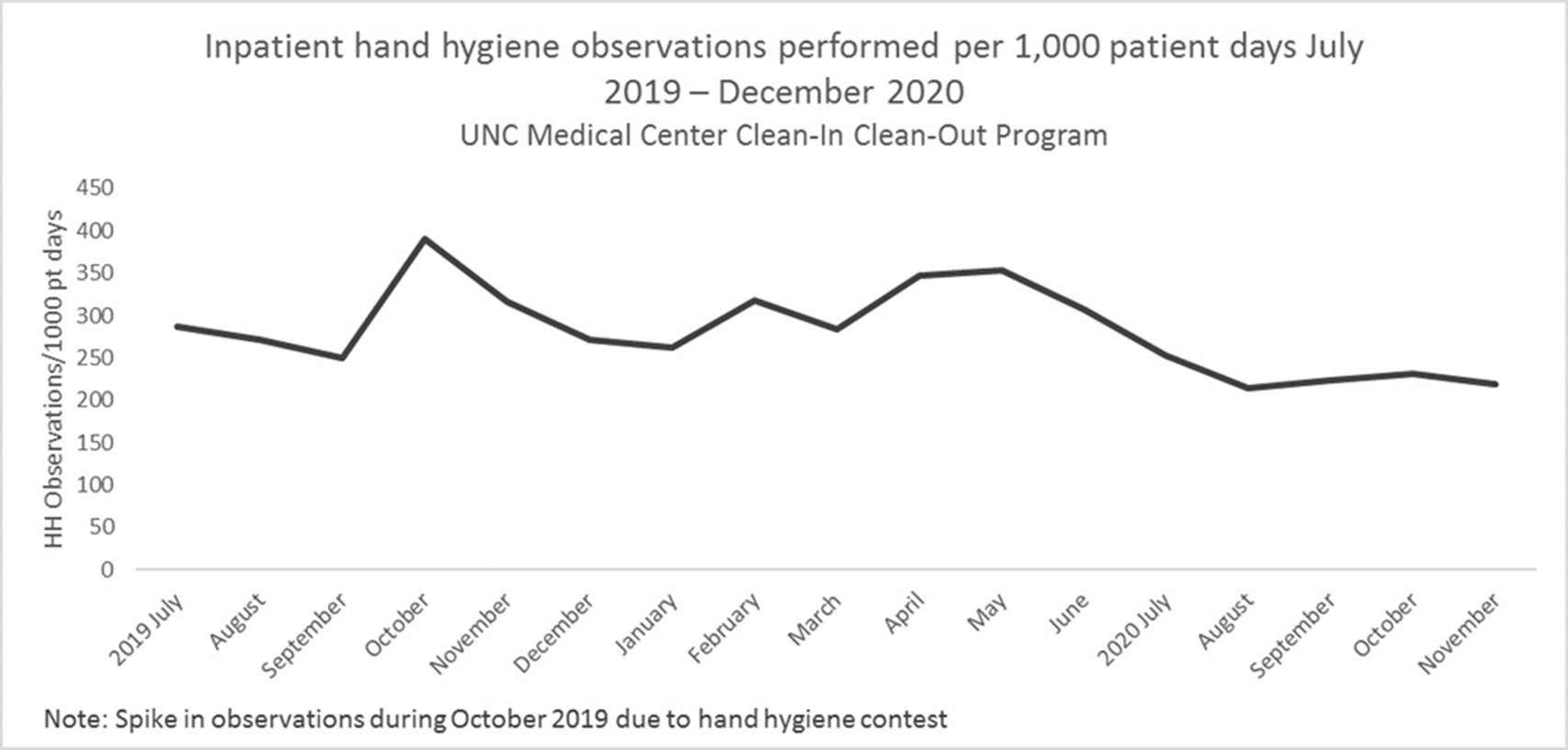
Figure 2.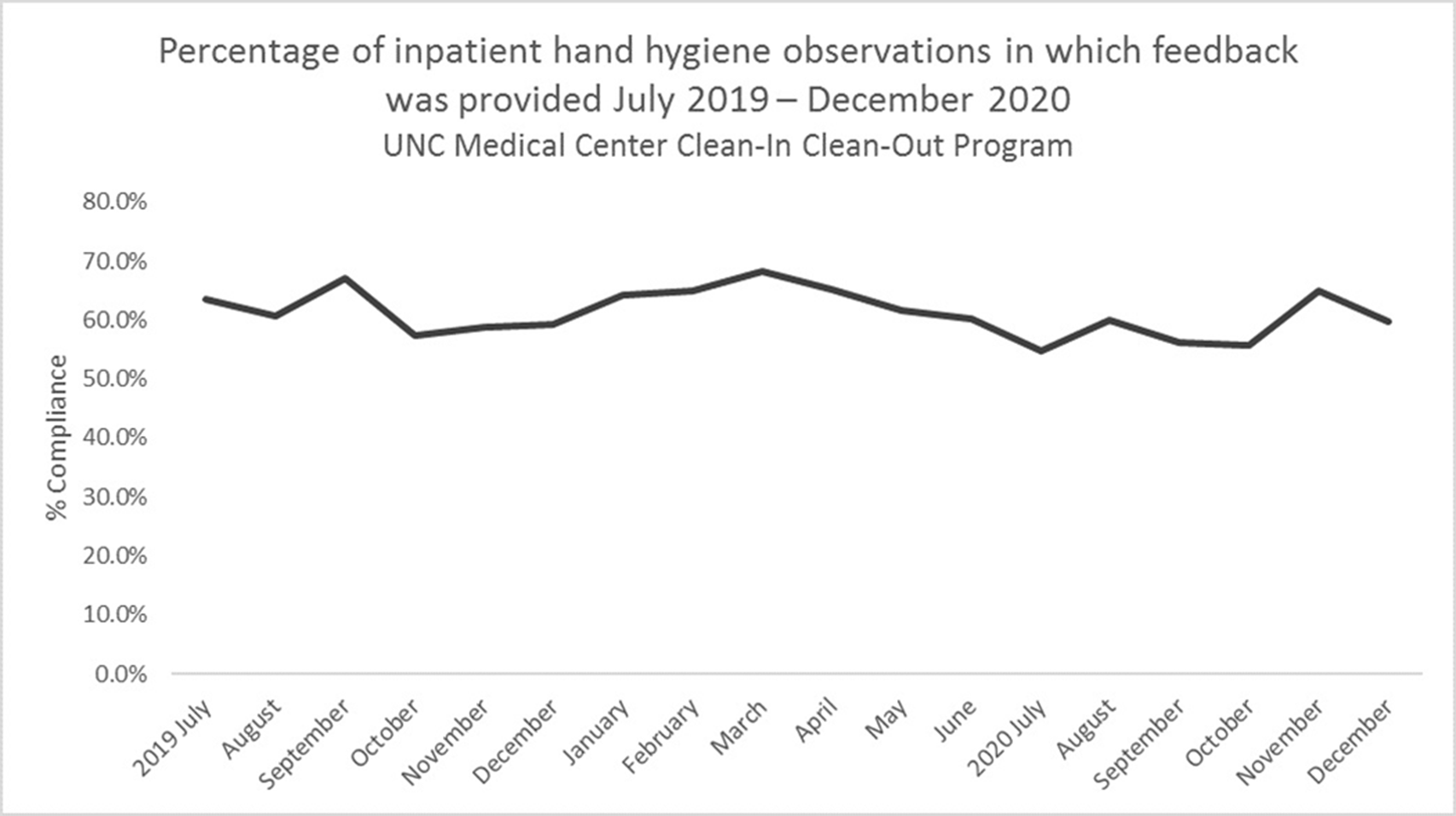
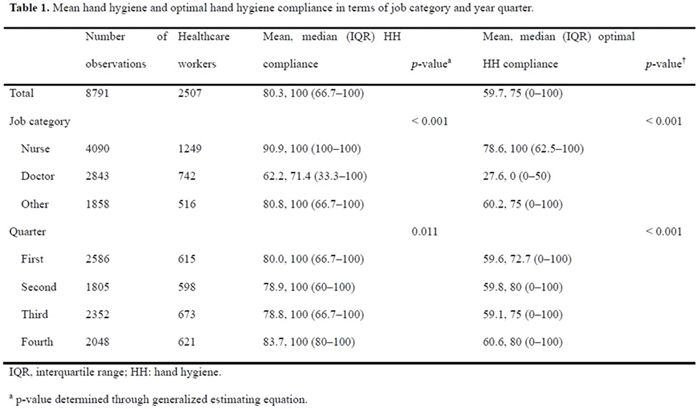
Background: We sought to determine the minimum number of observations needed to determine hand hygiene (HH) compliance among healthcare workers. Methods: The study was conducted at a referral hospital. We retrospectively analyzed the result of HH monitoring from January to December 2018. HH compliance was calculated by dividing the number of observed HH actions by the total number of opportunities. Appropriate HH compliance rates were calculated based on the 6-step technique, modified from the World Health Organization (WHO) recommendation. The minimum number of required observations (n) was calculated by the following equation using overall mean value (r), absolute precision (d), and confidence interval (1-α) [The equation: n3 Zα/22×ρ×1-ρ/d2]. We considered ds of 5%, 10%, 20%, and 30%, with CIs of 99%, 95%, and 90%, respectively. Among the various cases, we focused on 10% for d and 95% for CI. Results: During the study period, 8,791 opportunities among 1,168 healthcare workers were monitored. The mean HH compliance and appropriate HH compliance rates were 80.3% and 59.7%, respectively (Table 1). The minimum number of observations required to determine HH compliance rates ranged from 2 (d, 30%; CI, 90%) to 624 (d, 5%; CI, 99%), and the minimum number of observations for optimal HH compliance ranged from 5 (d, 30%, CI, 90%) to 642 (d, 5%; CI, 99%) (Figure 1). At 10% absolute precision with 95% confidence, the minimum number of observations to determine HH and optimal HH compliance were 61 and 92, respectively. Conclusions: The minimum number of observations to determine HH compliance varies widely according to setting, but at least 5 were needed to determine optimal HH compliance.
Funding: No
Disclosures: None
Figure 1.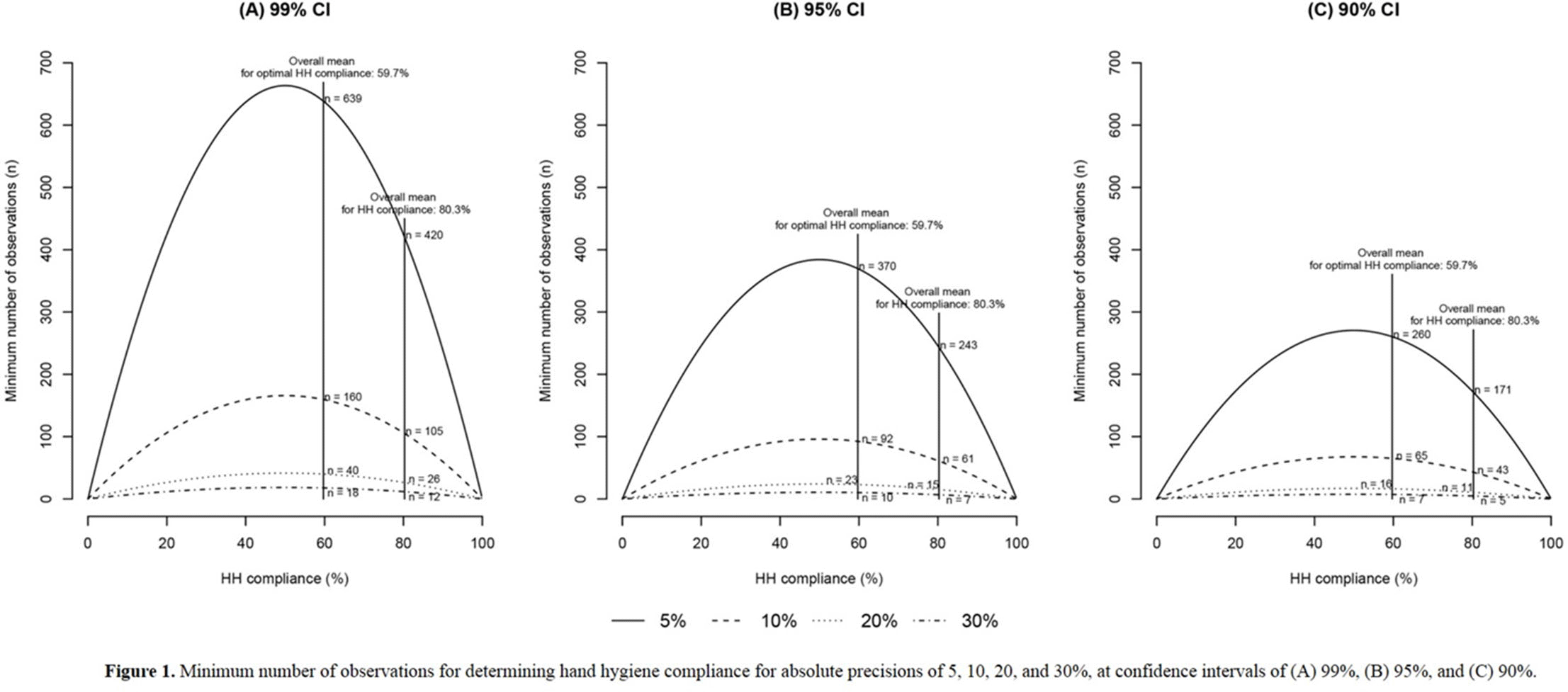
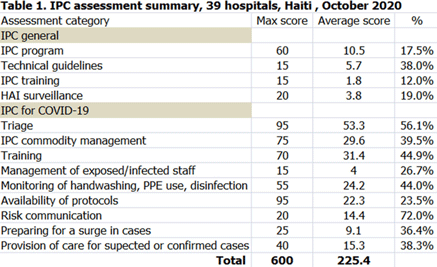
Background: Infection prevention and control (IPC) is key (1) to keeping health workers and patients safe from contracting infections during care, (2) to enabling continuity of essential health services, and (3) to pandemic preparedness and response. Frontline health workers are at 3-fold increased risk for COVID-19 (Lancet 2020) and account for 6% of COVID-19 hospitalizations (CDC 2020). With the support of the US Agency for International Development Bureau of Humanitarian Assistance (USAID/BHA) and collaboration of the Haitian Ministry of Health (MSPP), MSH’s Rapid Support to COVID-19 Response in Haiti project (RSCR Haiti) developed an instrument to assess select public hospitals and identify IPC gaps that informed COVID-19 response and system strengthening measures for increasing patient and provider safety. Methods: The IPC tool contains 13 IPC domains and 80 questions, for a total of 600 points. It was developed based on the World Health Organization IPC Assessment Framework for Health Facilities (2018) and US Centers for Disease Control Facility Readiness Assessment for COVID-19 (2020). In total, 39 health facilities chosen by the MSPP across all 10 departments of Haiti were evaluated in October 2020. Data were analyzed in Microsoft Excel by category, site, and IPC capabilities then classified as inadequate, basic, intermediate or advanced. Results: IPC capabilities scored as inadequate in 18% and basic in 67% of hospitals (Graph 1). No institution was advanced. Among health facilities, IPC programs existed in only 18%; IPC guidelines or procedures were present in 38%; staff were trained regularly in 12%; and healthcare-associated infection surveillance was performed in 19%. Systems for COVID-19 triage existed in 56%; 39% had IPC commodity management systems; 45% provided COVID-19 training; 26% practiced monitoring of staff and patients for COVID-19; 36% had protocols for an influx of COVID-19 cases; and 72% practiced risk communication (Table 1). Conclusions: No health facility was sufficiently equipped to implement adequate COVID-19 IPC measures, and all needed strengthening, even in the highest-scoring IPC areas. Through RSCR Haiti, MSH and MSPP were able to identify and address priorities in hospitals: establishing hospital IPC programs; training staff; monitoring health workers and patients; and implementing guidance, triage, and commodity-management systems. This study demonstrates that it is possible to do a quick yet thorough assessment to rapidly identify IPC needs and opportunities, using the results to rapidly build response capacity. Haiti’s experience of integrating locally contextualized global IPC tools to inform systemic COVID-19 response measures can benefit other experts globally.
Funding: United States Agency for International Development Bureau of Humanitarian Assistance (USAID/BHA)
Disclosures: None
Figure 1.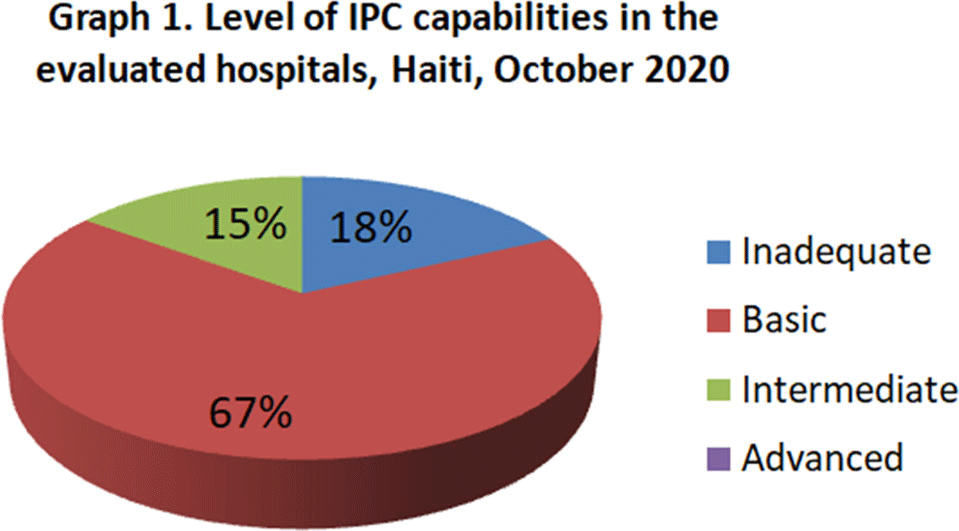
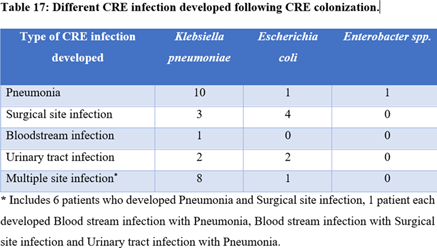
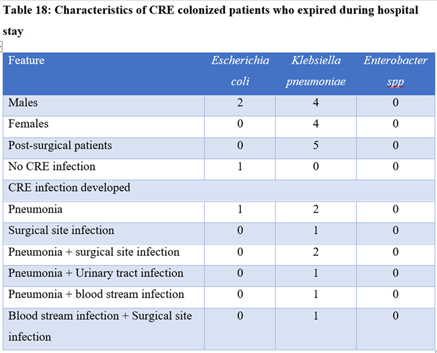
Background: Carbapenem-resistant Enterobactericeae (CRE) has emerged as a global health threat with increasing incidence. It is a particular problem in India because control over antibiotics prescription is really poor; these agents can be easily bought over the counter and the antibiotic prescription threshold is low among Indian doctors. Also, even when administered, antibiotics are given in inappropriate dosages and durations. CRE infections are a healthcare challenge due to their difficulty to treat and high morbidity and mortality. Colonization requires infection prevention measures, and it should be prioritized. Methods: We sought to determine the prevalence rate of CRE colonization in the gastrointestinal tract in newly admitted ICU patients along with follow-up of any subsequent infection following colonization. A prospective observational study was carried out among ICU patients from January 2019 to August 2020 by collecting perirectal swabs from patients who gave consent. Clinical variables were identified, and the relationship between CRE colonization and subsequent systemic CRE infection was assessed. Processing was carried out by culturing on MacConkey agar plate with ertapenem disk and further identified using conventional microbiological techniques. The ertapenem MIC was determined using an Epsillometer (E) test. The modified carbapenem inactivation (mCIM) test and the EDTA carbapenem inactivation method (eCIM) were used to confirm carbapenem resistance using Clinical Laboratory Standards Institute 2020 guidelines (Figure 1). Results: Among 192 ICU patients, 37 (19.27%) were colonized with CRE (Table 1). Also, 13 (35.13%) CRE isolates showed metallo-β-lactamase resistance. Furthermore, 18 CRE isolates (48.64%) showed serine carbapenemase activity; 6 CRE isolates showed no carbapenemase activity. Klebsiella pneumoniae (n = 25 of 37, 67.56%) was the most common CRE isolated followed by Escherichia coli (n = 11 of 37, 29.72%) and 1 isolate of Enterobacter spp (n = 1 of 37, 0.02%). Of 37 patients, 33 (89.18%) developed CRE infection during their hospital stay. Pneumonia was the most common infection developed (36.36%), followed by surgical site infection (21.21%) and urinary tract infection (12.12%). Only 1 patient developed a bloodstream infection. However, 9 patients (27.27%) developed multiple-site infections. Of 37 CRE-colonized patients, 10 (27.02%) died during their hospital stay. Conclusions: Our study highlights the increased risk of CRE infection and mortality in patients with CRE colonization in ICU patients. Hence, CRE perirectal screening for detection of asymptomatic carriers should be conducted, and strict infection control measures, such as isolation and cohorting with barrier nursing of such patients, should be done to prevent further spread of CREs in hospital settings.
Funding: No
Disclosures: None
Figure 1.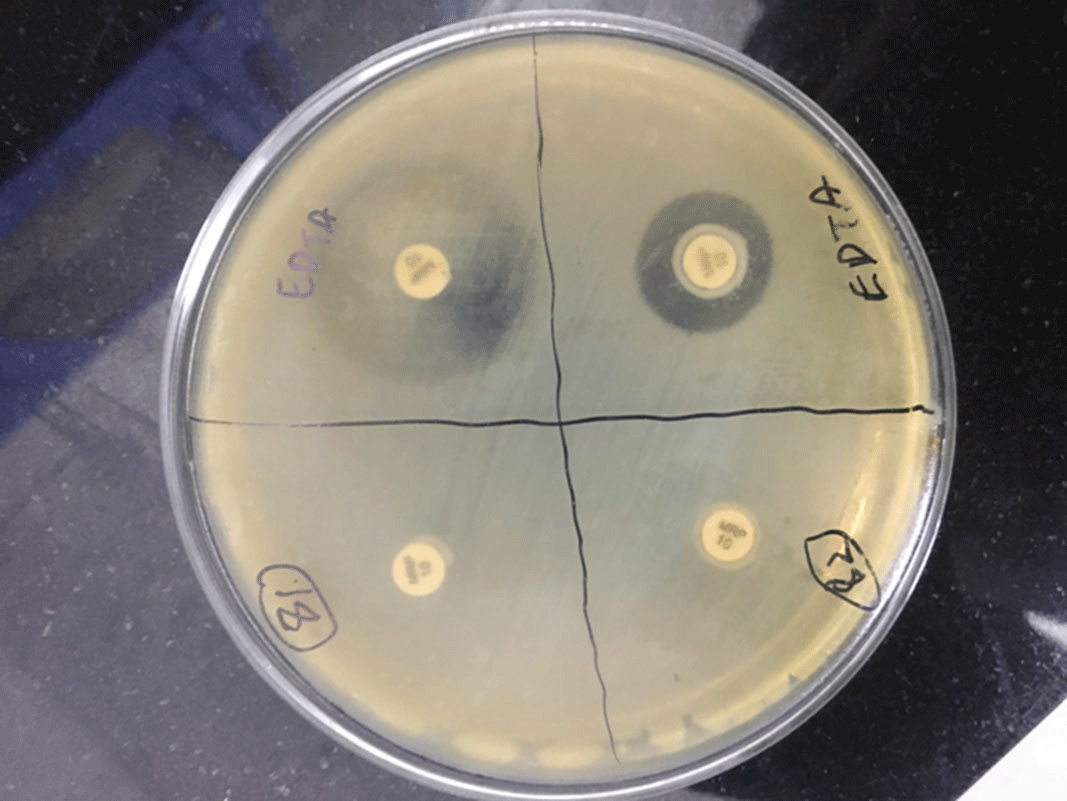
Background: Medical tape is used routinely for a variety of tasks across healthcare settings. The literature contains numerous publications in which common practices around medical tapes have been suspected to lead to infection transmission. Healthcare providers can turn to individually packaged single-patient-use medical tape rolls to help reduce cross-contamination risk by limiting exposure to environmental contaminants, minimizing contact with hospital surfaces and equipment, and minimizing exposure to healthcare workers’ hands and other patients. Methods: We evaluated the effect of individually packaged tape on cross contamination using a controlled laboratory assay. Ceramic tiles were inoculated with microorganisms evenly spread across the surface and allowed to air dry. Using gloves, packaged and unpackaged tapes were rolled over their entire outside circumference onto the contaminated tiles to simulate cross contamination. Using new gloves, the packaged tapes were then removed from their package with minimum contact. All cross-contaminated tape rolls were placed in phosphate-buffered water and mixed in a vortexer for bacterial recovery procedures. Serial dilutions were plated on appropriate media for bacterial enumeration. The average log10 colony-forming unit (CFU) recovery was measured for comparison. We used 4 types of tapes in this study (3M Micropore S Surgical Tape, 3M Medipore H Soft Cloth Surgical Tape, 3M Durapore Surgical Tape, and 3M Transpore White Surgical Tape). We used 4 different microorganisms as inoculates: Staphylococcus aureus (methicillin-resistant), Enterococcus faecium (vancomycin-resistant), Klebsiella pneumoniae (carbapenem-resistant), and Clostridium difficile (spore). Each test (tape and bacteria combination) was done in 3 or 6 replicates; each bacterial enumeration was the average of duplicate plates. The detection limit for this method is 8 CFU per sample, which is equivalent to 0.9 log10. Results: The results for all tapes tested showed a statistically significant lower mean log10 recovery of each of the microorganisms tested for packaged versus unpackaged tape (Figure 1). The mean differences of log10 recoveries from a packaged and unpackaged tape ranged from 2.51 log10 (for S. aureus on Micropore S) to 4.64 log10 (for K. pneumoniae on Medipore H). This is equivalent to 99%–99.99% cross-contamination protection from the 4 organisms tested. Conclusions: Individual packaging of medical tape rolls protects them from external contaminants. Even if the packaging becomes contaminated, the tape retrieved from the package will be significantly less contaminated than it would have been from exposure to the same contaminants without packaging.
Funding: 3M Company
Disclosures: None
Figure 1.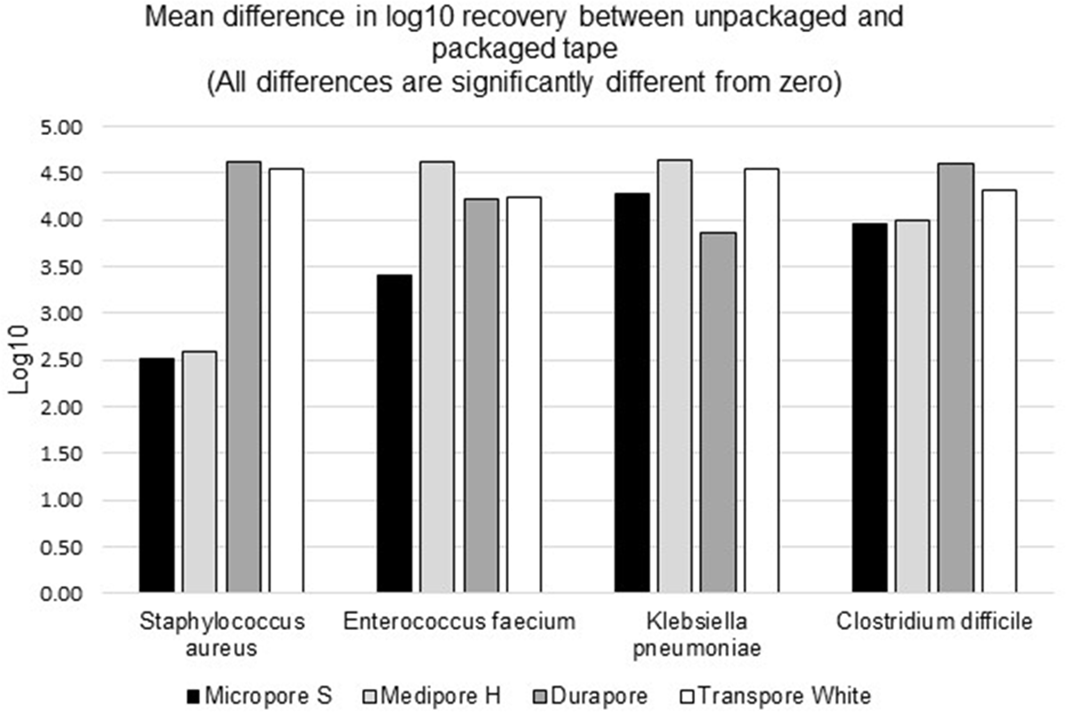
Background: Patient colonization and shedding of vancomycin-resistant enterococci (VRE) is a major source of environmental contamination leading to VRE transmission in nursing homes. We hypothesize that we can inform mitigation strategies by identifying patient clinical and microbiota features associated with environmental contamination with VRE. Methods: During a 6-month period of active surveillance in 6 Michigan nursing homes, 245 patients (with 806 follow-up visits) were enrolled. Patient clinical data and swabs for VRE were collected from multiple body sites and high-touch environmental surfaces. In total, 316 perirectal swabs were collected from 137 patients for gut microbiota analysis and community status type (CST) assignment based on taxonomic composition. The associations between VRE colonization pattern, gut microbial CST, and patient factors were examined using multivariable generalized estimating equations, adjusting for patient-and facility-level clustering. We used VRE colonization patterns to group study visits: “uncolonized” (patient−/environment−); “environment-only” (patient−/environment+); “patient-only” (patient+/environment−); “both” (patient+/environment+). Results: Across all study visits, VRE colonization on patient hand and groin/perirectal area was positively correlated with VRE contamination of high-touch environmental surfaces, suggesting direct transfer of VRE between patient and environment via patient hands (Figure 1A). We next set out to identify patient factors associated with patient colonization and environmental contamination. At baseline, while patients in the “both” group had anticipated risk factors such as longer prior hospitalization and more frequent broad-spectrum antibiotic use, they were unexpectedly younger than “uncolonized” patients and had similar functional status. This last feature contrasted with the “patient-only” group, characterized by higher urinary catheter use and higher functional dependence, suggestive of lower functional dependence facilitating patient contamination of their environment. No clinical features distinguished “uncolonized” and “environment-only” patients (Table 1). Lastly, in multivariable analyses, we determined the contribution of patient functional status and gut microbiota features to environmental contamination. Low-diversity CST, characterized by reduced anaerobic taxa, was weakly associated with “patient-only” and significantly associated with “both.” Notably, high functional dependence was significantly associated with “environment-only” and “patient-only” but not “both,” indicating high-functioning patients with disrupted gut microbiota as drivers of environmental contamination (Figure 1B). Conclusions: Our findings suggest that antimicrobial exposure disrupts patient gut microbiota, a significant mediator of colonization dynamics between patients and their environment, and that high-functioning patients may be more likely to spread VRE between their body sites and high-touch environmental surfaces (Figure 2). These findings highlight both antibiotic stewardship and patient hand hygiene as important targets for interrupting transmission mediated by environmental contamination.
Funding: No
Disclosures: None
Figure 1.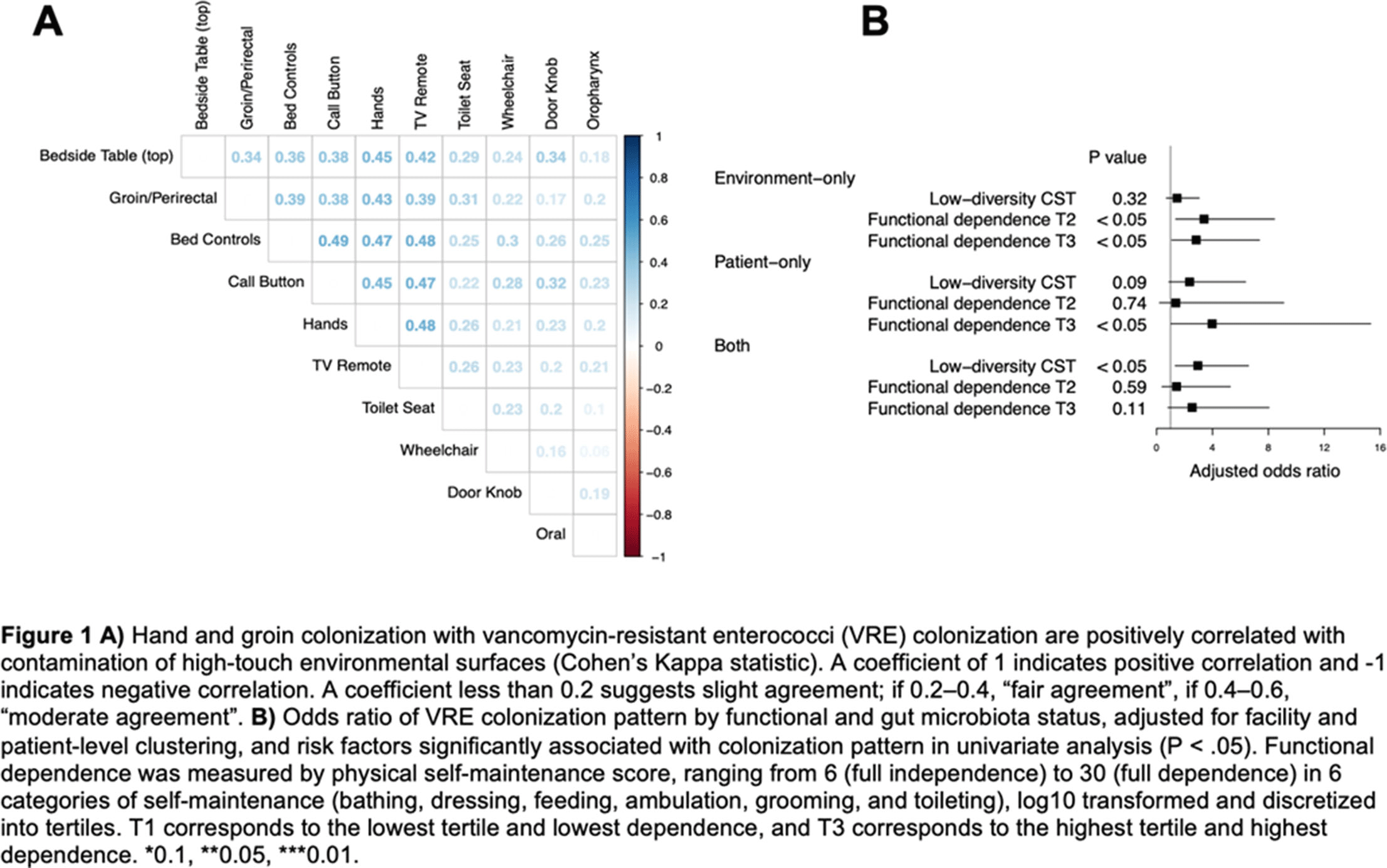
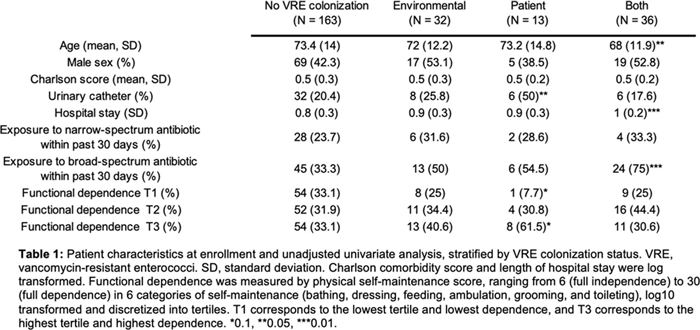
Figure 2.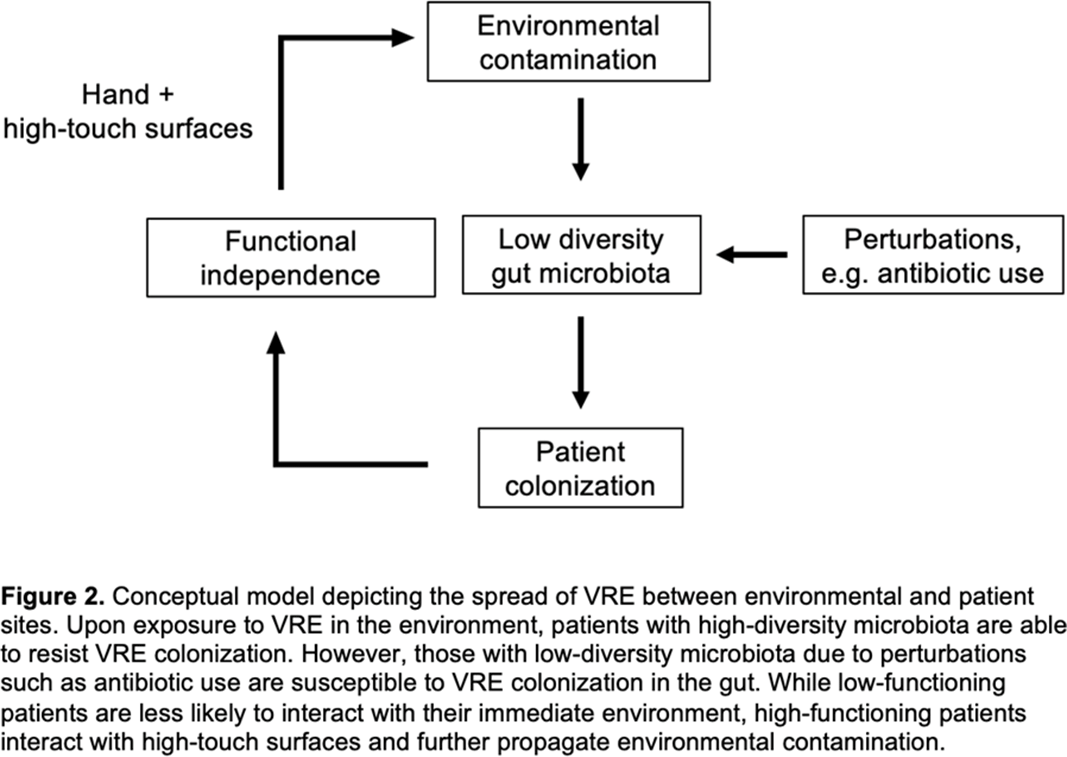
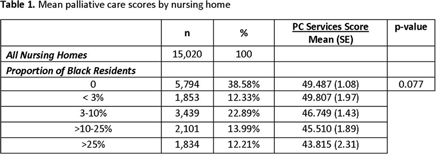
Background: Infections are common at end-of-life in older nursing-home residents. This often leads to the overuse of antibiotics and burdensome treatments. Improving infection management through palliative care at the end of life has been proposed as a key strategy to reducing inappropriate antibiotic use. Black nursing-home residents tend to reside in poorly performing nursing homes. We examined palliative care services in nursing homes with varying proportions of black residents. Methods: Cross-sectional, nationally representative nursing-home survey data (2017–2018) was combined with the Minimum Data Set 3.0 (nursing-home resident characteristics), the Certification and Survey Provider Enhanced Reporting data (nursing-home facility characteristics), and the Multidimensional Deprivation Index (county-level poverty estimates). The survey included 24 validated items on nursing-home palliative care services, as well as the nursing home’s infection control program and integration of infection management and palliative care (summative score, 0–100). We used nursing-home facility-level multivariate regression to estimate the relationship between proportion of black residents and palliative care scores, before and after controlling for county-level poverty estimates, facility characteristics, and resident characteristics. We categorized proportion of black residents using methods reported in the literature (25%). Results: The mean weighted palliative-care score in our sample of 869 nursing homes (weighted n = 15,020) was 47.7 (SE, 0.70). In unadjusted analyses, nursing homes with higher proportions of black residents provided significantly fewer palliative care services than nursing homes with no black residents, with the greatest differences (P = .027) observed between nursing homes with >25% black residents (mean palliative care score, 43.82; SE, 2.31) versus nursing homes with no black residents (mean palliative care score, 49.47; SE, 1.08). These disparities persisted after adjustment for urbanicity and county-level poverty rates (p < 0.01) but were attenuated after further adjustment for resident and facility level characteristics (p=0.138). Conclusions: Our findings demonstrate that wide variations in nursing-home palliative-care services exist with increased proportions of black residents, even after accounting for community characteristics. Further research is needed to identify and understand the specific community characteristics that play a role in the provision of palliative care services. Palliative care is a method to reduce inappropriate antimicrobial use at the end of life and should be expanded with a focus on nursing homes with higher proportions of black residents.
Funding: No
Disclosures: None
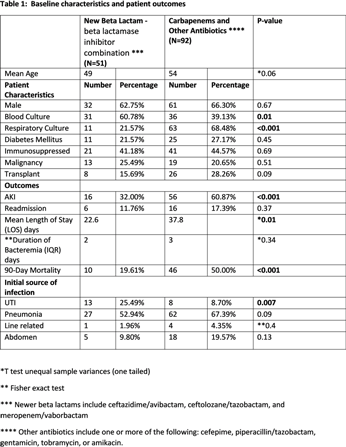
Background: Data on the patient outcomes for newer β-lactam–β-lactamase inhibitor (BLBI) drugs compared to carbapenem-containing combination antibiotics for multidrug-resistant (MDR)–Pseudomonas aeruginosa infections are limited. Methods: This retrospective, case–control observational study was based on chart review of the patients managed at the University of Kentucky. Results: In total, 143 patients with MDRO Pseudomonas aeruginosa infections were identified and divided into 2 groups: 1 group received newer BLBI combinations with or without aminoglycosides or polymyxins, for at least 72 hours, and the control group received carbapenem containing combination antibiotics or other antibiotics. Baseline characteristics and patient outcomes are shown in Table 1. Discussion: The newer BLBI combinations group consisted of 60.8% MDR Pseudomonas bacteremia, whereas the control group had 68.4% of MDR Pseudomonas respiratory cultures. Overall, the use of newer BLBI combinations such as ceftazidime/avibactam, ceftolozane/tazobactam, and meropenem/vaborbactam was associated with lower rates of acute kidney injury (AKI), shorter LOS, and lower mortality rates compared to the control group, and these differences were statistically significant. Because the 2 populations of patient differed significantly based on the site of infection (sepsis vs pneumonia), the data were reanalyzed to evaluate the impact of therapy on the occurrence of AKI, LOS, and mortality based on the site of infection. Only those patients with sepsis who received the newer combination drugs had significantly better rates of AKI, lower LOS, and had lower rates of mortality. The 2 treatment arms were not statistically different when comparing patients with pneumonia. Additionally, the use of these new combination therapies did not make a difference regarding readmission rates or duration of bacteremia for the patients included in the study.
Funding: No
Disclosures: None

Background: The Centers for Disease Control and Prevention reported 32,600 cases, 2,700 deaths, and healthcare costs of 767 million dollars attributed to multidrug-resistant Pseudomonas aeruginosa. A recent study of 128 patients with nosocomial pneumonia due to P. aeruginosa showed the noninferiority of ceftolozane-tazobactam compared to meropenem. However, the resistance of ceftolozane-tazobactam due to AmpC mutations has been described. Compared with 2019, we observed an increase from 2 to 13 cases of ceftolozane-tazobactam–resistant P. aeruginosa (CRPA) during the COVID-19 pandemic at our institution in the Bronx, New York. Methods: A report of patients with CRPA between March and August 2020 was obtained. Data collected included demographics, hospitalization/IV antibiotic use in prior 90 days, SARS-CoV-2 PCR result, ICU admission, length of stay, antibiotic days of therapy, mortality, etc. Results: In total, 13 patients with CRPA infection were reviewed (Table 1). Among them, 2 patients were on the same inpatient medical-surgical unit but separated by 5 months. Also, 11 patients were from different medical-surgical units or ICUs. In addition, 5 patients (38%) were SARS-CoV-2 PCR positive. None of these COVID-19 patients were cohorted on the same unit, making horizontal spread of CRPA or COVID-19 unlikely. Finally, 8 of these patients died while hospitalized (4 were COVID-19 patients). Conclusions: We found a high incidence of mortality in patients with CRPA infection. Many patients had prolonged hospital stay and required ICU admission. Few patients were from long-term care facilities. Given the associated morbidity and mortality, increased surveillance and intensified antimicrobial stewardship efforts are needed to mitigate the impact of CRPA during the COVID-19 pandemic.
Funding: No
Disclosures: None